
Abstract
Background
Chest pain is considered one of the crucial indicators in detecting acute coronary syndrome (ACS), and one of the most common complaints frequently found in hospitals. Atypical characteristics of chest pain have prevented patients from being aware of ACS. Chest pain symptoms have become ambiguous, particularly for specific parameters, such as gender, diabetes mellitus (DM), or other clinical conditions. Therefore, it is critical for high-risk patients to have adequate knowledge of specific symptoms of ACS, which is frequently associated with late treatment or prehospital delay. Therefore, this study aims to identify the particular characteristics of chest pain symptoms in DM and non-DM patients with ACS.
Design and methods
This is a quantitative and non-experimental research, with the cross-sectional approach used to carry out the analytical observation at a general hospital from January- April 2019. Data were obtained from a total sample of 61 patients, comprising 33 ACS with DM and 28 ACS non-DM patients.
Results
The result showed that the characteristic of patients with chest pain symptoms has a significant relation to DM and ACS. Therefore, non-DM patients with ACS are more likely to feel chest pain at moderate to a severe level, while ACS-DM patients are more likely to have low to moderate chest pain levels.
Conclusion
The significant differences in the characteristics of chest pain in DM and non-DM patients suffering from acute coronary syndrome are the points of location of chest pain radiating to the neck and quality of pain.
Introduction
Significance for public health
There are lots of differences in the various chest pain symptoms experienced by diabetes mellitus and non-diabetes mellitus patients with the acute coronary syndrome. Therefore, this study aims to provide optimal nursing care to patients and educate them along with their family members on the various chest pain symptoms to avoid delay in seeking medical attention.
Cardiovascular disease is the most severe cause of death among all non-infectious diseases and accountable for 17.5 million deaths in the world. This means that 46% of global deaths are attributed to non-infectious diseases, with approximately 7.4 million caused to ischemic heart disease. 1 According to data from Jakarta Acute Coronary Syndrome (JACS) registry, a total of 1223, 1915, and 1925 patients suffered from non-ST elevation myocardial infarction (NSTEMI) of the acute coronary syndrome (ACS) in 2007, 2010 and 2013, respectively. 2 These numbers showed that the prevalence of ACS has experienced increment over the years. Conversely, the ACS Registry in the hospital recorded approximately 1-2 ACS patients per day. Acute coronary syndrome requires early identification and management to prevent further severe complication.3,4 Studies have considered chest pain as a critical indicator and main complaint in detecting this disease. 5 Atypical characteristic of chest pain makes the patient unaware of having ACS due to its ambiguity, especially in specific parameters such as gender differences, diabetes mellitus, or any other clinical conditions. 5 Therefore, it is critical for high-risk and ACS patients to perceive the specific symptoms correctly since it has been frequently associated with late treatment or prehospital delay, which is one of the leading causes of ACS morbidity and increase in mortality rate.6-
Diabetes mellitus also takes into account the increased mortality rate due to ACS. According to previous studies,6-9 ACS patients with diabetes mellitus experience symptomatic conditions, such as atypical chronic and acute ischemia, which is mainly observed in type 2 DM patients. Heart mortality in patients with DM is frequently associated with prevalence silent ischemia, which is triggered by autonomic neuropathy, thereby decreasing the chest pain felt by them. Therefore, it leads to uncertainty of patients in early and appropriate detection of ACS.10,11
Several studies have been carried out in studying chest pain characteristics in DM patients. However, such studies are rarely found in Indonesia. Therefore, based on the description above, this study aims to investigate the characteristic of chest pain in ACS patients with DM at a general hospital in Malang, East Java, Indonesia.
Design and Methods
This is a quantitative non-experimental research, with the analytical observation method used to carry out the cross-sectional study at a general hospital in Malang, East Java, Indonesia from January-April 2019. Furthermore, the respondents were selected through the purposive sampling method. The inclusion criteria used in this study are as follows: i) Patients diagnosed with STEMI and NSTEMI; ii) patients are male; iii) above the age of 40 years; iv) Patients with acute myocardial infarction without chest pain (angina) for 24 hours; v) patients who are hemodynamically stable; vi) patients without acute decompensated heart failure (ADHF); vii) patients without malignant arrhythmias, viii) patients without in Acute Lung Oedem (ALO) condition; ix) patients not using ventilator; x) patient willing to and become respondents. Meanwhile, the exclusion criteria used in this study are: i) Patients with several complications, thereby making it impossible to interview them; ii) patients who have never undergone CABG surgery; iii) patients who refuse to be respondents. Based on the inclusion and exclusion criteria, the total sample obtained in this study is 61 patients.
This study utilized the chi-square statistic test to analyse the demographic characteristics and its differences in chest pain of DM and non-DM patients with the acute coronary syndrome. The questionnaire used in this study is a modified flowchart (SCORE chart). 12 Furthermore, the study was approved by the Institutional Ethics Committee of Dr. Saiful Anwar Hospital, number 400/016/K.3/302/2019.
Results and Discussions
The patient's baseline characteristics observed in this research include ages, body mass index, marital status, educational background, occupation, type of payment, clinical history and medical diagnosis. Table 1 shows the distribution analysis result of baseline characteristics of ACS patients at the hospital. The total number of respondents in this study are 61 patients, consisting of 33 ACS patients with diabetes mellitus and 28 ACS without DM. Table 1 shows that out of the baseline characteristics of patients, only two types of payment and hypertension record where significant to respondents suffering from chest pain (p<0.05). Therefore, a significant number of ACS patients bearing DM tend to carry out payment using varying JKN general payment and employment insurance strategies. Furthermore, the proportion of hypertension as a risk factor is also shown to be significantly higher than the ACS group with non-DM.
Baseline characteristics.
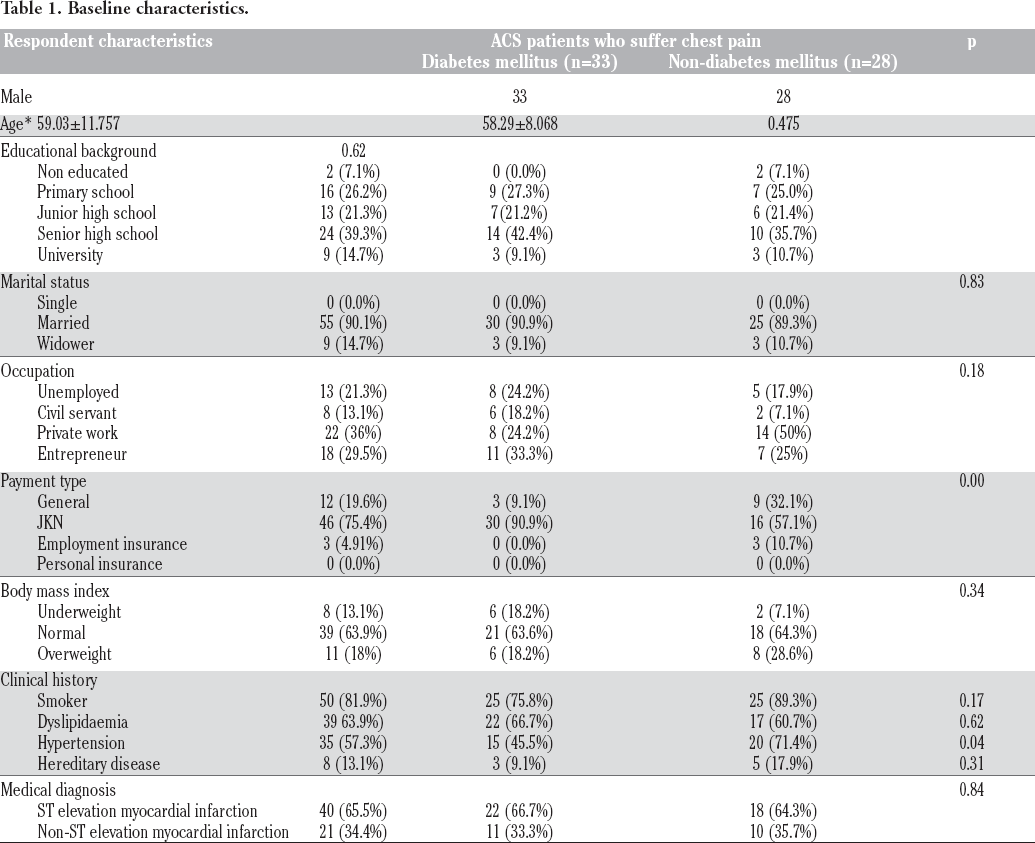
Table 2, shows the chest pain characteristic differences in ACS patient which distinct DM from non-DM. The results indicate that out of 6 points related to chest pain characteristics, 2 had significant relations (p<0.05). The table also indicates a point of chest pain location, which attacks around the chest and radiates around the neck. Chest pain proportion in radiating to the neck is relatively higher in ACS patients non-DM than ACS patients with DM. Table 3 shows the analysis result regarding the characteristic of typical symptoms in ACS patients with DM and non-DM. Out of all points mentioned above, the value of p is over 0.05 which corresponds to the fact that there are no significant differences between atypical symptoms in ACS patients with DM and non-DM, as shown in Table 2. Therefore, it can be concluded that symptoms are typically not affected by clinical history of diabetes mellitus.
Chest pain characteristics.
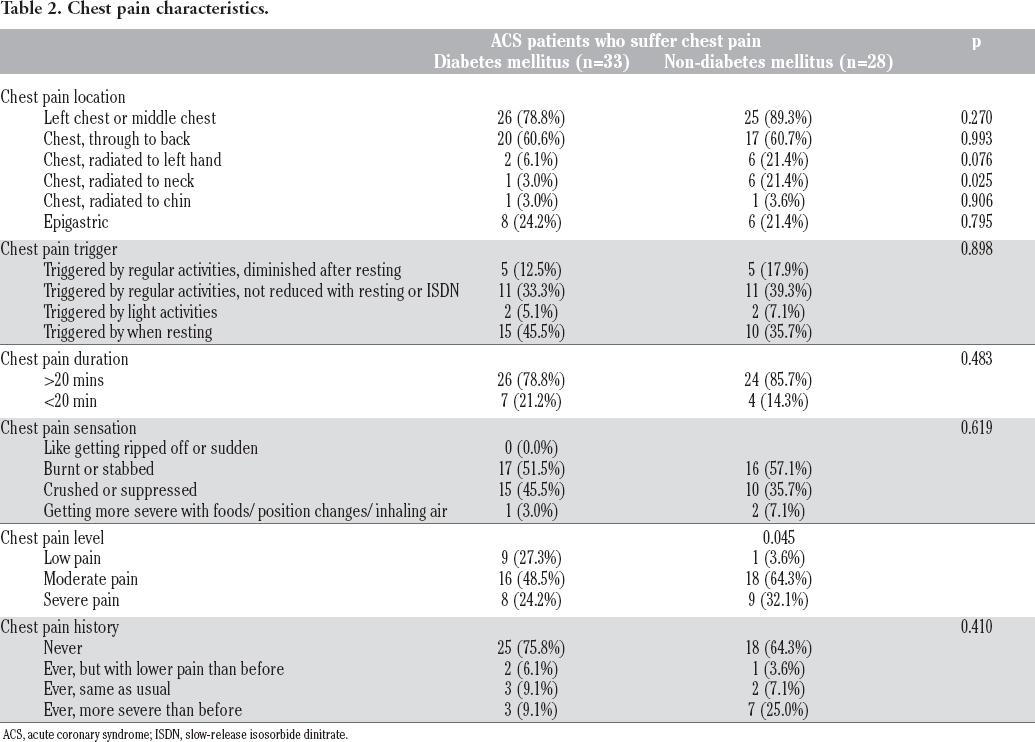
ACS, acute coronary syndrome; ISDN, slow-release isosorbide dinitrate.
Characteristics of atypical symptoms.

ACS, acute coronary syndrome.
The characteristics of chest pain used in this study consist of 6 points, namely location, triggers, duration, sensations, levels and history. Out of the 6 characteristics, 2 have significant p values below 0.05, namely areas around the chest pain location and radiating to the neck, as well as the chest pain level. In the point of chest pain location, between ACS patients with DM and non DM, both have a proportional comparison in a higher number of patients suffering chest pain from left to middle. This is because the anatomical position of the heart is on the left side, therefore the pain tends to radiate more on that side through the cervical nerve.12,13 However, significant differences were obtained in chest location that radiates to the neck with a p-value less than 0.05. Chest pain location that radiates to the neck occurs to ACS patients with DM. This fact was supported by a previous study, 14 which stated that ACS patients with DM or those with high-risk tend to suffer atypical chest pain which is triggered on the side of atypical pain distribution, such as the arm, shoulder, back, etc. This is in line with the researches carried out by DeVon 14 and Funk, 15 which stated that area or location of chest pain distribution which frequently occurred in ACS patients with DM is on the arm, neck, chin and back.
Generally, ACS patients with non-DM tends to suffer more atypical chest pain which initiated on the left or middle chest. 16 However, there are no significant differences in chest pain location between ACS patients with DM and non-DM. This is because, in patients with DM, chest pain seems to be rather biased. Therefore, several numbers of patients are considered difficult to describe the exact location of chest pain.17-19 This can be possibly proposed as references in the identification of chest pain characteristics in the future.
Another point with significant differences is chest pain level with a p-value below 0.05 is patients with acute coronary syndrome and DM. This category of patients has low and moderate chest pain level, while those with and non-DM have moderate to severe pains. According to the previous research,13,17 ACS patients with DM tend to be incapable of feeling pains, or inconveniences around the chest. This is because there is a mechanism of cardiac autonomic neuropathy which causes damage to autonomic nerve fibres. 11 Therefore, the delivery of pain stimuli from the myocardium to cerebral is hindered and eventually leads to the inability to identify pain.11,17 Therefore, this leads to difficulties in early detection process of acute coronary syndrome symptoms, thereby increasing the mortality rate due to silent ischemia.20-22 Furthermore, ACS patients with DM frequently experience asymptomatic indication, such as cold sweat or difficulty in breathing. 23,24 However, in this research, there are no significant differences in asymptomatic indication of patients with DM or non DM.
Conclusion
The significant differences in the characteristics of chest pain in patients with acute coronary syndrome with diabetes mellitus and non-diabetes Mellitus are the points of location, which radiates to the neck and the quality of pain. Acute coronary syndrome patients with diabetes mellitus tend to feel chest pain radiating to the neck more than those with acute coronary syndrome and nondiabetes Mellitus. The scale of chest pain at mild to moderate levels is generally more pronounced in patients with the acute coronary syndrome with diabetes mellitus than in those without diabetes mellitus. Furthermore, there were no significant differences in the asymptomatic symptoms felt by the two groups of patients with acute coronary syndrome.
Footnotes
Acknowledgement
The authors are grateful to the Ministry of Research, Technology and Higher Education of the Republic of Indonesia, Research and Community Service Brawijaya University and Saiful Anwar Hospital for their support and assistance.