
Abstract
Introduction
Recreational cycling is gaining popularity in Singapore but there is a lack of literature regarding the spectrum and severity of these injuries and their impact on the utilisation of healthcare resources. We aim to characterise these injuries, as well as to review the healthcare resources required by injured cyclists.
Methods
A retrospective review of patients with recreational cycling-related injuries presenting to the Emergency Department (ED) between August 2018 and December 2020 was performed. Information about demographics, circumstances of injury, injuries sustained, clinical progress, and outcomes were collected and analysed.
Results
There were 214 patients, with an increase in monthly attendance towards the end of the study period. The median age was 48 years old (interquartile range (IQR) 31 to 60) and 165 (77.1%) patients were male. In the ED, 35 (16.4%), 142 (66.4%), and 37 (17.3%) patients were triaged as P1 (emergent), P2 (urgent), and P3 (ambulatory) respectively. Blunt injuries occurred in 210 (98.1%) patients. Soft tissue injuries involving the upper and lower limbs were most common. One hundred and eighty-one (84.6%) patients had a minor to moderate injury classified by an Injury Severity Score of 0 to 8. One hundred twenty-four (57.9%) patients were admitted to the hospital with 40 (18.7%) requiring surgery.
Conclusion
Recreational cycling-related injuries are increasingly encountered in the ED. These injuries are associated with morbidities which require utilisation of healthcare resources. Legislation and education efforts to promote safety in recreational cycling are required to reduce accidents and minimise the impact of the injuries sustained.
Introduction
Recreational cycling for exercise or commute is gaining popularity in Singapore due to an increased focus on health and fitness, as well as awareness of the environment. 1 This was further contributed by COVID-19 restrictions on international travel, social gatherings, and group activities.2,3 In response, local authorities have led improvements in infrastructure to support recreational cycling as part of overall efforts to reduce the carbon footprint of the country, as well as to encourage a healthy lifestyle. 4 However, this changing trend of recreational cycling is not without negative consequences. According to the annual traffic statistics of 2020, there was an increase in the number of casualties who were cyclists or pillions from 460 in 2019 to 570 in 2020. 5
The main pattern of injuries from recreational cycling involves superficial trauma such as abrasions, contusions, and lacerations involving the extremities, followed by other body regions like head, face, trunk and neck.6,7 Among these, head injuries from recreational cycling were associated with higher morbidity and mortality rates. 8 However, the healthcare resources for injuries from recreational cycling was only briefly examined in one local study reporting the utilisation of healthcare resources caused by accidents related to elderly cyclists and motorcyclists. 9 There existed a gap in local literature focusing on injuries from recreational cycling across all age groups. Therefore, we aimed to characterise the spectrum and severity of recreational cycling related injuries presenting to the Emergency Department (ED) of a restructured hospital, as well as to describe the utilisation of healthcare resources for these injuries.
Methods
Setting
This study was conducted at the general Emergency Department (ED) of (anonymised for peer review) with an annual census of about 105,000 patients and trauma-related complaints accounted for about 15% of all attendances.
Trauma care at the pre-hospital level is provided by paramedics who are sent to the accident scene by the Singapore Civil Defence Force (SCDF) for the assessment, treatment, and transport of the injured patients to public hospitals. Adult patients will be transferred to the nearest general ED. Paediatric patients (less than 16 years old) will be conveyed to the nearest paediatric ED-if they are in extremis (e.g. airway compromise, profound shock or cardiopulmonary arrest), they will be conveyed to the general ED instead.
Our hospital has a single-tier trauma team which is made up of emergency physicians and surgeons from the general surgery and orthopaedics departments. Additional consults from other departments such as neurosurgery or otolaryngology may be obtained by the trauma team in specific cases. This team is activated by a pre-defined criteria which includes mechanism of injury, anatomical injuries, and physiological parameters.
Design
A retrospective study involving a review of case records was conducted from August 2018 to December 2020. All patients who presented to the ED with injuries due to recreational cycling for the purpose of exercise or commute were included. Patients with injuries due to cycling for competitive purpose, or use of motorised bicycles and personal mobility devices were excluded. The patients’ medical records were accessed for data collection and tabulated in a standardised form. Information including demographics, mode of arrival to the ED, place of occurrence, mechanism of injury, use of helmets, injuries sustained, injury severity score (ISS), disposition from the ED, admitting discipline, level of care and length of stay were collected. Utilisation of healthcare resources included the need for ambulance at the pre-hospital level, as well as the need for hospital admission, trauma team activation, blood product transfusion and surgery performed.
Ethics
This study was approved by (anonymised for peer review).
Statistical methods
SPSS version 22 (SPSS, Chicago, IL) was used to perform the statistical analysis. Categorical and continuous data were presented using frequencies with percentages and medians with interquartile ranges (IQR) respectively. Association between categorial variables was assessed using Fisher’s exact or chi-squared test. Odds ratio (OR) with 95% confidence interval (CI) was calculated for measure of association. Statistical significance was taken at a p-value of less than 0.05.
Results
Patient characteristics
Population demographics (n = 214).
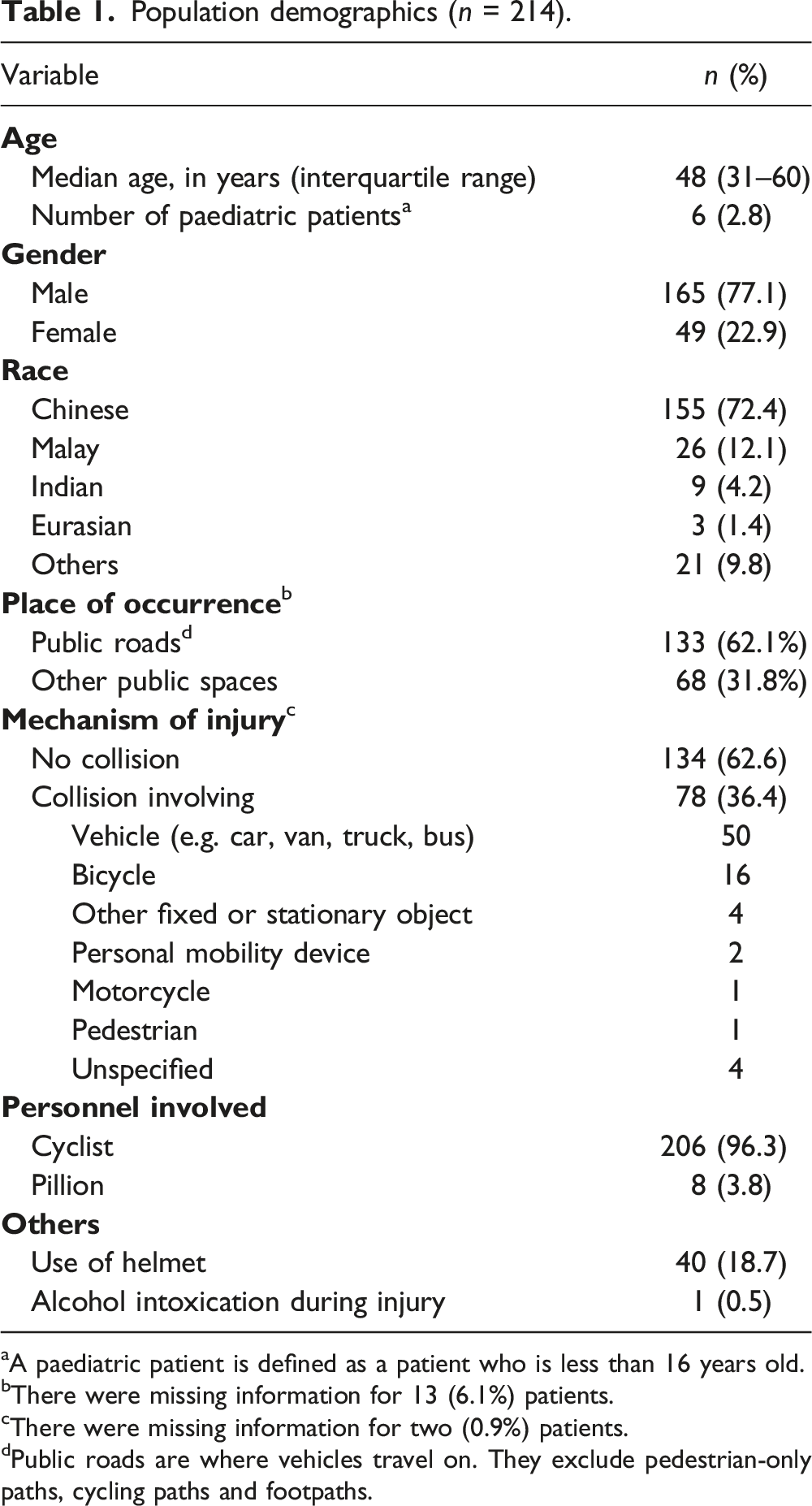
aA paediatric patient is defined as a patient who is less than 16 years old.
bThere were missing information for 13 (6.1%) patients.
cThere were missing information for two (0.9%) patients.
dPublic roads are where vehicles travel on. They exclude pedestrian-only paths, cycling paths and footpaths.
Type and severity of injuries
Type and severity of injury (n = 214).

aThere were patients with more than one body region affected or more than one type of injuries.
Utilisation of healthcare resources
Utilisation of healthcare resource (n = 214).

Trends and associations in recreational cycling related injuries
There was a time trend towards an increased incidence of patients with recreational cycling-related injuries in the second half of 2020 as compared to the preceding months of the study period. (Figure 1). However, this increased incidence was not associated with more injuries with ISS of 9 and above [22/136 (16.2%) vs 11/78 (14.1%), OR 0.9 (0.4–1.9), p = 0.69] and increased admission to hospital [81/136 (59.6%) vs 43/78 (55.1%), OR 0.8 (0.5–1.5), p = 0.53]. Monthly number of patients with recreational cycling related injuries during the study period (n = 214).
Comparing patients with an ISS of 9 and above to those with an ISS of 8 and below, the proportion of patients with accidents occurring on public roads [22/33 (66.7%) vs 111/181 (61.3%), OR 1.3 (0.6–2.8), p = 0.56], with accidents involving collisions [12/33 (36.4%) vs 66/181 (36.5%), OR 1.0 (0.5–2.2), p = 0.99], and those who were not using helmet [24/33 (72.7%) vs 150/181 (82.9%), OR 0.6 (0.2–1.3), p = 0.17] were not significantly differently.
Examining the effect of COVID-19 pandemic and the associated lockdown measures from April 2020, the proportions of injuries as a result of accidents on public roads were not significantly different [before April 2020: 78/120 (65.0%) vs April 2020 onwards: 55/94 (58.5%), OR 1.3 (0.8–2.3), p = 0.33].
Discussion
With the increasing popularity of recreational cycling in Singapore, there is an increased number of patients with recreational cycling-related injuries at the ED. 10 Many recognise the health and environmental benefits that recreational cycling brings but not its associated risks. In this study, we have shown that these patients would require medical attention for their injuries and utilise healthcare resources, particularly upon admission to the hospital.
While emergency and trauma teams are familiar with the tenets of Advanced Trauma Life Support which provides a systematic approach, recognition of the unique considerations of injuries related to recreational cycling can enhance their assessment and management of the trauma patient. For instance, these patients can have multiple injuries which affect more than one body region, and while soft tissue injuries of the upper and lower limbs are common, it is important that these external injuries which are obvious do not distract the team from identifying the less common and obvious traumatic brain injuries and solid organ injuries. Also, in evaluation of the soft tissue injuries, radiographs may be necessary to help distinguish contusions, sprains, strains and tears from fracture and dislocation. The use of clinical decision rules for imaging at the ED and bedside ultrasound may aid in this decision-making process.
Healthcare resources were utilised to varying degrees throughout the patient’s journey. At the pre-hospital level, these patients were able to make their way to the ED from the accident scene by themselves instead of requiring conveyance by an ambulance. This was due to the majority of patients having sustained minor to moderate injuries. At the hospital level within the ED, the activation of the trauma team was also uncommon. However, at the hospital level beyond the ED, more than half of the patients required admission to the hospital for further care, with almost a fifth requiring surgery. These represented significant requirements for inpatient and surgical resources at the hospital. To cope with this, we suggest developing alternative models of care and workflows which could be applicable for trauma patients with minor to moderate injuries like those in this study. For instance, since these patients have a short length of stay, admission to the short stay ward may be considered to reduce the demand for regular inpatient beds. Expedited imaging, trauma care pathways and community rehabilitation services can be further developed to minimise length of stay for patients. Also, patients who require non-emergent surgery can be discharged with early appointments at the specialist outpatient clinic for review and elective operation can be scheduled instead of waiting in the hospital indefinitely for a slot in the emergency operation theatre. These alternative strategies would be especially suited for this group of patients as they are generally younger as seen from our study and are therefore likely to have less complex healthcare issues.
Our study identified that more than of the accidents happened on public roads where recreational cyclists had to interact with vehicles, and as a result, accidents with collisions predominantly involved other vehicles-a finding that was similar to reports from United States.7,11 Even though accidents on public roads and those involving collision were not significantly more common in patient with ISS more than 9, we advocate for the importance to develop guidelines and educate recreational cyclists on traffic rules and etiquette as they do not undergo formal licensing process to cycle on the road. This is in line with the Singapore Active Mobility Advisory Panel’s effort for public safety. 12 A code of conduct has taken effect in January 2022 and it balances the needs of motorists and cyclists to create a safer road environment for all road users. Other than guidelines such as limitations on cycling group sizes and safe distances between cyclists and other road users, it has also recommended better public education and imposing penalties to reduce errant behaviours. Further efforts to minimise collisions with other vehicles include road user segregation by having dedicated cycling paths so that recreational cyclists are moved away from shared road usage with motorists.5,11
The large majority of the accidents in our study did not involve collisions, suggesting that other than road usage, environmental, bicycle and rider factors may also contribute to the occurrence of recreational cycling related injuries. Environmental factors such as uneven or slippery road surfaces, sharp turns, up-and down-slopes may exist during the ride. Examples of bicycle factors include malfunction or wear-and-tear of various components of the bicycle, while examples of rider factors include control of the cycling speed and care while cycling. All these factors can contribute together or individually to the cyclist losing control of the bike and subsequent fall, leading to injuries.13–16 Therefore, environmental awareness and safe cycling habits are paramount-the recreational cyclist must be on the lookout for potential hazards and ride in a defensive manner to protect himself or herself.
We found a need to reinforce the use of helmet during recreational cycling. The use of helmet is a requirement for cyclists on public roads in the Active Mobility Act under the Land Transport Authority. 17 Helmet protects the head and can reduce risk of traumatic brain injury, which is among a common cause of mortality in cyclists.8,18,19 Yet, even though majority of the injuries happened on public roads, a large proportion of injured cyclists were not wearing helmets at the time of accident. In addition to helmet, other protective gears for recreational cycling include proper clothing with appropriate skin coverage which can reduce soft tissue injuries which are most commonly sustained, as well as wrist and elbow guards which can reduce fractures and dislocations. 20 Further studies would be necessary to determine the benefits on the protective gears among recreational cyclists so guidelines can make evidence-based recommendations on what is mandatory and what is good to have for minimising injury.
We postulate that the popularity of recreational cycling would continue to persist. Behavioural changes have been brought about by the pursuits of healthier lifestyle and greener environment, as well as the restrictions of the COVID-19 pandemic. These new cycling habits are supported and sustained in the long run by Singapore’s cycling-based movements such as adding more cycling paths and widening footpaths, establishing safety rules and codes of conduct, as well as reviewing legislations.
Limitations
The main limitation was that our study was based on the experience of a single ED. Other patients with recreational cycling related injuries, particularly those with minor injuries who were likely to present to primary care units such as general practitioner clinics or polyclinics, were not captured by our study. Therefore, the magnitude of recreational cycling related injuries, as well as the actual utilisation of healthcare resources, would most likely be higher than reported here. Next, the healthcare costs arising from the utilisation of healthcare resources by injured cyclists were not assessed.
Also, this was a retrospective study based on available records as documented by various medical personnel which could be inconsistent, leading to missing or incomplete information. Furthermore, as predictors and outcomes of could not be predetermined, we had to work with existing data which were available from the electronic medical records. We were thus unable identify specific reasons for observed trends or perform a more detailed analysis on the various factors contributing to the injuries and their associated outcomes or utilisation of healthcare resources. These details can be used to derive a clinical decision rule or guide policy-making for safer recreation cycling practices. It will also help to enhance healthcare facilities such as urgent care clinics to deal with the increasing needs of this group of patients, thereby offloading EDs and hospitals. 21
Looking forward, we trust that this work would generate further collaboration at a national level. A prospective study involving all primary care units and hospitals would be useful to provide further clarity on the issues reported and the associated healthcare costs. The Haddon Matrix can be incorporated to examine the accidents according to pre-event, event and post-event phases, with identification of contributory factors. 22 This in-depth analysis of each accident would provide valuable information in policy-making so that guidelines and legislations can be developed for prevention, thereby reducing actual accidents and the associated morbidity and mortality. Subsequently, information sharing and collaboration with Ministry of Transport, Land Transport Authority and Traffic Police would contribute to a concerted effort to improve safety for recreational cyclists and other road users.
Conclusion
The increased popularity of recreational cycling is expected to continue and injuries will occur. It is therefore crucial for the healthcare teams to be cognisant of injuries related to recreational cycling and the healthcare resources that would be needed to care for the injured cyclists. While the Singapore Active Mobility Advisory Panel has implemented measures and legislations that improve road safety and reduce accidents, public education must persist and all recreational cyclists must adopt safe riding habits. Ultimately, it is about preventing injury among recreational cyclists, and improving outcomes among injured recreational cyclists.
Footnotes
Author contributions
(anonymised for peer review).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by (anonymised for peer review).
Informed consent
Waiver of consent was granted by (anonymised for peer review).
Data availability
The data of this study would not be available in accordance to approval by (anonymised for peer review).