
Abstract
Background
Early detection of autism spectrum disorders (ASDs) is essential given the under-reported cases in low- and middle-income countries. This first national representative survey was conducted to explore the prevalence of ASDs amongst 18 and 30 months in seven provinces in Vietnam.
Design and methods
During 2017-2018, a national cross-sectional and population-based survey for autism spectrum disorder (ASD) amongst 40,243 children aged 18 to 30 months was conducted in 7 provinces representing the socio-economic regions of Vietnam. M-CHAT was used to screen children and then confirmed by diagnostic assessment using DSM-IV criteria.
Results
The prevalence of ASDs amongst children aged 18 and 30 months in Vietnam was high (0.758% or 1 in 132 children). Urban setting, male gender, and hereditable genes were associated with ASD prevalence.
Conclusions
ASDs amongst children aged 18 and 30 months in Vietnam tend to be increasing and are similar to this rate in other middle-income countries but lower than that in Western countries. This under-recognized public health problem amongst children should be addressed by early detection and intervention for families with affected children.
Introduction
Autism spectrum disorders (ASDs) are the greatest burden of life-long neurodevelopmental disorders in children and adolescents with an estimated prevalence of 62/10,000 children worldwide. 1,2 ASDs are characterized by ‘impaired social behavior, communication and language, and a narrow range of interests and activities that are both unique to the individual and carried out repetitively’. 3 Although accurate and representative numbers are difficult to obtain, empirical studies in the last 50 years show that prevalence of the ASDs appears to be increasing significantly worldwide.1,2 The reasons of this rapid increase are still not known. 4
Significance for public health
This first nationally representative and population-based survey adds empirical data about autism spectrum disorder (ASD) amongst children aged 18 to 30 months in Vietnam. Using M-CHAT as screening tool and DSM-IV criteria for confirmation, ASD amongst children aged 18 and 30 months shows an increasing trend with the prevalence as high as 0.758% in 2018. Early detection and intervention should be conducted to provide affected child with the potential for a better life.
The number of children with ASDs in low- and middleincome countries are under-reported. 3 To date, no nationally representative population-based survey of ASDs has been conducted in Vietnam. Previous small-scale studies show an increase trend of ASD cases from three-fold in a 7-year cohort study5,6 to four-fold in another 3-year cohort study.7 Early detection of ASDs is of utmost importance, particularly given the growing numbers of cases, high level of morbidity and impairment, financial burden, and better outcomes for interventions. Early detection often applies qualitative tools to assess behavioral patterns due to no definitive biological markers.8,9
The first signs and symptoms of ASDs could be observed during the first 12 to 18 months of life.10,11 The screening for ASDs is recommended for all children aged 18 months or older. 12 In Vietnam, there has currently no large-scale study using validated tools to investigate the prevalence of ASDs. We, therefore, conducted this national representative survey to explore the ASD prevalence and its association with socio-economic status, parental characteristics among children aged 18 and 30 months in seven provinces in Vietnam.
Design and methods
Design, study setting, and sampling
This cross-sectional survey applied population-based survey. In the first stage, we selected Hanoi (capital of Vietnam) and 6 provinces representing the typical characteristics of the six socioeconomic regions in Vietnam (pursuant to the Decree No. 92/2006/ND-CP in 2006 on the master plan on socio-economic of Vietnam). The six provinces were Thai Binh, Hoa Binh, Quang Nam, Dong Nai, Dong Thap, and Dak Lak.
For the second stage, based on multistage sampling strategy, in each selected city/province, one urban district and two rural districts were randomly chosen. As such, the survey was conducted in 21 study sites (7 urban and 14 rural districts) in seven cities/provinces in Vietnam during 2017-2018.
For the third stage, in each selected district, about 2,000 children aged 18 to 30 months were chosen randomly from the full list of children with the same age. Therefore, a total of 6,000 children were chosen in each city/province. The list of potential participants was provided by the District Health Center.
Sample size
In each district, the sample size of children aged 18 and 30 months was calculated by estimating a population proportion with specified relative precision:

Where: n is total number (sample size); z(1- α/2) is 95% confidence interval (CI); ɛ is relative precision (35%); p is anticipated proportion of children with ASDs (0.46%) in the population based on prior studies. 13 The final sample size for each province, assuming a maximum refusal rate of 15%, was 5,918 children aged 18 and 30 months. Therefore, for all seven cities/provinces, the total sample size of this study was 42,551 children.
Measurements of ASD
Phase 1: Screening
After a thorough review of different ASD screening tools, the Modified Checklist for Autism in Toddlers (M-CHAT) was utilized for the screening phase of our study.13,14 This tool was also the most common and easy-to-use for early ASD screening in children aged 16 and 30 months in both primary and tertiary health facilities. 15,16 However, the American Academy of Pediatrics (AAP) has issued guidelines for ASD screening at 18 and 24 months since there had evidence for efficacy of screening in community settings. 17 M-CHAT is a self-administered parental questionnaire consisting of 23 (yes-no) items. 18 The M-CHAT is available in at least 22 languages including Vietnamese. 19 Validation studies show the positive predictive value (PPV) of M-CHAT varies from 0.57 to 0.65 in low-risk samples.20–22 From a public health perspective, using M-CHAT improves early ASD detection for the entire population while being an easy-to-perform and low-cost tool.22–24 In Vietnam, M-CHAT is the main screening tool for children 16-30 months used in both primary and tertiary hospitals with a higher PPV (0.7583) 13 than the PPV in other high-income countries. 21,23,25 In our study, M-CHAT-R/F was not chosen as these tools require much more time and resource for follow-up screening. All screenings were conducted by a trained health staff with the participation of the children's parents and/or caregivers.
Phase II: Comprehensive diagnostic assessment
Phase II aimed to confirm the ASD among the selected group of children already considered to be at high risk, that is, children with positive-screening result. These screen-positive children were invited for a further comprehensive diagnostic assessment. We used DSM-IV for diagnosis of ASD because it has been widely used in Vietnam and other countries. 26 The newer version, DSMV, introduced in 2013, has not yet been tested in Vietnam. 4 For each screen-positive child, two screen-negative children matched on major socio-economic factors (e.g., age group, sex and healthcare setting), were randomly selected and invited for a further assessment. As recommended by the AAP, 12 a multi-disciplinary team, composed of a neurologist and a child psychologist, performed the comprehensive diagnostic assessment for the study. Eight professionals from Department of Psychiatry, National Hospital of Pediatrics were recruited. These professionals were experienced experts in ASD diagnosis and intervention. The team performed an ASD diagnostic assessment, identified the mimic ASD or comorbid conditions, and determined functional levels of all participants. The average length of time for the diagnosis ranged from 40 minutes to 1 hour.
Data collection
In each district, about 15 local staff of the commune health centers (medical doctor, nurse, and/or midwives) were recruited and trained. Data collectors conducted face-to-face interviews with the children's parents and/or caregivers. Besides 23 items of MCHAT, the questionnaire included questions regarding sociodemographic information and history of maternal pregnancy
For data monitoring and supervision in each district, a team of three or four supervisors was trained from the multi-disciplinary team. Supervisors oversaw the entire process of data collection and validated all screen-positive cases through additional interviews with the children's parents. After confirmation, the multi-disciplinary team invited the children and caregivers to the district health center and performed the comprehensive diagnostic assessment. After discussing and reaching diagnostic consensus, the team concluded the ASD status of each child using DSM-IV criteria. A few children was lost to follow up. 19 positive-screen cases and 241 negative-screen cases were not collected due to refusal of parents or their absence at the time of data collecting.
Study variables
The dependent variable was ASD status (initially identified by M-CHAT test and subsequently diagnosed by the multi-disciplinary team). Independent variables were socio-economic status (SES) divided into three groups: i) socio-demographic information of the children (province, age group, sex, and setting), ii) parental characteristics (age at the time of childbirth and occupation), and iii) hereditable genes (having relative with mental disorder or genital anomalies). Age group of the children was dichotomized into 18-23 months and 24-30 months. Parents’ age was classified into four different groups (<20 years, 20 to 29 years, 30 to 34 years, and ≥35 years for mother; and <20 years, 20 to 34 years, 35 to 45 years, and ≥46 years for father). Parents’ occupation included government staff, private sector staff, farmer, unstable job, and others.
Statistical analysis
All data analysis was performed using Stata 14. Univariate logistic regression was to explore the associations between independent variables and the outcome measure (ASD status) among children aged 18 and 30 months. Next, multivariable logistic regression models were applied to minimize the potential confounding effects. A p-value <0.05 was considered significant.
Ethical considerations
The study was approved by the Institutional Review Board of Hanoi University of Public Health (Decision 319/2016/YTCCHD3 dated 16/Dec/2016). Prior to participation, all respondents were asked to sign informed consent documents. Respondents were informed they could refuse to participate or withdraw from the interview at any time without any recourse.
Results
A total of 40,243 children (94.5% of those approached) agreed to participate in the study and completed the face-to-face interviews (Figure 1). Of the 40,243 children who had M-CHAT screening, 514 screen-positive cases (100%) and 1028 screen-negative cases (2%) were further diagnosed using DSM-IV criteria. There were 19 positive cases and 241 negative cases with M-CHAT of loss to follow- up due to refusing to diagnose, moved to another province, the child was absent at the time off diagnosis. A total of 305 confirmed cases was diagnosed (302 cases/495 positive-screening children and 3 cases/787 negative-screening children). The overall prevalence of ASDs among children aged 18 and 30 months in 7 cities/provinces was 0.758% or 1 in 132 children.
Both children's and their parents’ characteristics are presented in Table 1. There were slightly higher numbers of boys than girls and more than half (57.3%) of the children were 24–30 months. Three-fourths of children (75.2%) lived in rural areas.
In term of parental characteristics, most of the mothers (90.5%) were aged less than 34 years old and most of the fathers (95.4%) were aged less than 45 years old. The highest group of occupation was unstable job (28% of mothers and 40% of fathers), next to private sector staff (25.4% of mothers and 21.4% of fathers). About 3.6% of children had a relative with mental health disorder or genital anomaly.
Table 1 also presents the prevalence of ASDs among children aged 18 to 30 months by independent variables. The provinces of Ha Noi, Dong Nai, and Quang Nam had the highest prevalence of ASDs, 0.84%, 0.84%, and 0.81% respectively. The prevalence of ASDs was significantly higher in boys (three times higher than that in girls - OR=3.65, 95% CI: 2.75–4.84), children living in urban areas (about 2.7 times higher than that in rural areas OR=2.67; 95% CI: 2.13–3.34). In addition, the prevalence of ASDs was significantly higher among older parent (highest among mothers aged ≥35 and among fathers aged ≥46).
Table 2 presents the multivariable logistic regression to test the association of socio-economic status and parental characteristics with ASD. After controlling for all other variables in the model, the odds of having ASD were significantly higher among: i) children living in urban than in rural areas (OR=2.8, 95%CI: 2.2–3.5); ii) boys as compared to girls (OR=2.6, 95% CI: 2.0–3.4); iii) mothers aged ≥35 (OR=1.7, 95%CI: 1.2–2.4); iv) children who have a relative with mental health disorder or genital anomaly (OR=3.6, 95%CI: 2.6–4.8).
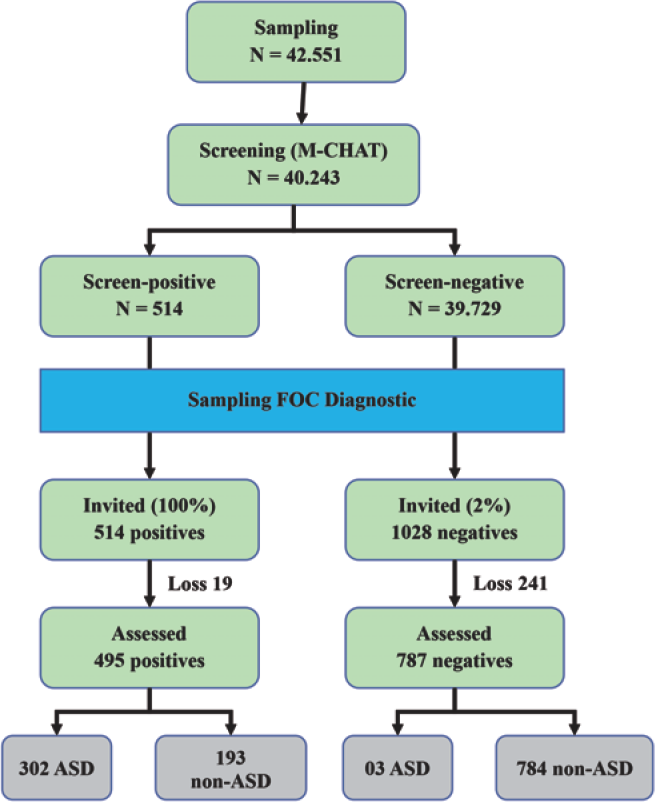
Screening and diagnostic process.
Discussion
To the best of our knowledge, this is the first epidemiological, nationally representative, population-based survey on autism spectrum disorders (ASDs) in Vietnam. The survey was conducted by implementing a two-step ASD diagnostic procedure: Phase I using M-CHAT to identify high-risk children in the general population, and Phase II using comprehensive diagnostic assessment criteria (DSM-IV) to confirm the ASD diagnosis. The overall ASD prevalence in children aged 18 and 30 months is 0.758%, that is, 1 in 132 children. Our finding is similar to the estimate of ASD prevalence in other low- and middle-income countries such as China,1,2,4 but slightly lower than that rate in high-income countries such as Canada (1.59%), 27 US (1.68%), 28 Japan (1.8%). 8 Furthermore, our results indicate a much higher prevalence reported by previous small-scale in Vietnam such as 0.46% in National Hospital of Pediatrics in 20075 or 0.50% in 2014. 14 This suggests that ASD should be recognized as a fast-growing issue of national public health concern in Vietnam. Therefore, ASDs are one of the greatest burdens of disease amongst children in Vietnam. The government and relevant stakeholders in Vietnam should prioritize actions to address the developmental and mental health needs of affected children and their families.
In Vietnam, routine screening for ASDs in both low- and highrisk children does not exist. As M-CHAT screening is collected from parents and/or caregivers of the children, self-administered survey could provide inaccurate information if their children are thought to be low risk for ASDs. Furthermore, the completion rate is low even in high-risk populations. 29 As such, it is challenging to collect accurate data from parent self-administered instruments and the data may be less reliable. In line with other countries, Vietnamese parents prefer face-to-face interviews to self-administered interviews. This has been documented in the previous surveys of M-CHAT in Turkey 30 and Thailand. 31 To address this concern, in our study, trained health staff were recruited to conduct face-to-face interviews with the parents to improve the diagnostic predictive power, which is recommended in both high- and lowrisk children.21,32,33 For future studies in Vietnam, we recommend to apply the screening process by semi-structured interviews to improve overall sensitivity and specificity of the M-CHAT. This suggestion is also highlighted in other studies in Thailand 31 or South Korea. 34
Due to the large sample size, follow-up interviews to improve the PPV and minimize the false-positive results of the M-CHAT for both general population and for high-risk individuals are not feasible.21,33,35 A follow-up interview after screening in primary care settings could be helpful in reducing false-positive cases. Besides, high-risk children with developmental disorders should be referred to specialized health facilities.20,22 The M-CHAT-R/F is recommended for use as a follow-up interview as it has been demonstrated to help reduce the number of false-positive cases and to have a higher identification rate compared to M-CHAT. 32
In low- and middle-income countries, ASDs are not well-recognized by the general public and sometimes even the government. 3 Early detection of ASDs in young individuals in low- and middle-income countries is very challenging since most of ASD screening tools are not feasible in scarce-resource settings. Time constraint is also a barrier for the widespread use of screening tools, including M-CHAT.7,31,36 In addition, further training should be conducted to ensure the understanding of each item in M-CHAT tool which depends on local context and cultural background of each area.7,18,33
In terms of socio-demographic characteristics of the children, as expected, geographical representation and sex are strongly associated with the prevalence of ASDs. The odds of a boy being diagnosed with ASDs are approximately 3 times higher than that of a girl. This result is in line with the previous studies in other settings.37–41 Another associated factor is the setting of the children, in which, children living in urban areas are 2.7 times more likely to have ASDs than that of children living in rural areas. This is also reported in previous studies.42,43 A potential explanation is that urbanization could increase exposure to air pollutants and microbial agents during pregnancy and early childhood which are the risks for ASD. 43
Socio-economic status, parental characteristics and their association with autism spectrum disorders (ASD) in children aged 18 to 30 months.

Result from univariate logistic regression
statistically significant at p<0.01
statistically significant at p<0.001.
Multivariable logistic regression analyses of socio-demographic variables for association with autism spectrum disorders (ASD) in children aged 18 to 30 months.

Result from multivariable logistic regression after adjusting for other variables in the model
statistically significant at p<0.05
statistically significant at p<0.01
statistically significant at p<0.001.
Maternal and paternal characteristics are found to be associated with an increased risk of having ASDs amongst children aged 18 to 30 months. Advanced maternal and paternal age at the time of delivery is associated with higher risk of ASDs. Mothers ≥35 years-old have 1.4 times higher odds of their child having an early ASD diagnosis than that of mothers <35 years old. This finding is consistent with previous reports that younger mothers are less likely to have children with ASDs. 41
Strengths of the present study include the use of a carefully assessed using a nationally representative population sample of children with ASDs. A structured interview approach was used to reduce variability and increase reliability of the ASD diagnosis. All interviewers were trained and closely supervised by the corresponding author to establish reliability among interviewers and to ensure that all interviews were conducted following a strict protocol. Our results could be generalized to the entire population of Vietnam. However, the stigma of the local residents to children with ASDs and their parents/ caregivers could create biases during data collection.
Conclusions
The prevalence of ASDs amongst children aged 18 and 30 months in Vietnam (0.758%) showed a significant increasing trend. This rate is similar to estimates in other middle-income countries but lower than that of the Western countries. The significant correlates of ASDs among the children were urban setting, and male gender. While the underlying causes of ASDs among children in Vietnam could not be investigated in our study, addressing this under-recognized public health problem is essential. A need for major interventions in healthcare and education systems should be performed to support the affected children and their families. There is also a clear need to develop effective surveillance system to detect by early screening, diagnosis, and interventions for children with ASDs in Vietnam.
Footnotes
The authors declare that they have no competing interests, and all authors confirm accuracy.
Acknowledgements
We would like to thank data collectors and the participants in this study, as well as Department of Health in Hanoi, Thai Binh, Hoa Binh, Quang Nam, Dong Thap, Dong Nai, Dak Lak for supporting us to implement this study. We also send thank to Ministry of Science and Technology, Vietnam for providing both technical and financial support to the study.