
Abstract
Background
Globally, unintentional injury has been a documented public health problem among adolescents having debilitating consequences and accountable for economic burden. The study was undertaken to estimate the prevalence of unintentional injury, identify the determinants and consequences among adolescents.
Design and methods
This cross-sectional study recruited 222 adolescents using systematic random sampling from a site covered under UHTC Srinagar Garhwal, Uttarkhand. Binary and multivariate logistic regression was used to compute crude and adjusted odds ratio (95% CI) for establishing an association between risk factors and unintentional injury. Descriptive measures (causes, consequences, etc.) describing injuries were presented in tabular, graphical form in proportions.
Results
73.1% of the adolescents suffered from unintentional injury. The risk factors associated (statistically insignificant) with unintentional injury was males (AOR=1.019, 95% CI=0.524-1.979), living in nuclear family (AOR=1.540, 95% C =0.766-3.093), smoked tobacco (AO=2.797, 95% CI=0.227-34.4377), visually impaired (AOR=1.629 95% CI=0.548-6.458) and living in house with overcrowding (AOR =1.66, 95% CI=0.818-3.395). Five percent of those affected with unintentional injury had disability.% of those affected with unintentional injury had disability.
Conclusions
Health education addressing causes, risk factors, consequences of unintentional injury among adolescents, parents, school, and district health authorities should be mandated for the formulation of policy to prevent unintentional injuries.
Significance for public health
Adolescence is often a period of life that connects adolescence to maturity and is marked by significant physical, psychological, and social changes. The country's changing disease profile is profoundly embedded in the country's recent social, fiscal, and environmental developments. The cost of adolescent accidental injury to the country is rising as a result of damage and death. As a result, avoiding accidental accidents is crucial. More evidence on the overall costs and benefits of injury prevention is also required. This will assist governments in prioritising investments, and it is a subject on which leading scholars and organisations will collaborate. Injury prevention can be low-cost, with a high return on investment in terms of preventable years of life loss and disability-adjusted life years for young children.
Introduction
Unintentional injuries are a public health challenge around the world causing physical, psychological, and economic implications to families and society. 1 Globally the leading cause of unintentional injury worldwide is road traffic accidents, 2 followed by falls, 3 drowning, 4 burns, poisoning, 5 and others. Domestic accidents 6 and animal bite injuries further add to the burden of unintentional injuries. 7 The worldwide rate of unintentional injuries is 61 per 100,000 population per year 2 and causes 10% of the total annual deaths. 5 In India non-fatal unintentional injury rates as high as 342/1000 children. 8 Unintentional injuries may have long-term consequences of disability. Road traffic and other unintentional injuries account for 0.9 DALYs/1000 capita, per year in India. 9
The factors associated with the occurrence of unintentional injuries are demographic factors, i.e age, gender, Socioeconomic factors, i.e low income, and overcrowding. 10 Young adults are at high risk of unintentional injury caused by alcohol drinking and substance use (tobacco and cannabis use). 11 People with psychological distress are more likely to suffer from unintentional injuries. 10 Medical conditions, such as neurological, cardiac, or other disabling conditions; poor mobility, cognition, and vision, are other risk factors for unintentional injuries. 3
A review of the literature revealed a paucity of comprehensive health research among the hilly population of India. Most of the studies are isolated and fragmentary and focus on single injury, children, and are hospital-based. The actual burden of unintentional injury may have been significantly underestimated. There is an immediate need to address the risk factors contributing to unintentional injury. The need to address issues arising out the actual burden of unintentional injury, contributing risk factors and associated consequences among adolescents and lack of studies in the hilly population of Srinagar, Garhwal, Uttarakhand are the three main reasons for undertaking this study.
Design and Methods
This cross-sectional study was conducted in Srinagar Uttarakhand under the Urban health training center from August 2017 to December 2017 using systematic random sampling recruited residents aged 10 to 19 years living in the study area for the last six months and assent/consent given by their parents. The study excluded participants who were not available for three consecutive visits. According to Census 2011, it has nearly 20000 total population. 12
The formula used for sample size calculation is n=4pq/d 2 . 13 The sample size was calculated based on the prevalence of unintentional injuries in the Indian population. For the calculation of the sample size, the prevalence of unintentional injuries was taken to be 17.4% as per a study from Pune City, Maharashtra, India. 14 The sample size came to be 229 after taking 5% precision and 95% confidence level. A simplified questionnaire was designed based on a review of literature, for measurement of the prevalence of unintentional injuries, risk factors like demographic factors, socioeconomic factors, behavioral factors, pathological factors, and others, and consequences of unintentional injuries. The information was documented after receiving the informed consent and assent form.
Adolescents in Srinagar's population were systematically sampled. After a random starting point between 1 and 10, the nth house was selected. The research included all of the people who were eligible in a given household. Before beginning the interview, the Investigator introduced herself/himself to the research subject. An information sheet was provided to parents/caregivers/participants explaining the report, its goals, protocol, and the participants’ rights. After reading the information sheet, if the parents/caregivers/ participants wished to participate in the study, written consent was obtained from the parents/caregivers and assent was obtained from the participants. The participants in the research were interviewed following the interview protocol. This was carried out at the participant's residence, preferably outdoors in the daytime. The survey continued until the full sample size is close to being reached.
The outcome variables were indicators used were prevalence (%) of unintentional injuries in the last one month, three months, and one year. In addition, consequences of unintentional injuries were studied in terms of disability. The explanatory variable taken into account were demographic factors (age, gender, and others), socioeconomic factors like (education, family type, overcrowding, etc.), behavioral factors (alcohol or tobacco use), and pathological factors (presence of impaired vision, hearing, etc.)
As per our operational definition, the following variables were defined as: i) unintentional injury defined as an injury that occurred because of traffic accident, falling, near drowning, poisoning, burns, or animal biting; ii) tobacco/alcohol use will be defined as smoking /smokeless tobacco/alcohol use at least once during the past 30 days; iii) impaired vision is referred to a person who cannot count fingers at a distance of six meters, or a known case of refractive error or other; iv) impaired hearing is a person's inability to repeat the whispered words or a known case of deafness.
All the data was entered into Microsoft Excel 2010 and analyzed using SPSS 17. Descriptive statistics were done for causes of unintentional injury and place of occurrence of injury, presence of disability and displayed in bar and pie charts. Moreover, tabular description for an injury like the mechanism of injury, body part injured, nature of the injury, and severity of the injury was done. Bivariate analysis was done between the presence of unintentional injury and explanatory variables to compute unadjusted odds ratio (95% CI) and variables who were significant (p<0.20) were taken into multivariable analysis for computing adjusted odd ratio (95% CI). Ethical clearance was taken from the Institute Ethics committee.
Results
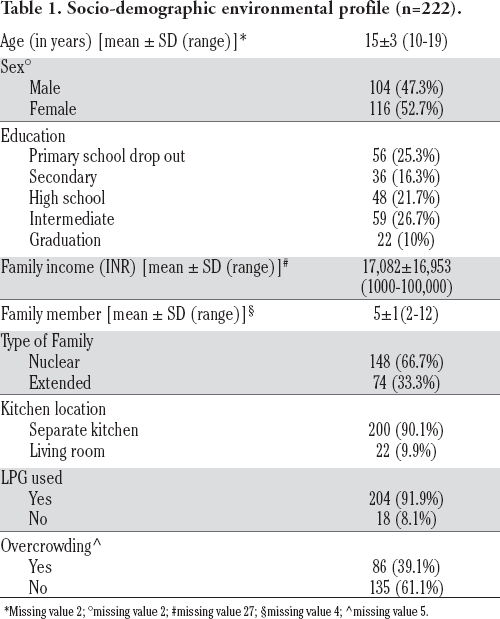
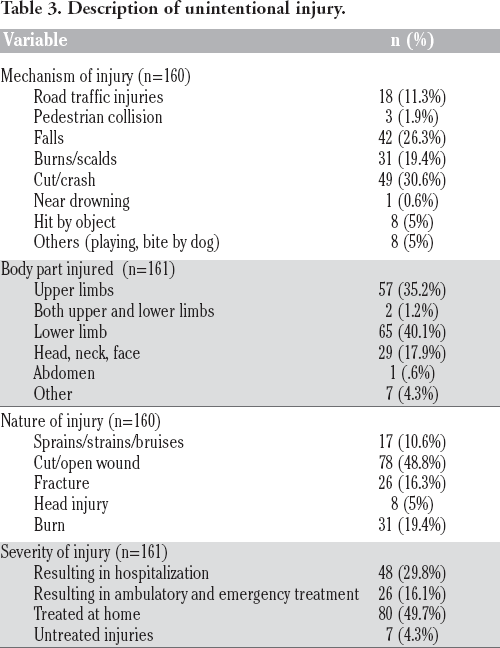
The mean age of the participants was 15±3 years with a mean family income of Rs.17082±16953 and with a mean family number of 5±1. The majority of the participants were female (52.7%), primary school dropout (25.3%) belonging to the nuclear family (66.7%), living in a home with a separate kitchen (90.1%), access to LPG (91.9%), and presence of overcrowding in their home (39.1%) (Table 1). Of 173, 18.5% incurred an unintentional injury in the last one month, 19.8% in the last three months, and 21.6% in the last year. Overall, of 220 participants, 161 suffered an unintentional injury. The odds of unintentional injury per unit increase in age is 1.071 (0.792–1.494) and less in age category 10-15 years (AOR =0.380, 95% CI =0.093-1.560) in comparison to 16-19 yrs. Further, the odds of unintentional injury were lower in primary school dropout (AOR =0.245, 95% CI =0.039-1.559), secondary school (AOR =0.202,95% CI=0.042-0.974), high school (AOR = 0.635,95% CI=0.189-2.938), intermediate (AOR = 0.597, 95% CI =205-1.739) in comparison to graduate students. The odds of unintentional injury was higher in males (AOR =1.019, 95% CI=0.524-1.979), living in nuclear family (AOR = 1.540, 95% CI=0.766-3.093), smoked tobacco (AOR = 2.797, 95% CI=0.227-34.4377), vision impairment (AOR =1.629 95% CI=0.548-6.458) and living in house with overcrowding (AOR =1.66,95% CI=0.818-3.395) but less in hearing impairment (AOR =0.434 95% CI=0.066-2.863) (Table 2). Of 155 participants who incurred unintentional injury, 44.5% were engaged in sports activity, 30.3% involved in domestic studies, 2.6% in leisure activity, 6.5% faced injury during resting, sleeping, and eating, 1.3% working for income, and 14.3% incurred injuries while involved in other activities. Of 158 participants who incurred unintentional injury, 28.5% were alone during the injury. Cut/crash injuries accounted for 30.6% of all unintentional injuries, accompanied by falling (26.3%), burns (19.4%), road traffic injuries (11.3%), hit by an obstacle (5%), bicycle impact (1.9%), close drowning (0.6%), etc.; 40.1% of the 161 participants who sustained an accidental injury did so in the lower limb, led by 35.2% in the lower limb, 17.9% in the head, neck, and face, and 1.2% in both the upper and lower limb. Of 161 participants suffering an unintentional injury, 49.7% were treated at home followed by 29.8% in hospitalization, 16.1% in ambulatory and emergency treatment, and 4.3% were untreated (Table 3). Of 152 who suffered an unintentional injury, 41.4% were due to falling followed by poisoning (19.7%), traffic accidents (14.5%), burns (11.8%), animal biting (9.9%), and 2.3% each near-drowning and choking (Figure 1).

Cause of unintentional injuries among adolescent (n=152).
Socio-demographic environmental profile (n=222).
Missing value 2
missing value 2
missing value 27
missing value 4
missing value 5.
Determinants of unintentional injury among adolescents.

Description of unintentional injury.
Of 160 suffering unintentional injury, most of the injury occurred at home (48.8%) followed by residential institution (17.5%), sports, athletic area (15.6%), school, public administration area (10.6%) street and highway (3.1%), farm (1.8%), industrial construction area (1.5%) and trade and service area (0.6%) (Figure 2). Of 158 who suffered an unintentional injury, 5.1% resulted in a disability.

Place of occurrence of unintentional injuries among adolescent (n=160).
Discussion
Nearly three-fourths of participants suffered an unintentional injury. Unintentional injury was higher among adolescents who were in the age group 16 to 19 years, graduates, males, living in a nuclear family, smoked tobacco, vision impairment, and living in a house with overcrowding. A quarter was hospitalized and one-fifth was in ambulatory and emergency treatment.
Ainey et al. study among 727 high school students revealed 44% of boys and 38% of girls were exposed to risky behaviors leading to unintentional injuries. 15 Ok and Sung's study among 68,043 adolescents from 7th to 12th-grade findings show 22.9% of the adolescents had treatment experiences for unintentional injuries at school in the past 12 months and the significant factors associated with unintentional injuries at school included gender, grade, academic achievement, current smoking, alcohol consumption, frequency of high caffeine intake, depression, and relief of fatigue after sleep. 16 Fernandez et al. on evaluating the Spanish National Health Survey highlighted boys suffered unintentional injuries 1.64 more times than girls (OR=1.64; 95% CI=1.48-1.82) and adolescents aged 15-18 years (OR= .24; 95% CI=1.07-1.42) had a higher probability of reporting an unintentional injury when compared to children aged 6-10 years. 17 Shi et al. on conducting a cross-sectional study in three main colleges in Wenzhou, China found falls were the leading cause of unintentional injury, followed by traffic injuries, animal/insect bites, and male students were more likely to be injured than female students. 18
ASEAN 2019, a study among 29,480 school adolescents of secondary schools studying in Lao, Philippines, Thailand, and Indonesia indicates the proportion of participants with one or multiple serious past one year injuries was 36.9% (21.4% once and 15.4% multiple times). The following factors - male sex, experiencing hunger, substance use (alcohol, tobacco, cannabis, amphetamine, and soft drinks), school truancy, participating in physical education classes, and psychological distress were associated with unintentional injury. 19 Wickramasinghe et al.’s study among 3262 adolescents attending government school in Sri Lanka findings highlight 35.8% of the students reported being seriously injured one or more times. Being male sex, bullied, physically attacked, or being in a physical fight were associated with unintentional injury. 20 Ssemugabho et al. study among 1583 children from Ugandan slum community between 6 months of age and 18 years revealed 706 had suffered 787 unintentional injuries. 21 Mathur et al. study among 6308 children up to 18 yrs belonging to slum areas of Ujjain findings indicate the annual incidence of all injuries was 16.6%, the incidence was significantly higher among boys compared to girls (20.2% versus 12.7%, respectively), was highest in age group 6-10 years of age (18.9%), and urban locations (17.5%). 22
In our study, around three-fourth of the participants suffered an unintentional injury and the odds of unintentional injury were higher in males, living in a nuclear family, smoked tobacco, vision impairment, and living in a house with overcrowding but statistically insignificant association.
Cause and common form of injury
In Malaysia study among 21,699 school-going adolescents revealed two major causes of the most serious injury were fall (9.9%) followed by a motor vehicle accident or being hit by a motor vehicle (5.4%), and the most frequent type of injury sustained was cut, puncture, or stab wound (6.2%) and a broken bone or dislocated joint (4.2%). 23 Similarly, the ASEAN 2019 study among school adolescents of secondary schools studying in Lao, Philippines, Thailand, and Indonesia indicate the most frequent cause of the reported injury was fall (10.2%) and motor vehicle (5.8%). The most common form of injury was a broken bone or dislocated joint (8.1%) and cut, puncture, or stab wound (3.4%). 19 The most common type of injury among 3262 adolescents attending government school in Sri Lanka was cut or stab wounds (5.5%), followed by broken bones/dislocated joints (5.3%). 20 An Uganda 2018 study among 1583 children (between 6 months and 18 years old) from Ugandan slums reported commonest injuries were cuts, bites, or open wounds (30.6%) and bruises or superficial injuries (28.6%) with the majority (75.5%) occurring at home.21. The most commonly identified injury types among 6308 children up to 18 years belonging to slum areas of Ujjain was physical injuries (71%), burns (16%), poisonings (10%), agriculture-related injuries (2%), near drowning (2%), and suffocations (2%). The most commonplace of injury was streets followed by home. 22
In our study, the most like the cause of injury were cut/crash (30.6%), falls (26.3%), burns (19.4%) and road traffic injuries (11.3%), etc. and the most common form of injury were cut/open wound (48.8%) followed by 19.4% burn, 16.3% fracture, and 5% head injury.
Activity and place of injury
The most commonplace of injury are either home or house yards or schools or streets.21-23 Similarly, our study reports, nearly half of the injury occurred at home followed by residential institutions, sports, and athletic areas, school and public administration area, street and highway, etc. The activity during which injury usually occurs has been reported to be walking or running (17.24%), biking (11.4%), motorcycle driving, and road racing (10.37%) in an Iranian study among 13486 elementary, secondary, and high school students. 23 In our study, most of the unintentional injuries were during sports activity (44.5%), domestic studies (30.3%), 6.5% faced injury during resting, sleeping, and eating, etc.
In addition to the previous study, the study assessed the presence of disability in an injured adolescent. The findings of the study should be cautiously interpreted because it was conducted in a single setting despite the random selection of the participants.
Conclusions
Unintentional injury is prevalent among adolescents in the hilly terrain of Srinagar, Uttarkhand. The tendency of unintentional injury to occur was higher in the age group 16 to 19 years, males, living in a nuclear family, smoking tobacco, visually impaired, and living in the overcrowded house and most occurred in homes followed by other venues like schools and streets. Health education among adolescents, parents, school teachers, and district health authorities are required for addressing causes, severity, complication, and prevention of unintentional injury.