
Abstract
Background
The total number of people affected by dementia worldwide is increasing rapidly. Recent studies provided evidence for the contribution of modifiable risk and protective factors to dementia risk. Although healthcare professionals could play an essential role in informing the general public about the relationship between lifestyle and dementia, it is unclear what they know about this relationship. Therefore, this study assesses the awareness of dementia risk reduction among current and future healthcare professionals.
Design and methods
An online survey was carried out among 182 healthcare students from Maastricht University and 20 general practitioners (GPs) and practice nurses in Limburg, The Netherlands. The survey assessed the knowledge about risk and protective factors of dementia and identified needs, wishes and barriers concerning dementia risk reduction strategies.
Results
The majority of current (75.0%) and future (81.9%) healthcare professionals indicated that dementia risk reduction is possible. Among students, awareness of cardiovascular risk factors of dementia (e.g., coronary heart disease (44.5%), hypertension (53.8%)) was low. Most participants (>70.0%) would like to receive more information about dementia risk reduction.
Conclusions
The majority of current and future healthcare professionals were aware of the relationship between lifestyle and dementia risk. However, there are still substantial gaps in knowledge regarding individual dementia risk factors. Given the essential role of healthcare professionals in providing lifestyle advice, there is a need to increase awareness by providing educational programs focused on dementia risk reduction.
Significance for public health
Since the number of individuals with dementia is increasing worldwide, dementia is a major public health concern. As there is no curative treatment for dementia yet, recent research has focused on the contribution of lifestyle factors to dementia risk. Cumulating evidence has shown that modifiable risk factors such as smoking, hypertension and depression are attributable to around 40% of all dementia cases. However, the majority of the general public is unaware of the relationship between lifestyle and dementia risk. Although current and future healthcare professionals play an important role in informing the general public about this relationship, the present study showed that there are gaps in knowledge on specific risk factors for dementia. Therefore, educational programs are urgently needed to increase awareness of dementia risk reduction among current and future healthcare professionals.
Introduction
Dementia is a progressive neurodegenerative disorder that leads to memory impairments, difficulties in carrying out daily activities and personality changes. 1 The global impact of dementia continues to grow as life expectancy increases. The rising total number of individuals affected by dementia is accompanied by increased healthcare costs and burden on caregivers, families and society. 2 The World Health Organization (WHO) has predicted that 82 million people in 2030 and 152 million people in 2050 will have dementia. 1 Yet, the incidence of dementia in Europe and North America has been declining over the past three decades.3-6 Improved provision of and access to education and better treatment and management of cardiovascular risk factors (e.g., blood pressure control and antithrombotic medication) may explain this decline.3,5,6
Since there is no disease-modifying cure for dementia available yet, dementia research has recently shifted to focus more on the contribution of modifiable lifestyle factors like smoking, physical inactivity and obesity to dementia risk. Modifiable risk factors may account for up to 40% of all dementia cases worldwide. 3,7,8 The Lancet Commission on Dementia Prevention, Intervention, and Care suggested that lifestyle modifications may already have an influence on dementia risk decades before the onset of dementia.3-8 These findings provide opportunities for prevention of dementia through lifestyle interventions earlier in life.9-11 This was recently supported by the WHO guidelines on risk reduction of cognitive decline and dementia. 1 Still, most people seem to be unaware of a relationship between lifestyle factors and dementia risk and consider dementia as an inevitable part of ageing.12,13 A recent study showed that 56% of the Dutch population aged 40-75 years believed that there is nothing one could do to decrease dementia risk. 14 More specifically, the majority of the population was unaware of the relationship between cardiovascular risk factors and dementia risk.12,14
To decrease dementia risk within our ageing society, the general public needs to become more aware of the influence of modifiable risk and protective factors. For this, healthcare professionals need to have adequate knowledge of preventative strategies for dementia, since they play a key role in conveying this information to the general public. Nevertheless, previous studies have shown that general practitioners (GPs) only sporadically provide advice on preventive strategies for dementia, which could be explained by the concerns about their knowledge regarding this topic.15-17 Survey studies conducted in Malta and Malaysia found inadequate knowledge of dementia risk factors among pharmacy and medical students.18,19 However, it is unclear what healthcare students and professionals know about dementia risk reduction in The Netherlands. Therefore, the current study aims to assess the knowledge of dementia risk and protective factors among current and future healthcare professionals in The Netherlands.
Design and methods
Study population and recruitment
The present study assesses the level of knowledge of current healthcare professionals (GPs and practice nurses) and future healthcare professionals (healthcare students) on the association between lifestyle factors and dementia risk. The future healthcare professionals sample consisted of students enrolled in various health-related bachelor programs at Maastricht University (Maastricht, The Netherlands), namely Health Sciences, Biomedical Sciences, European Public Health, Medicine, and Psychology. All (first, second and third year) bachelor students from these study programs were eligible to participate in this study (e.g., no age or language restrictions). Compared to the Netherlands, where international students make up 20% of the total student population, the student population of Maastricht University is characterized by a large number of international students (2019: 54% for all Bachelor's and Master's programs combined). The current healthcare professionals sample included GPs and practice nurses employed within the Province of Limburg, The Netherlands. Compared to the rest of the Netherlands, health disparities are persistent in the Provence of Limburg, especially in South-Limburg. In the Netherlands, practice nurses are registered nurses with additional education and training who work within an expanded scope of the general practice that includes diagnosing and treating specific medical conditions [e.g., diabetes, cardiovascular risk management (CVRM), chronic obstructive pulmonary disease (COPD)].
Students were recruited using advertisements in faculty newsletters, through social media platforms, as well as via poster/leaflet distribution within university buildings. The local GP associations Cohesie and Huisartsen Oostelijk Zuid Limburg (HOZL) approached GPs and practice nurses via a weekly newsletter, and the GP association Zorg in Ontwikkeling (ZIO) contacted them via a personal letter. The present study was approved by the Medical Ethics Committee of Maastricht University Medical Centre+ (METC azM/UM) (reference number: 2019-1054).
Measurements
Both study samples were asked to complete an online survey (LimeSurvey). The survey was available from April 2019 to September 2019. All participants received an information letter and signed a digital informed consent form prior to participation. Participants were asked to complete questions about their study program (for students) or the number of years of professional experience (for GPs and practice nurses) to confirm eligibility. The survey also included items on socio-demographic factors (e.g., age, gender). To assess the knowledge about dementia risk reduction, a 24-item questionnaire from the Dutch ‘MijnBreincoach’ survey was used,14,20 including ten translated items from the British Social Attitudes (BSA) survey. 21 These items covered self-reported knowledge of dementia, personal experience with people with dementia, dementia risk awareness, and knowledge of modifiable risk and protective factors. Most items were set up as statements. Participants indicated to what extent they agreed or disagreed on a five-point Likert scale ranging from ‘completely disagree’ to ‘completely agree’. The statement used to measure our primary outcome (awareness of dementia risk reduction) was: “There is nothing you can do to reduce your risk for dementia.” Further, the survey included statements on 12 modifiable risk and protective factors of dementia incorporated in the validated ‘LIfestyle for BRAin Health’ (LIBRA) index.9,22 This validated dementia risk index was developed to yield insight into one's personal potential for reducing dementia risk. Factors included in the LIBRA index are physical inactivity, smoking, alcohol use, cognitive activity, healthy diet/Mediterranean diet, depression, hypertension, obesity, diabetes, hypercholesterolemia, coronary heart disease, and renal disease.9,22-27 All statements about LIBRA factors were set up to be correct (e.g., “High blood pressure increases your risk of getting dementia” and the number of correctly identified LIBRA factors was summed up to evaluate someone's overall knowledge of LIBRA factors (our secondary outcome). Furthermore, the participants were asked whether they would be interested in acquiring more knowledge regarding the relationship between lifestyle and dementia/brain health, their preferred information source, and perceived barriers to engage in a brain-healthy lifestyle. The questionnaire, available in both Dutch and English, consisted of 30 items for students and 29 items for GPs/practice nurses. For students, an additional item was included about the exposure to the topic dementia risk reduction as part of their study program. The English version of the complete survey (for both study samples) is shown in Appendix 1.
Statistical analysis
Independent samples t-tests and one-way ANOVA tests were used to examine whether there were differences between years of professional experience (within GPs/practice nurses), study years (within students), study programs (within students) and gender (within students) regarding the awareness of dementia risk reduction (primary outcome) and the number of correctly identified risk and protective (LIBRA) factors (secondary outcome). X 2 tests were used to investigate whether participants who stated that their knowledge of dementia was good were more aware (both for our primary and secondary outcome) compared to participants who indicated that they had poor or reasonable knowledge of dementia. All statistical analyses were performed using IBM SPSS statistics (version 25). The level of statistical significance used was p<0.05.
Results
Demographics
The study sample consisted of 182 students and 20 GPs/practice nurses. The characteristics of the students and GPs/practice nurses are summarized in Table 1 and Table 2, respectively.
Awareness of dementia risk reduction
In the student sample, 81.9% was aware of the relationship between lifestyle and brain health by indicating that dementia risk reduction is possible. Three quarters (75.0%) of the GPs/practice nurses stated that dementia risk reduction is possible. More experienced health care professionals (11-40 years) did not agree more often with this statement compared to less experienced health care professionals (0-10 years) (66.7% vs 87.5%; X 2 (1)=1.111, p=0.292). There were significant differences with regard to the percentage of students who were aware of the relationship between lifestyle and brain health across study years (year 1: 69.2%, year 2: 88.1%, year 3: 82.8%; X 2 (2)=8.268, p=0.016). In the student sample, there was no association between gender and awareness of the relationship between lifestyle and brain health (males: 90.0%, females: 79.6%; X 2 (1) =2.284, p=0.131). There were no differences between study programs with regard to the awareness of the relationship between lifestyle and brain health (Health Sciences: 88.1%, Medicine: 82.4%, Biomedical Sciences: 77.1%, European Public Health: 78.9%, Psychology: 88.2%; X 2 (4)=2.729, p=0.604). Moreover, 47 students (25.8%) stated that their knowledge regarding dementia was good, 104 students (57.1%) indicated that their knowledge was reasonable, and 31 students (17.0%) indicated that their knowledge of dementia was poor. Among the students who indicated that their knowledge regarding dementia was good, 40 students (85.1%) agreed with the statement dementia risk reduction is possible. Furthermore, 87 students (83.7%) who indicated that their knowledge was reasonable agreed with this statement. In addition, 22 students (71.0%) of the students who indicated that their dementia knowledge was poor agreed with the statement that dementia risk reduction is possible. Of the GPs/practice nurses, 6 professionals (30.0%) indicated that their knowledge of dementia was good and 14 professionals (70.0%) stated that their dementia knowledge was reasonable. Among the GPs/practice nurses that indicated that their knowledge was good, 5 professionals (83.3%) agreed with the statement that dementia risk reduction is possible. Amongst those that indicated that their dementia knowledge was reasonable, 10 GPs/practice nurses (71.4%) agreed with this statement. There was no significant association between self-reported dementia knowledge (e.g., poor, reasonable or good) and the percentage of participants that agreed to statement on dementia risk reduction in both students (X 2 (2)=3.037, p=0.219) and GPs/practice nurses (X 2 (1)=0.317, p=0.573).
Knowledge of dementia risk and protective factors
The proportion of students (n=20; 11.0%) and GPs/practice nurses (n=1; 5.0%) that correctly identified all twelve risk and protective factors of dementia was low. Moreover, 99 students (54.4%) and 13 GPs/practice nurses (65.0%) correctly identified 8-12 risk and protective factors, and 38 students (20.9%) and 3 GPs/practice nurses (15.0%) only identified 0-4 factors correctly. There were no differences regarding the mean number of correctly recognized risk and protective factors between more experienced (11-40 years of professional experience) and less (0-10 years of professional experience) experienced GPs/practice nurses (7.83±2.17 vs 8.50±2.88; t=0.592, p=0.561). In the student sample, there were significant differences with regard to the mean number of correctly identified risk and protective factors between the different study years (F(2, 181)=5.332, p=0.006). First year bachelor students identified less risk and protective factors correctly compared to second (6.46±3.39 vs 7.96±3.26; p=0.020) and third year students (6.46±3.39 vs 8.59±2.50; p=0.014). On average, male students identified more risk and protective factors of dementia compared to female students (8.58±2.74 vs 7.37±3.36; t= -2.087, p=0.038). There were no differences between the study programs with regard to the mean number of correctly identified risk and protective factors (Health Sciences: 8.31±2.93, Medicine: 8.35±3.52, Biomedical Sciences: 7.51±3.25, European Public Health: 6.63±3.25, Psychology: 6.12±3.08; F(4, 181)=2.314, p=0.059). Since the sample size for the Biomedical Sciences study program was reasonable (n=70: Year 1: 19; Year 2: 44; Year 3: 7), differences between study years were investigated. Yet, no differences were found with regard to the mean number of correctly identified risk and protective factors between study years of the Biomedical Sciences program (year 1: 6.63±3.77, year 2: 7.52±3.04, year 3: 9.86±1.95; F(2, 69)=2.637, p=0.079). Of the participants that reported that their dementia knowledge was good, 32 students (68.1%) and 5 GPs/practice nurses (83.3%) identified 8-12 dementia risk and protective factors correctly. Of the students stating their dementia knowledge was reasonable or poor, 54 students (51.9%) and 13 students (41.9%) correctly identified 8-12 risk and protective factors for dementia, respectively. There was no association between self-reported dementia knowledge (e.g., poor, reasonable or good) and the mean number of correctly identified risk and protective factors in both students (poor: 6.74±3.42, reasonable: 7.51±3.26, good: 8.49±3.03; F(2, 181)=2.904, p=0.057) and GPs/practice nurses (reasonable: 7.50±2.38, good: 9.50±2.07; F(1, 19)=3.181, p=0.091).
Group characteristics of the healthcare students.

Group characteristics of the GPs/practice nurses.
Students identified cognitive activity (92.9%), healthy diet (87.4%) and physical inactivity (84.1%) most often as being a risk or protective factor for dementia. GPs/practice nurses correctly identified physical inactivity (90.0%), hypertension (85.0%), and cognitive activity (85.0%) most often. Students least often recognized vascular-related factors such as chronic kidney disease (28.0%), coronary heart disease (44.5%), hypertension (53.8%) and obesity (54.4%) in relation to dementia risk. GPs/practice nurses least often identified low-to-moderate alcohol use (35.0%), depression (40.0%), obesity (55.0%) and chronic kidney disease (55.0%). Compared to students, GPs/practice nurses recognized hypertension (85.0% vs 53.8%; t=3.465, p=0.002), diabetes (80.0% vs 59.3%; t=2.092, p=0.047), chronic kidney disease (55.0% vs 28.0%; t=2.269, p=0.033) and coronary heart disease (70.0% vs 44.5%; t=2.288, p=0.031) more often as risk factors for dementia. The percentages of correctly identified dementia risk and protective factors in both samples are presented in Figure 1.
Male students identified smoking (85.0% vs 62.7%; t=3.180; p=0.002), physical inactivity (97.5% vs 80.3%; t=4.119; p<0.001), diabetes (72.5% vs 55.6%; t=2.036; p 0.046), healthy diet (95.0% vs 85.2%; t=2.130; p=0.036) and chronic kidney disease (42.5% vs 23.9%; t=2.135; p=0.037) more often as being a risk or protective factor compared to female students. Students from the Biomedical Sciences study program recognized smoking more often as being a dementia risk factor compared to Psychology students (77.1% vs 35.3%; p=0.009). Health Sciences students identified coronary heart disease more often as a dementia risk factor in comparison with students from Biomedical Sciences (69.0% vs 34.3%; p=0.001), European Public Health (69.0% vs 31.6%; p=0.045), and Psychology (69.0% vs 17.6%; p=0.002). Medicine students recognized coronary heart disease more often as a dementia risk factor compared to Psychology students (58.8% vs 17.6%; p=0.037). Figure 2 shows the percentages of correctly identified risk and protective factors among the different study programs.
Needs, wishes and barriers
Most students (73.1%) and GPs/practice nurses (70.0%) indicated that they would like to receive more information about the relationship between lifestyle and brain health/dementia risk. Both students (68.4%) and GPs/practice nurses (55.0%) indicated that they would like to receive information on this topic via the Internet, followed by visiting the website of the Dutch Alzheimer's Association (students: 40.8%; GPs/practice nurses: 55.0%). In addition, students would like to gain more information through their study program (66.1%), consulting their GP (40.8%) and via the website of the municipal health services (31.0%). The largest barriers for implementing a brain-healthy lifestyle in daily life were lack of knowledge (students: 59.2%; GPs/practice nurses: 40.0%), lack of time (students: 54.0%; GPs/practice nurses: 50.0%) and lack of motivation (students: 27.0%; GPs/practice nurses: 15.0%). Other barriers for students were having difficulties with organizing (27.6%), financial reasons (25.3%), and health problems (6.9%).
Discussion
The current study assessed the knowledge of current and future healthcare professionals on dementia risk reduction. Most of the students and GPs/practice nurses were aware of a relationship between lifestyle and dementia risk. Nevertheless, there are still some substantial gaps in knowledge in both groups regarding individual dementia risk factors, especially regarding cardiovascular risk factors. The majority of participants indicated that they would like to receive more information on the relationship between lifestyle and dementia risk, primarily via the Internet (both groups), their study program (students) and their GP (students). The current study shows that Dutch healthcare students were in general aware of the relationship between lifestyle and dementia risk. In a recent Malaysian study, only one third of pharmacy and medicine students was able to correctly identify potential risk factors for dementia. 18 Although the study samples were comparable regarding age and gender distribution, the current study showed a higher level of awareness among Dutch students. The exact reason for this difference is unclear and might be related to several causes and/or circumstances. For instance, it could be related to a difference in the attitude towards dementia. In a previous study, Malaysian medicine students showed fewer positive attitudes towards dementia compared to medicine students from the United Kingdom. 28 Furthermore, this difference in the level of awareness between countries could be related to national dementia initiatives. To increase awareness of and to reduce the stigma around dementia, several countries, such as the Netherlands, have recently implemented a National Dementia Strategy. While the current study showed a higher level of awareness among students, particular gaps in knowledge exist regarding cardiovascular risk factors. Around half of the healthcare students did not recognize cardiovascular factors as being risk factors for dementia. This knowledge gap regarding cardiovascular risk factors has also been previously reported among the Dutch general public 14 and might be explained by the notion that the general public is becoming more aware of the association between cardiovascular risk factors (e.g., hypertension, diabetes) and cardiovascular complications (heart health) instead of linking those factors at the same time to increased dementia risk (brain health).29,30
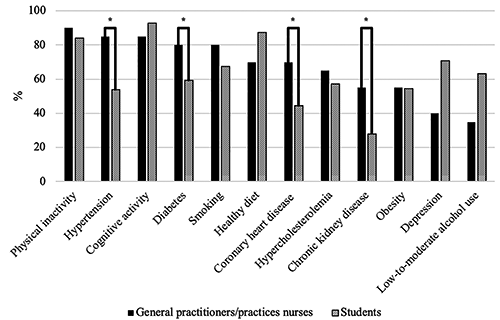
Percentages of correctly identified risk and protective factors for dementia among both GPs/practice nurses and students. *p<0.05.

Percentages of correctly identified risk and protective factors for dementia among the different study programs. *p<0.05.
Among GPs/practice nurses, one in four indicated that dementia risk reduction was not possible. However, most of the GPs/practice nurses were aware of the contribution of cardiovascular factors to dementia reduction. This is in line with a previous study conducted in Hungary in 2019 among 209 GPs demonstrating that GPs listed vascular and metabolic risk factors most often as being risk factors for dementia. 31 In contrast, a study conducted in Spain reported on the unawareness among GPs and pharmacists with regard to hypercholesterolemia and hypertension as being risk factors for dementia. 32 Differences in the knowledge of healthcare professionals between countries might be due to several factors/circumstances such as the national policy on dementia and the availability and the level of educational/training programs for healthcare professionals focused on dementia (risk reduction). 33
Interestingly, both students and GPs/practice nurses who indicated that their knowledge of dementia was good, did not show more awareness than participants who indicated that their knowledge was reasonable or poor. This shows that current and future healthcare professionals might overestimate their knowledge or feel unsecure about their own knowledge of dementia. The lack of confidence of healthcare providers about their knowledge of dementia and healthy ageing has previously been reported. 15,16 This could explain the alarming finding that although healthcare professionals believe they should play an important role in identifying individuals at risk for dementia, they only sporadically provide advice on dementia risk reduction to their patients.17,34 Lack of knowledge also was identified by both the students and the professionals as the main barrier why they personally do not engage in a brain-healthy lifestyle. However, most of the participants indicated that they were eager to learn more about dementia risk reduction and students specifically indicated that they would like to receive information via their study programs. In a previous study, GPs themselves identified a need for more dementia education in undergraduate, specialist and ongoing training. 35 These findings together suggest that there is a need to address dementia specifically both in undergraduate and postgraduate programs. Therefore, implementation of this topic within the curriculum of health-related study programs could be a promising first step to raise awareness among future healthcare professionals. Although most study programs have a general introduction on the topic of dementia in their curriculum, information about (modifiable) dementia risk factors and preventive strategies is often lacking. Therefore, it is suggested to include a dedicated lecture on dementia prevention with a focus on cardiovascular risk factors to dementia risk to increase awareness among current and future healthcare students.
Apart from identifying individuals at risk for dementia, the knowledge of healthcare professionals regarding modifiable dementia risk factors is also important from a public health perspective. Previous studies have found that the majority of the general population in Europe, United States, Eastern Asia, Israel and Australia did not believe dementia risk could be reduced by lifestyle changes.12-34 A recent study conducted in The Netherlands showed that 56% of the general population was unaware of a relationship between lifestyle and dementia risk. 14 Although a recent public health campaign in The Netherlands was not able to reach a population-level increase of awareness of dementia risk reduction, it showed that individuals exposed to the campaign were more aware of dementia risk reduction and more inclined towards behavioral change. 20 Besides public health campaigns, the emergence of Massive Open Online Courses (MOOCs) provides an opportunity to globally improve public awareness of dementia risk reduction. 36 Additionally, healthcare professionals should function as a reliable source of education for the general public, once adequately educated. Importantly, not only the healthcare professionals mentioned in the current study should benefit from dementia-specific training, but knowledge gaps have also been identified in other dementia healthcare providers such as nurses and aged care staff members. 37 Thus, there is a need to inform all current and future healthcare professionals about dementia risk reduction. This is also in line with recent recommendations to implement dementia prevention strategies on a societal level.1,3,8,38 Effective strategies to increase awareness among healthcare professionals include educational programs with an interactive approach that provide tools to support the application of training into practice. 39 Although these programs are likely to improve professional awareness, policy changes might be urgently needed to support awareness on a larger scale. Therefore, education focused on dementia risk reduction should be incorporated in the training programs of all healthcare professionals working within the dementia field or working with people at risk of dementia.
Maintaining a healthy brain throughout the whole lifespan is also crucial for dementia risk reduction. 38 Therefore, dementia prevention strategies should not only start at the age when first changes in the brain occur (40-75 years of age) but should already start decades before (e.g., adolescence). Due to their large population reach, healthcare professionals such as GPs and practice nurses would be the most suitable group to provide lifestyle advice in order to reduce dementia risk on the long term. For example, hypertension is the most common reason to visit the GP in The Netherlands. The GP or practice nurse could use this appointment to explain the link between hypertension and both cardiovascular and brain health and provide tailored lifestyle to lower the blood pressure. Next to increasing awareness, the link between lifestyle and dementia risk might be an additional stimulus for people to make sustainable lifestyle changes.
One of the main strengths of our study is that students of multiple health-related study programs participated. These future healthcare professionals will be employed in various disciplines. Besides medical doctors, other healthcare professionals (e.g., psychologists, public health advisors) will also meet middle-aged individuals who are interested in ways to foster their brain health. 40 Another strength of the current study is that non-Dutch students were also able to participate because the questionnaire was available in both Dutch and English. By including non- Dutch students, the current study sample serves as a good representation of the international student population of Maastricht University. Additionally, our study samples were representative in terms of mean age of GPs/practice nurses (The Netherlands: 48.0 years; current study: 48.5 years) and percentage of female healthcare students (The Netherlands: 74.1%; current study: 78.0%). To our knowledge, this is the first study reporting the knowledge of students from different healthcare fields on the risk and protective factors for dementia. Moreover, a similar methodology as in previous dementia literacy studies was used.14,21 This provides consistency related to existing knowledge and allows for some comparisons between studies.
However, our study has some limitations. Due to small sample sizes, the generalizability of our results might be limited. The participants of the study may not be an exact reflection of the population of interest since participants might have been more interested in dementia and health in general. Possible reasons for this selection bias might be the restricted recruitment of students and healthcare professionals. The student recruitment was limited to the use of social media, (news-)letters and posters and leaflets and GPs/practice nurses could only be reached indirectly via online newsletters or personal letters of GP associations due to privacy issues.
In conclusion, the present study showed that most current and future healthcare professionals were aware of the relationship between lifestyle and dementia risk. However, a considerable gap in the knowledge of specific risk factors, in particular cardiovascular- related risk factors, still exists. Therefore, future educational programs should focus on the credo: ‘What's good for the heart, is good for the brain’. These findings and the participants’ desire to receive more information regarding the relationship between lifestyle and brain health show the necessity of educating current and future healthcare professionals about dementia risk reduction. Implementing dementia prevention in the curriculum of different study programs and additional training of current healthcare professionals could be a promising strategy to not only increase awareness among healthcare professionals but also indirectly among the general public.
Footnotes
Acknowledgements
We thank all study participants, the Faculty of Health, Medicine and Life Sciences of Maastricht University, and the Alzheimer Centrum Limburg for their support in carrying out the study.