
Abstract
Background
Major depressive disorder (MDD) is a very prevalent mental disorder worldwide. Beyond MDD’s individual impact, it also constitutes a real burden for society, as it affects all domains of everyday life. Lifestyle factors may play an important role in the prevention, development, progression, and treatment of MDD. Consequently, our research aimed to assess the relationships between depressive symptoms and lifestyle to identify which lifestyle characteristics constitute risk or protective factors against depression. Furthermore, since adults aged between 18 and 29 years are at most risk of developing depressive symptoms, we focused on this population.
Methods
Two hundred and ten young adults, aged 18 to 29 years, completed online questionnaires assessing lifestyle behaviors—including physical activity, sleep quality, dietary habits, connectedness to nature, mindfulness, and resilience—and depressive symptoms.
Results
Regular physical activity, balanced diet, good sleep quality, mindfulness, and resilience to stress were all correlated with lower levels of depression. The study did not reveal a significant relationship between connectedness to nature and depression in this sample.
Conclusion
These results align with previous research, highlighting that physical activity, diet, sleep quality, mindfulness, and stress resilience are crucial for managing depression; connectedness to nature requires further study.
“Our research findings reinforce the well-established link between lifestyle behaviors and depressive symptoms, highlighting the importance of physical activity, dietary habits, sleep quality, mindfulness, and stress resilience.
Introduction
Major depressive disorder (MDD) is one of the most common mental disorders worldwide. It is associated with cognitive (e.g., concentration difficulties), emotional (e.g., sadness), behavioral (e.g., avoidance) and physiological (e.g., appetite disturbances) symptoms. 1 MDD affects an estimated 3.8% of the global population: some 320 million people. This prevalence includes approximately 5% of adults, with a gender distribution of 4% among men and 6% among women. 2 The prevalence of depression is highest among young adults aged between 18 and 24 years (21.5%), and lower in adults aged ≥65 years (14.2%). 3 According to Sciensano, 4 Belgium’s public health institute, the group in that country that is most at risk of developing depressive disorders is young adults aged between 18 and 29 years. This age group is particularly vulnerable to the onset of depression, underscoring the need to examine how lifestyle factors contribute to this disorder so we can create effective intervention strategies. Young adults often face unique stressors tied to transitions in education, work, and personal relationships, which can exacerbate mental health difficulties. Supporting this assertion, Wagener et al 5 observed similar findings in the specific context of the COVID-19 pandemic. They determined that younger adults tended to experience more intense negative emotions, as well as higher levels of worry and rumination, than older adults.
The etiology of MDD is widely recognized to be complex and multifactorial, involving genetic, environmental, psychological, and neurobiological influences. 6 For instance, genetic vulnerability, as indicated by a family history of depression, has been shown to increase the likelihood of developing the disorder.7,8 Likewise, substance use, which is especially common in young adulthood, has been found to contribute independently to both the onset and exacerbation of depressive symptoms because of its impact on neurochemical regulation.9,10 In contrast to these chronic vulnerability factors, precipitating factors such as significant illness, 11 traumatic events, and acute psychosocial stress 12 can also trigger depressive episodes. While these pathways of causality have significantly enhanced our comprehension of the origins of depression, it also seems relevant to address these issues with a correlational approach, which can offer a complementary lens, one that foregrounds the dynamic interplay between lived experience and symptom expression.
Beyond its effects on individuals suffering from depression, such as impairments in individual and family functioning,13,14 social isolation, 15 and deterioration of physical health, 16 MDD also imposes a significant burden on society. Its impact manifests in multiple dimensions, including direct costs (e.g., medical and pharmaceutical expenses related to the treatment of MDD), suicide-related costs, and indirect costs such as workplace costs (e.g., reduced productivity). 17 The growing prevalence of MDD, 18 along with its substantial societal and individual burden, highlights the need to proactively address the underlying factors contributing to this mental health challenge. To achieve this goal, a focus on the risk and protective factors for depression would be relevant. Interestingly, previous studies have demonstrated that lifestyle modifications, such as increased physical activity, healthy dietary choices and improved sleep quality, can lead to favorable outcomes in both preventive and therapeutic contexts.19,20 From that perspective, addressing lifestyle disturbances appears a promising approach.
“Lifestyle” refers to a person’s behavioral patterns 21 and includes everyday behaviors in several life domains (e.g., health, work, social relationships, leisure activities, education). It varies based on specific geographical, economic, political, cultural and religious contexts. 22 Important lifestyle behaviors involve exercise, nutrition, substance use, social interaction, time spent in nature, and meditation or relaxation. 23 An individual’s lifestyle choices and behaviors can lead to “lifestyle diseases”: conditions that often arise from factors such as poor diet, insufficient physical activity, and exposure to unhealthy environments. Various diseases, including depression, are classified as lifestyle diseases due to their association with these lifestyle factors. 24 For instance, research has shown that poor eating habits and lack of physical activity can increase the risk of depression, whereas regular physical activity and a healthy diet can help alleviate depressive symptoms and improve mental well-being.25,26 Furthermore, a large-scale study (84 860 participants) utilizing data from the UK Biobank provides evidence of the influence of specific lifestyle factors on depressive mood. The cross-sectional analysis revealed that physical activity, a healthy diet, and optimal sleep duration were linked to a lower frequency of depressive symptoms in both MDD patients and healthy controls. Longitudinal analyses corroborated these findings, demonstrating that both optimal sleep and a healthy diet served as protective factors against depressive mood in both groups. These results underscore the critical role of lifestyle modifications—particularly in diet and sleep—in the management and prevention of depression. 27
The World Health Organization 28 reported a 25% rise in the global prevalence of depression during the first year of the COVID-19 pandemic. This surge was linked to abrupt, substantial lifestyle changes and emphasized that both healthy and unhealthy lifestyle behaviors can function as protective or risk factors for depression, a circumstance that demands increased attention. Understanding the influence of lifestyle on depression is critical not only for enhancing individual well-being but also for addressing public health concerns. Evidence suggests that the accumulation of lifestyle risk factors correlates with an additive increase in the risk of developing depressive symptoms. 29 In this context, Wong et al 30 demonstrated that lifestyle medicine offers a promising strategy for mitigating such risks. Their meta-analysis found that multifaceted lifestyle interventions—which include changes in diet, increased physical activity, better sleep hygiene, and stress management—are particularly successful in both preventing and managing depression, especially in more severe cases. Furthermore, such interventions could potentially lower the overall prevalence of depression, 30 reduce the economic costs related to the disorder, 31 and improve overall health-related quality of life. 32
In line with the above-mentioned findings, research focusing on the interplay between lifestyle factors and depression is essential as it offers potential avenues for improving mental health outcomes through lifestyle modifications. From that perspective, this study is intended to address this gap by adopting a holistic approach to understand how various lifestyle factors interact with depression. Specifically, it focuses on young adults aged 18 to 29, a group that is particularly susceptible to developing depressive symptoms. 3 The study explores the relationship between several lifestyle factors—physical activity, dietary habits, sleep patterns, connection to nature, mindfulness, and resilience skills—and depressive symptoms. Ultimately, an understanding of how these behaviors influence depression could significantly contribute to the identification and development of effective strategies for its prevention and management. In this context, this research seeks to offer novel insights into the impact of various lifestyle elements on depression, thereby facilitating the development of targeted interventions that promote healthier lifestyles for young adults.
Method
Participants and Procedure
The local ethics committee of our university’s faculty of psychology approved the protocol (approval number: 2223-052), and all participants completed the informed consent process online.
A cross-sectional correlational study was conducted from April to August 2024. Based on a priori power analysis using G*Power 3.1, 33 the required sample size was determined to be a minimum of 200 participants, with an alpha level of 0.05, a power of 0.8, and an effect size of 0.25 for the correlations. Participants were recruited through a combination of posters, emails to various groups, social media platforms, and offline methods. Participation in the study was entirely voluntary.
Measures
The self-administered assessment pack comprised eight separate questionnaires, accompanied by an information sheet explaining the study’s objectives related to the assessment of depression and lifestyle factors. These questionnaires were (1) sociodemographic information, (2) Center for Epidemiology Studies Depression Inventory (CES-D); (3) Five Facet Mindfulness Questionnaire—Short Form (FFMQ-SF); (4) Connectedness to Nature Scale (CNS); (5) Dietary Habits Evaluation; (6) Ricci-Gagnon questionnaire on physical activity; (7) Spiegel’s Sleep Questionnaire; and (8) Brief Resilience Scale (BRS). The questionnaires were administered online to facilitate accessibility and convenience for participants. Strict adherence to data protection regulations was ensured during the questionnaires, thereby safeguarding the confidentiality and security of all information provided. The data collected were anonymized and utilized exclusively for research purposes. All questionnaires were validated in French.
Sociodemographic Information
The demographic characteristics of interest included age, gender, and education level.
Depression
Depression was measured using the 20 items of the Center for Epidemiology Studies Depression Inventory (CES-D) 34 to capture various symptoms of depression, including depressed mood, anhedonia, appetite changes, sleep disturbances, and feelings of worthlessness. Participants completed the CES-D by rating each item on a Likert-type scale from 0 (Rarely or none of the time) to 3 (Most or all the time), according to the frequency with which they had experienced each symptom over the past week. The total score was derived by aggregating the responses across all items. The CES-D has demonstrated high internal consistency, with Cronbach’s alpha typically exceeding 0.85, which indicates excellent reliability. For instance, Radloff 34 reported an internal consistency of α = 0.85 in the general population and α = 0.90 in patient samples. Test-retest reliability over a period of several weeks has been reported to range from 0.51 to 0.67, reflecting moderate stability. 34 The CES-D has been widely used in both clinical and non-clinical populations, reinforcing its utility and robustness as a tool for measuring depressive symptoms. 34
Mindfulness
Mindfulness was measured using the 24 items of the Five Facet Mindfulness Questionnaire—Short Form (FFMQ-SF), 35 which captures five key facets of mindfulness: observing, describing, acting with awareness, non-judging, and non-reactivity. Participants rated each item on a 5-point Likert-type scale ranging from 1 (Never or very rarely true) to 5 (Very often or always true), reflecting how frequently they had experienced each aspect of mindfulness over the past month. The total score was calculated by summing the responses to all items.
Bohlmeijer et al 36 reported that the FFMQ-SF demonstrated strong internal consistency, with Cronbach’s alpha values ranging from 0.82 to 0.92, confirming its reliability in assessing different dimensions of mindfulness. Additionally, the questionnaire exhibited strong convergent validity with other established mindfulness measures, affirming its suitability for both research and clinical applications.
Connectedness to Nature
Connectedness to nature was assessed using the 14-item Connectedness to Nature Scale (CNS), 37 which measures an individual’s affective experience of connection with the natural environment. Participants responded using a self-administered questionnaire, rating each item on a five-point Likert-type scale, ranging from “completely disagree” to “completely agree.” The CNS captures various dimensions of connectedness to nature by evaluating the subjective relationship between the self and nature. The French version of the CNS has demonstrated strong reliability: Navarro et al 38 reported Cronbach’s alpha values ranging from 0.81 to 0.89, confirming its consistency in measuring this construct.
Dietary Habits
Dietary behaviors were assessed using the Dietary Habits Evaluation questionnaire. 39 This 10-item instrument enables participants’ dietary profiles to be classified according to their consumption of various foods and beverages over the preceding weeks. The items specifically evaluate the intake of fruits and vegetables, dairy products, meat, processed foods, and foods with added sugars. Responses are rated on a Likert-type scale, with scores ranging from 1 to 5 for each item. The cumulative score derived from these items reflects participants’ overall dietary habits, with higher scores indicating healthier eating patterns. Consequently, results are categorized as follows: 10 to 19 points indicates a need for improvement, 20 to 29 points is considered reasonable, 30 to 39 points denotes good quality, and 40 to 50 points signifies excellent dietary quality. The psychometric properties of the instrument were further validated by the significant intercorrelations between the items and the summary score (r = 0.39-0.59, P < .05), suggesting that the items consistently measure interconnected aspects of dietary behavior. 39
Physical Activity
Physical activity levels were assessed with the Ricci-Gagnon questionnaire. 40 This 9-item instrument allows participants’ physical activity profiles to be classified into three distinct categories: inactive, active, and very active. The questionnaire items are rated on a 5-point Likert scale and are organized into three sections: (A) sedentary behavior (1 item); (B) leisure physical activities, including sports (4 items); and (C) daily physical activities (4 items). Each item is scored from 1 to 5 points, resulting in a cumulative score that ranges from 9 to 45 points. A higher total score indicates a greater level of physical activity. Specifically, a cumulative score below 18 points is classified as inactive, a score between 18 and 35 points is considered active, and a score of over 35 points is categorized as very active.
Quality of Sleep
The quality of sleep among participants was evaluated using Spiegel’s Sleep Questionnaire.41,42 This 6-item instrument assesses sleep quality across six distinct domains: sleep latency, sleep quality, sleep duration, nocturnal awakenings, night-time dreams, and the overall sense of alertness and wakefulness upon waking. Each item is scored, allowing for the categorization of sleep quality into four levels: Normal (scores below 13), Regular (scores ranging from 13 to 18), Poor (scores between 19 and 25), and Very Poor (scores exceeding 26).
Resilience
To assess participants’ self-perceived stress management ability, the Brief Resilience Scale (BRS) 43 was employed. The BRS scoring system ranges from 1 to 5, with higher aggregate scores indicating enhanced ability to recover from stress and adversity. 44 The BRS consists of six items that evaluate an individual’s resilience, incorporating both positively (items 1, 3, and 5) and negatively worded items (items 2, 4, and 6). The BRS demonstrates good internal consistency, with Cronbach’s alpha coefficients ranging from .80 to .91, 43 confirming its reliability as a measurement of resilience to stress. Higher scores on this scale correspond to greater resilience in the face of stress.
Analytic Approach
The collected data underwent detailed statistical analysis using Jamovi version 2.5.6. 45 To address the research questions, a series of statistical tests were performed. First, descriptive statistics were calculated to summarize the main characteristics of the dataset, including means and standard deviations. Next, Pearson’s correlation analyses were conducted to examine the relationships between continuous variables, specifically focusing on the associations between depression and various lifestyle factors (i.e., physical activity, dietary habits, sleep quality, connectedness to nature, mindfulness, and resilience skills). The purpose of these analyses was to assess both the strength and the direction of the correlations, providing insight into how variations in lifestyle behaviors may be associated with levels of depression within the study sample. All statistical tests adhered to a significance level of P < .05, and results were reported with 95% confidence intervals to ensure robustness.
Results
We had hypothesized that lifestyle factors such as physical activity, diet quality, sleep, mindfulness, connectedness to nature, and stress resilience are negatively correlated with depressive symptoms in young adults. To explore this hypothesis, descriptive statistics were initially employed to provide an overview of the data, followed by Pearson correlation analyses to investigate the relationships between these variables.
Descriptive Statistics
The final sample comprised 210 French-speaking adults aged from 18 to 29 years (M = 25.7, SD = 2.5). The sample was predominantly female, and the educational level was quite high: 53% of participants had completed a master’s degree and 30% held a PhD.
Sociodemographic Characteristics.
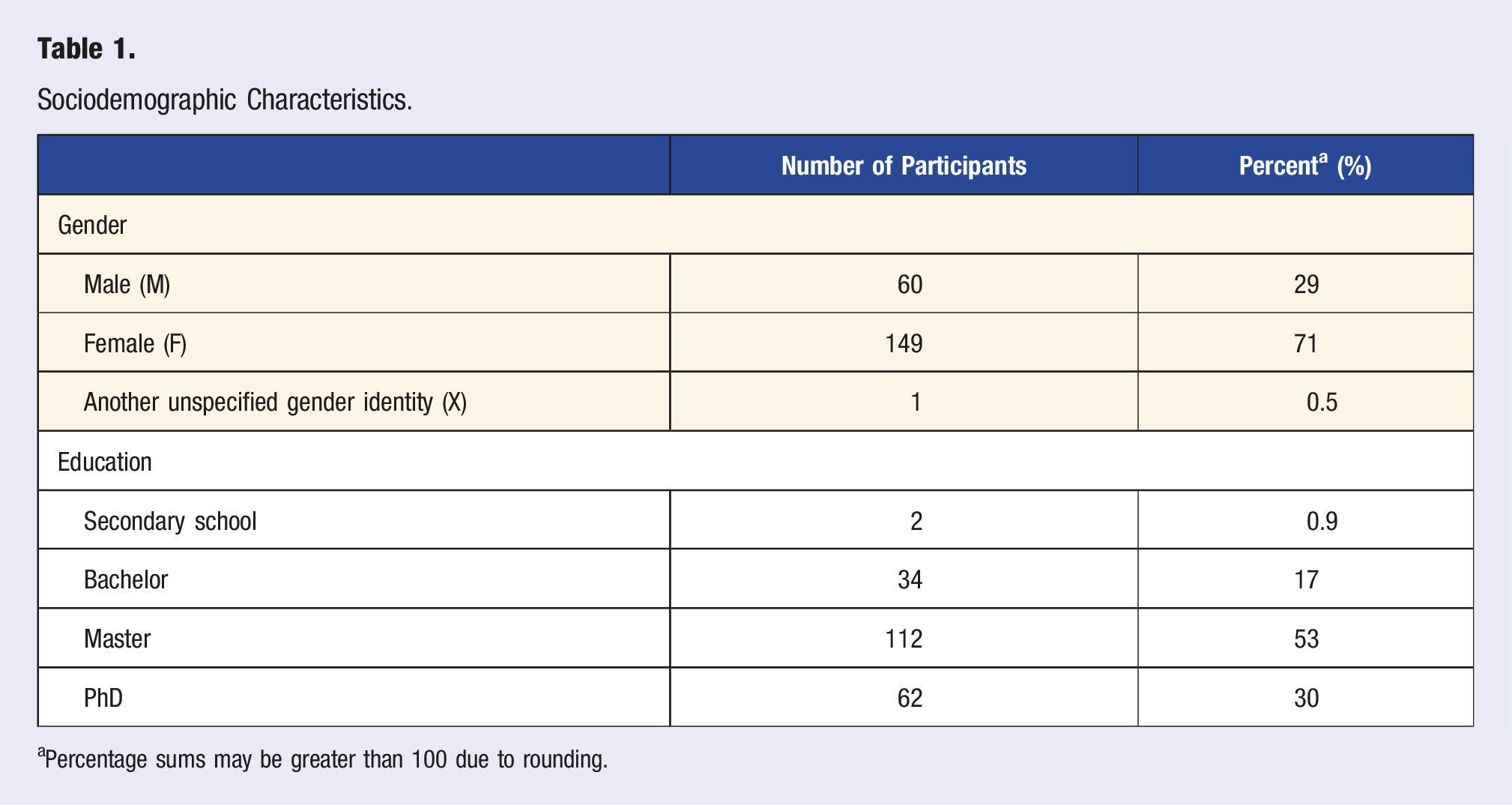
aPercentage sums may be greater than 100 due to rounding.
Descriptive Statistics for Key Lifestyle Factors.
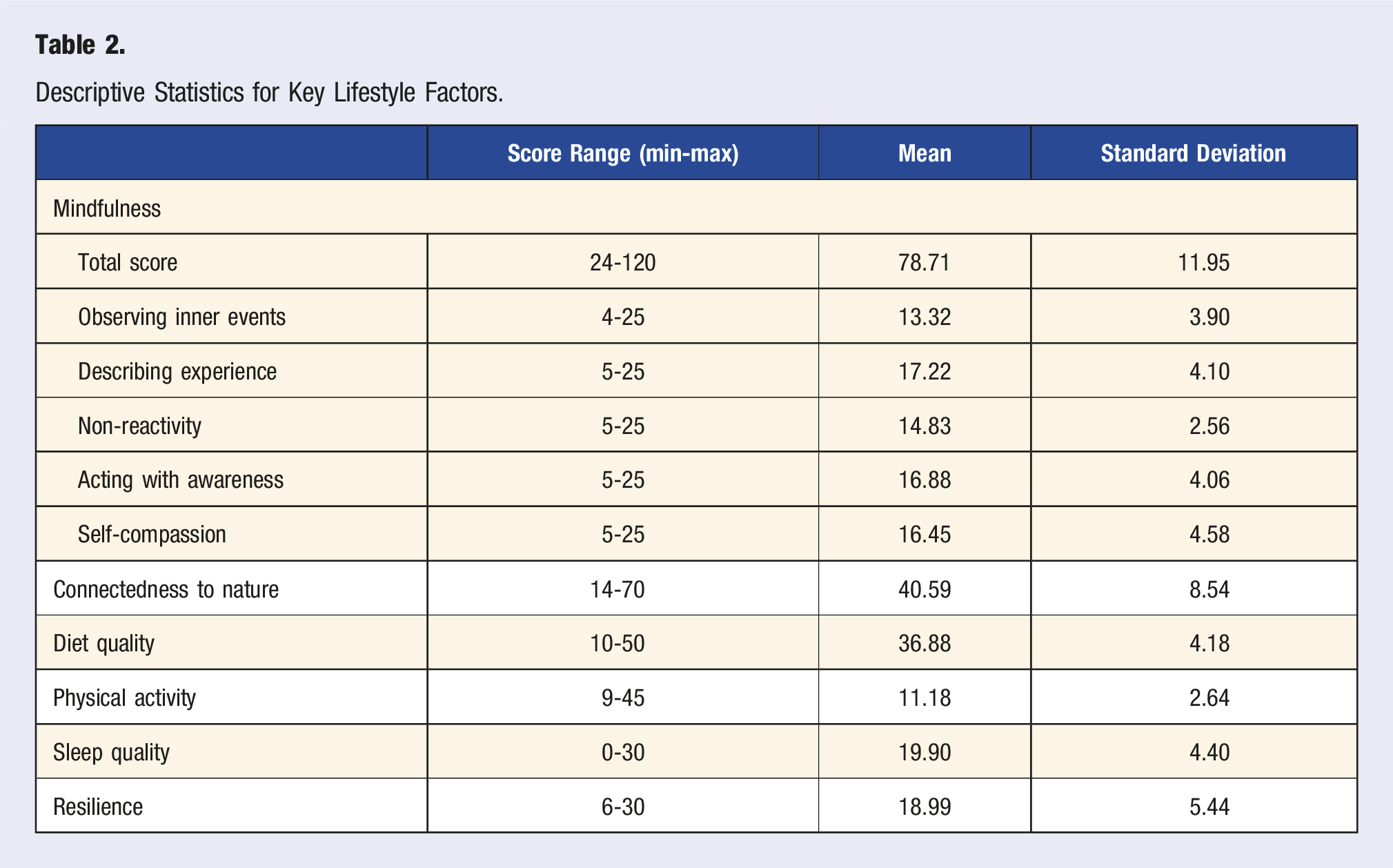
The overall mean depression score for participants was 18.19 (SD = 13.93), indicating that the sample showed mean levels of depressive symptoms above the established cut-off score of 16 on the CES-D. 46
Correlation Analyses
Correlations Between Depression and Lifestyle Factors.
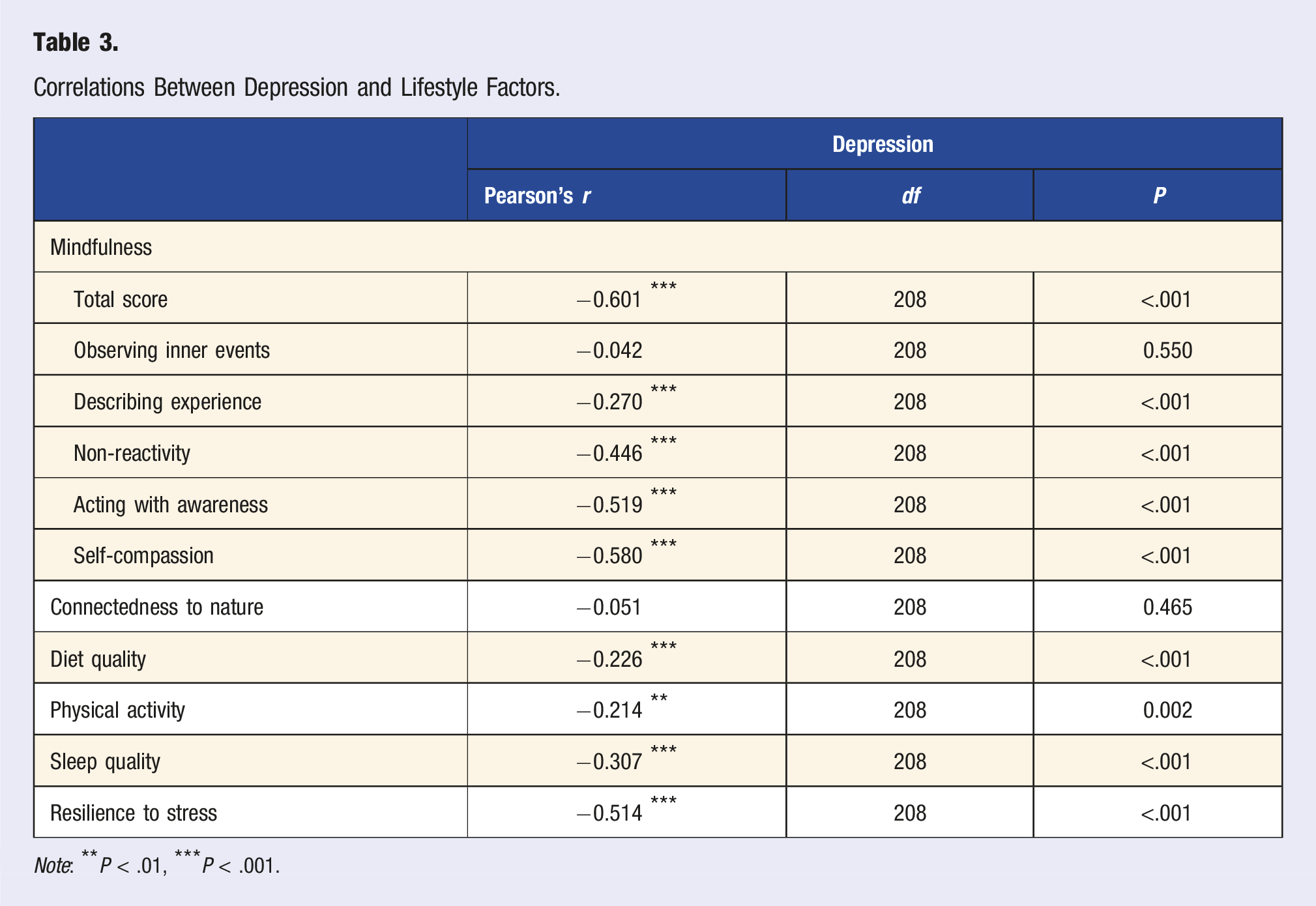
Note: **P < .01, ***P < .001.
Dietary habits (r = −0.22, P < .001), sleep quality (r = −0.30, P < .001), and physical activity (r = −0.21, P = .002) were also significantly negatively correlated with depression. These findings suggest that participants who report healthier dietary patterns, better sleep quality, and more regular physical activity tend to have lower levels of depression. The correlations for these variables, although moderate, still provide evidence of their importance in relation to mental health outcomes.
Connectedness to nature was the only lifestyle factor that did not show a statistically significant relationship with depression (r = −0.05, P = .465). This lack of correlation indicates that, within this specific sample, a sense of connection to nature does not appear to be directly associated with levels of depression. Although previous studies have identified positive associations between nature exposure and mental health outcomes, our study did not find such a relationship.
In summary, the analyses reveal significant negative correlations between five lifestyle factors—mindfulness, dietary habits, sleep quality, resilience, and physical activity—and depression. These results suggest that improvements in these lifestyle domains are associated with reductions in depressive symptoms. In contrast, the lack of a significant correlation between connectedness to nature and depression implies that this factor may not play a direct role in influencing depression within the population in question.
Discussion
This study investigated the relationships between depression and lifestyle factors among young adults aged 18 to 29, a population that is particularly vulnerable to the onset of depressive symptoms. By design, the research was purely correlational and therefore was not intended to establish causal explanations for why depression occurs. Rather, the focus was on examining how fluctuations in selected behavioral indicators, such as sleep quality, physical activity, diet, etc., align with shifts in depressive affect.
Briefly, our findings reinforce the well-established link between lifestyle behaviors and depressive symptoms, highlighting the importance of physical activity, 47 dietary habits, 25 sleep quality, 48 mindfulness, 49 and stress resilience. 50 Understanding these relationships is crucial for the development of targeted interventions that promote healthier lifestyle choices and improve mental health outcomes, thereby addressing the rising prevalence of depression in this age group. The associations between lifestyle behaviors and depression will be discussed in relation to the scientific literature in the following paragraphs.
Research has demonstrated the significant role of various lifestyle factors in influencing depression.51,52 Regular physical activity is strongly associated with reduced symptoms of depression, through a combination of psychosocial and neurochemical mechanisms.47,53-57 From a psychosocial perspective, physical activity promotes self-esteem—potentially by improving physical self-perception, including body image—enhances self-efficacy, and increases social support. These factors, in turn, help reduce symptoms of depression. 54 From a neurochemical perspective, physical activity has been shown to change the brain structure in individuals with depression, improve the functionality of key brain regions, facilitate behavioral adaptation, and preserve the volumes of the hippocampus and white matter. These changes contribute to enhanced neuroprocessing and help mitigate cognitive decline in patients with depression. 58 Furthermore, research has shown that exercise as a treatment for mild to moderate depression can produce effects like those of first-line interventions, including medications and psychotherapy. 59 Our research further corroborates past findings, indicating that modifications in physical activity can significantly alleviate depressive symptoms among young adults.
In parallel, a balanced, nutritious diet is fundamental for maintaining optimal brain function and emotional stability. 60 Evidence increasingly supports the link between balanced eating habits such as the Mediterranean diet and lower risk of depression or depressive symptoms, highlighting the significance of nutrition in managing depression.61-63 A diverse array of essential nutrients is necessary for optimal brain function, since they work synergistically, suggesting that improving the overall diet is likely to provide significantly greater mental health benefits than manipulating any single nutrient in isolation. 64 The findings of this study resonate with the existing literature, reinforcing the assertion that dietary habits are crucial to depression outcomes in young adults.65-67 This alignment not only supports the hypothesis that nutrition is a modifiable risk factor for depression but also calls for innovative strategies that integrate personalized nutrition plans, digital health platforms for dietary monitoring, and interdisciplinary collaborations with nutritionists and mental health professionals to incorporate dietary interventions into holistic mental health frameworks, particularly for vulnerable populations such as young adults.
Since one of the DSM-5 criteria for diagnosing MDD is disturbances in sleep patterns, 1 it is not surprising that a negative correlation between sleep quality and depression symptoms was established here. Sleep disturbances are prevalent in individuals with depression 68 : nearly 90% of patients are affected. 69 Insomnia, in particular, is a frequent sleep difficulty associated with depression and exhibits a two-directional relationship with the disorder. 70 This indicates that not only can depression lead to insomnia, but persistent insomnia can also exacerbate depressive symptoms, creating a vicious cycle. Maladaptive emotion regulation may be a cause of the relationship between poor sleep and depression, clarifying how sleep problems contribute to the development of depressive symptoms in both cross-sectional and prospective contexts. 71 The findings of this study support the existing literature by confirming the negative correlation between sleep quality and depressive symptoms, highlighting sleep disturbances as a risk factor and treatment of such disturbances as a potential protective factor in the context of depression in young adults.48,72,73 This suggests that, while poor sleep can increase the likelihood of developing depression, improving sleep quality may also be a beneficial strategy for alleviating depressive symptoms in this population. This finding underscores the importance of addressing sleep issues in therapeutic interventions designed to reduce depressive symptoms.
Mindfulness and stress resilience have been well documented to be protective factors against depression. Research indicates that mindfulness is associated with reduced levels of depression both directly and indirectly; emotional regulation strategies such as suppression, reappraisal, worry, and rumination act as significant mediators in this relationship.74,75 Furthermore, the capacity to manage stress is closely linked to resilience against depression: high levels of resilience constitute a protective factor that decreases the risk of developing depressive symptoms. Individuals who possess effective coping strategies for managing stress are less likely to experience depression, suggesting that resilience can mitigate the impact of stress on mental health. 76 Our research findings confirm the existing literature by affirming the negative correlation between mindfulness, stress resilience, and depressive symptoms. These findings underscore the importance of integrating mindfulness practice and resilience training into therapeutic interventions meant to prevent and treat depression. By enhancing mindfulness and stress management skills, individuals may bolster their defenses against depressive symptoms and improve their overall mental well-being.
The findings of this study did not reveal any significant relationship between connection to nature and depression within the examined population. However, the existing literature has identified such an association,77-79 suggesting that this relationship should be further explored. Future research should investigate the complexities of how nature-related experiences may affect mental health outcomes, considering factors such as individual differences, environmental contexts, and other potential mediators. An understanding of these dynamics could provide valuable insights into the role of nature exposure in alleviating depressive symptoms.
The results of this study emphasize the importance of addressing lifestyle factors among young adults in the general population. Effective public health initiatives should focus on creating environments that promote healthy lifestyle choices, including regular physical activity, balanced nutrition, and good sleep hygiene. Embedding these components into public health campaigns and community-based programs could more effectively address the root causes of depression. This study suggested that a holistic approach, combining lifestyle modifications with traditional mental health interventions, is essential. We recommend that mental health professionals integrate lifestyle modifications into treatment plans for depression, adapting their approach to each patient’s specific needs and circumstances. A comprehensive strategy includes recommendations for increasing physical activity, improving dietary habits, establishing healthy sleep patterns, adopting mindfulness practices, and fostering resilience to stress. Addressing these lifestyle factors within therapy sessions will allow for a more inclusive and effective intervention framework. By setting specific, actionable goals related to these lifestyle aspects, professionals can complement traditional psychological treatments, leading to a more holistic management of depression. This approach not only targets depressive symptoms but also supports overall well-being, potentially resulting in more enduring mental health benefits.
Our study has several limitations. First, the study’s cross-sectional design limits its ability to establish causation. Although significant associations between lifestyle factors and depression were found, it is unclear whether these factors influence depressive symptoms directly or are merely correlated. Furthermore, the study’s reliance on self-report measures may introduce biases. Participants’ perceptions of their own daily habits may be influenced by social desirability or recall bias. Objective measures, such as wearable devices, could provide more accurate data on lifestyle factors. By addressing these limitations, we can advance our understanding of the complex interplay between lifestyle factors and depression and develop more effective strategies to promote mental well-being.
Because its sample predominantly represented people with Western cultural backgrounds, this study presents minimal bias. Nonetheless, future research should prioritize a more nuanced understanding of how lifestyle behaviors are shaped by complex cultural factors, including entrenched norms, values, and socioeconomic conditions that influence both access to and perceptions of these behaviors. For instance, dietary practices are not solely the result of individual choices but are also shaped by cultural food traditions, regional availability of ingredients, and socioeconomic status. 80 These factors can differ across various populations, leading to diverse dietary habits. Similarly, physical activity cannot be viewed merely as a personal preference; it is also influenced by cultural expectations, the availability of infrastructure such as parks and recreational facilities, and prevailing social norms regarding body image. 81 Consequently, future research should focus on incorporating more culturally diverse samples and developing culturally specific tools to assess lifestyle behaviors. Such a shift would enable the development of more personalized, context-sensitive interventions that account for both lifestyle factors and their cultural contexts. Furthermore, future studies should explore the effectiveness of culturally adapted interventions through randomized controlled trials to understand how lifestyle factors like physical activity, diet, and mindfulness impact depression in different cultural settings. This would contribute to the development of more universally applicable treatments. Additionally, creating culturally appropriate questionnaires to assess lifestyle behaviors in relation to mental health could offer more accurate insights and improve depression management, particularly for at-risk populations.
It is essential to interpret the findings of this study while considering potential confounding variables that were not accounted for in its design. Depression is a complex disorder influenced by a variety of bio-psychosocial and premorbid factors (e.g., family history of mood disorders, substance use). These factors could modify the impact of lifestyle behaviors and may serve as potential confounders. Although these variables were not directly assessed in this study, they may have influenced the observed relationships. To gain a more comprehensive understanding of how lifestyle behaviors interact with depressive symptoms, future research should account for these confounding variables or consider analyzing subgroups based on such background factors. This would facilitate a more detailed exploration of the interplay between lifestyle habits and individual predispositions. Furthermore, a mixed-methods approach that integrates both correlational and causal analysis could offer deeper insights into the intricate connection between lifestyle choices, genetic predispositions, and depression. Employing longitudinal studies or mediation models could help clarify the directionality of these associations and guide more refined intervention strategies.
Conclusion
This study highlights the significant role of lifestyle factors as either risk or protective factors for depression in young adults. Regular physical activity, a balanced diet, adequate sleep, mindfulness, and stress resilience act as protective factors, reducing depressive symptoms, whereas poor sleep, insufficient physical activity, and an unhealthy diet are risk factors associated with increased depression. Although the study did not find a significant relationship between nature connectedness and depression, it underscores the necessity of integrating other lifestyle modifications into mental healthcare.
Supplemental Material
Supplemental Material - Investigating Lifestyle Risk and Protective Factors for Depression in Young Adults: Insights From a Large-Scale Cross-Sectional Study
Supplemental Material for Investigating Lifestyle Risk and Protective Factors for Depression in Young Adults: Insights From a Large-Scale Cross-Sectional Study by Maedeh Parvin, Anne-Marie Etienne, and Aurélie Wagener in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the University of Liège. The funding organization played no role in the design, collection, management, analysis, or interpretation of the data, nor in the preparation, review, or approval of the manuscript, or the decision to submit it for publication.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.