
Abstract
Empowering marginalised urban islanders with limited health accessibility through knowledge transfer program for controlling pulmonary tuberculosis (PTB) requires a specific training module. The study was aimed to develop this training module by adapting and modifying the IMCI (Integrated Management of Childhood Illness) framework. Structuring the content for the knowledge and skills for PTB control in the module was based on the National Strategic Plan for Tuberculosis Control 2016-2020. A total of five knowledge and skills were structured: i) PTB disease and diagnosis, ii) PTB treatment, iii) preventive PTB measures, iv) prevention of malnutrition, and v) psychosocial discrimination. The IMCI framework was modified through 3 ways: i) identifying signs and symptoms of PTB, ii) emphasising the IMCI's 5 steps of integrated management: assess, diagnose, treat, counsel and detect, and iii) counseling on BCG immunisation, malnutrition, environmental modifications and stigma on PTB.
Keywords
Significance for public health
Controlling tuberculosis in high pulmonary tuberculosis (PTB) regions among marginalised islanders with limited health accessibility requires a concerted effort from the community and the healthcare system. An efficient implementation is through community empowerment by transferring adequate knowledge and skills on PTB detection and treatment within the community for reducing the spread of the disease. Developing a training module for the knowledge transfer purpose has to be contextually relevant and adapted to the lack of healthcare resources of the targeted region. Adapting Integrated Management of Childhood Illness (IMCI) framework for developing such training module is feasible for PTB and should be extended to other diseases.
Background
Sabah recorded the highest notification of (PTB) in Malaysia with a considerable proportion attributed to immigrants. 1 Strategies for PTB control are governed by the Ministry of Health and requires concerted efforts from healthcare providers for PTB control. 2 Yet, in regions with large populations and high influx of immigrants, re-emergence of PTB is very likely, hence the critical call for community empowerment through awareness and active participation to promote successful implementation of PTB control. 3 Community awareness and understanding of PTB lack in many aspects including knowledge, perceptions, health-seeking behaviour and impact of the disease. 4
Extensive studies on behavioural changes for healthy lifestyle practices among longhouse residents in Sarawak based on the Healthy Village program from WHO, demonstrated that health education and health promotion initiatives implemented at community setting do influence and improve health determinants such as smoking, exercise habit and environmental hygiene. 5 Nevertheless, creating culturally acceptable local policies and supportive environments aiming for beneficial health changes is made feasible through partnerships between health authorities and community participation.
Based on these principles, community empowerment strategies in controlling PTB have to incorporate three main domains; i) accurate detection of PTB cases, ii) delivering early PTB treatment and promoting compliance, and iii) strengthening PTB-related counseling for containing the disease within the community. These domains share similar concepts with the pillars of Integrated Management of Childhood Illness (IMCI), an integrated public health care strategy developed in 1995 as frameworks incorporating an algorithmic approach for delivering holistic care to combat major causes of childhood deaths globally. 6
IMCI emphasises 3 components: improving case management skills by health providers, overall health systems, and community health practices. A systematic review on IMCI implementation has shown a reduction in child mortality rates, and strategies evaluated include training of health care staff, management strengthening of health care systems and home visiting. 7 IMCI was not intentionally developed for PTB. However, it has been implemented in many developing countries like Ethiopia, Rwanda and Uganda for PTB case detection. 8
On this basis, Knowledge Transfer Program (KTP) for community empowerment was proposed to empower and change the community by addressing the gaps on PTB detection, communitybased TB treatment, environmental modification and advocacy on balanced nutrition. Community empowerment was aimed through identified community volunteers that were trained to be the health providers for PTB control in the targeted community. The objective of this article is to enlighten in detail the process of developing the training module for PTB control by adapting and modifying the IMCI framework, brief methodology on phases of knowledge transfer intended for empowering the marginalised urban island volunteers of Kampung Pulau Gaya Proper, and highlighting the potential short-term impact of this program.
Methods
Site of study and population
Pulau Gaya has at least a population of 15,000 in an area of 3,700 acres. The island is over-crowded, known to have influxes of immigrants, has poor basic sanitation, untreated water supply consumption and complicated with a staggering number of PTB cases and chronic malnutrition. 9 The targeted community for the community empowerment is Kampung Pulau Gaya Proper. It is one of the most established villages with a recognised leadership organisation. The majority of the community people work in the fishery and tourism field, but many were noted to be unemployed when the study was conducted.
The nearest health care facility to the island is situated in Kota Kinabalu, a capital on the mainland of Borneo Island, which is only accessible by sea via a journey of approximately 20-30 min. Due to the prominent PTB issue in the community, the regional health office visits the area on an interval basis and conducted PTB screening using a mobile x-ray machine. Back in October 2018, it was reported that an almost 10% of potential PTB cases were detected after a total of 347 chest x-rays screening were conducted. 10
Phases of knowledge transfer program for PTB control
The implementation of KTP was proposed into 3 phases: i) developing a training module for PTB control, ii) training workshop for the community volunteers, and iii) monitoring the impact of community empowerment.
Phase 1: Developing a training module for PTB control
This phase involved collaborative effort involving academicians with public health specialty from the local university and health officers from the regional health office. In this country, public health specialists are the responsible healthcare professionals involved in communicable diseases matters including tuberculosis. Preliminary environmental assessments at the study site found that the majority of the community lacked in health awareness on PTB with more than two positive cases were detected among the young generation. Based on the main community issues: living in overcrowding house, malnutrition, consuming untreated water, poor basic sanitation, and the lack of PTB health awareness, structuring knowledge and skills for PTB control were formulated by adapting the IMCI framework.
Structuring knowledge and skills for PTB control. The process of structuring knowledge and skills for PTB control was based on the main strategies carefully constructed and planned under the National Strategic Plan for TB Control 2016-2020. 11 The structure has to contain knowledge and skills for PTB detection, diagnosis, treatment monitoring, and counseling for PTB control.
Adapting IMCI framework for developing a training module. The original IMCI framework has instructions for identifying signs and symptoms of common paediatric health conditions, identifying serious illnesses and counseling on immunisation status. The first two emphasise on implementing 5 steps (assess, classify, treat, counsel and follow-up) as part of the integrated management. By adapting the original IMCI framework and incorporating the structured knowledge and skills for PTB control based in (i), a training module was developed.
Phase 2: Implementing training workshop sessions for the community volunteers
The training module developers engaged the community aiming to recruit 50 eligible volunteers through interview sessions. These volunteers were intended to be the recipients for the knowledge transfer and act as the healthcare providers for this community in controlling PTB. Eligibility criteria for selecting the volunteers included adults (18 years and above), intact cognition, not under active PTB treatment, and ability to communicate. The workshop was conducted in 8 sessions that incorporated knowledge sharing sessions and practical skills based on the developed training module, a visit to a Tuberculosis Unit, and an engagement with a local tuberculosis-advocate non-governmental agency.
A pre- and post-training questionnaire assessing the knowledge and attitude of the volunteers was formulated as a form of evaluating the short-term effectiveness of the training module conducted through the workshop. There were 30 and 22 items for the knowledge and attitude domains, respectively. All items in the knowledge domain is in the form of True or False questions and marked accordingly with a maximum score of 30. For the attitude domain, the volunteers corresponded using a 5-point Likert scale: ‘strongly disagree’ (score as 1), ‘disagree’ (score as 2), ‘less agree’ (score as 3), ‘agree’ (score as 4), and ‘strongly agree’ (score as 5). Total attainable score for the attitude domain is 110. Both domains were calculated into percentages and reported as means and standard deviations.
Phase 3: Monitoring the community empowerment
This phase involved implementing the adapted IMCI framework into action by the volunteers themselves after acquiring the knowledge and skills from the training module. Volunteers were taught to utilise the training module for documenting cases.
Results
This section describes the main outcomes from Phase 1 and Phase 2 of the implemented KTP in empowering the community for PTB control at Kampung Pulau Gaya Proper. The outcome from Phase 3 is shown through on-field participation with the community volunteers.
Phase 1: Training module for PTB control
Knowledge and skills for PTB control
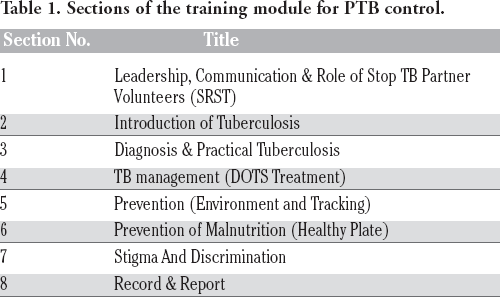
The knowledge and skills developed were developed for training through volunteer-centred learning activities including interactive lectures, group works, and hands-on demonstrations, roleplays and drama, video shows and quizzes. The developed module consisted of 8 sections (Table 1) that incorporated 5 knowledge and skills as follows:
Sections of the training module for PTB control.
Knowledge and skills on PTB disease and diagnosis. There were 2 major competencies that the volunteers have to acquire: i) knowledge and attitude towards PTB and ii) knowledge and skill of diagnosing PTB for active case detection. Basic skills to be learnt include identifying signs and symptoms of PTB, accurate sputum production technique, sputum storage for microscopic detection of acid-fast bacillus (AFB), procedural sessions for administering tuberculin skin injection, interpreting the tuberculin skin reaction, and understanding main pulmonary radiographic changes reported on the chest X-ray.
Knowledge and skills on PTB treatment. Volunteers have to learn to recognise common PTB medications, dosages and side effects, be competent in implementing Directly Observed Treatment for Short Course (DOTS) within the community, be skilful in monitoring affected community members’ compliance based on the TB treatment book, and able to counsel these people on drug-resistance PTB. These were conducted using real PTB cases in the community supervised by the academicians.
Knowledge and skills on preventive PTB measures. Environmental health officers educated the volunteers on the preventive PTB control measures including environmental modification for reducing over-crowding at home, cough etiquette, handwashing technique and face mask application for individuals with PTB. Volunteers learnt to counsel the community on PTB primary prevention with Bacillus Calmette- Guerin vaccination and were trained on intensified case finding (ICF).
Knowledge and skills on the prevention of malnutrition. Volunteers were educated on the significance of preventing malnutrition for reducing the risk of developing PTB among individuals with low immunity through didactic lecture. In addition, hands-on skills imparted included nutritional assessment through body mass index measurement, counseling on balanced dietary intake, monitoring children's’ growth, and counseling on promoting breastfeeding. Volunteers were trained to conduct live demonstrations on food preparation and cooking within the community as part of the health promotion.
Knowledge and skills on psychosocial discrimination. Volunteers were exposed to potential social stigma and discrimination experienced by confirmed PTB cases and their caregivers. Similar to the health education on HIV counseling within the original IMCI framework, for this module, volunteers were trained to counsel community members on PTB and advice on reducing negative perceptions in the community. Role-play sessions and small group discussions strategies were implemented for instigating this skill.
Adapted IMCI Framework for PTB control training module. The training module for PTB control through community empowerment was developed through 3 modifications of the original IMCI framework: i) identifying signs and symptoms of a single health condition (i.e. PTB), ii) emphasising on 5 steps (assess, diagnose, treat, counsel and detect) as the integrated management, and iii) assessment and counseling on BCG immunisation, malnutrition, environmental modifications and caregivers’ stigma on PTB (Figure 1). Based on the adapted IMCI framework, the structured knowledge and skills for PTB control were incorporated in the 5 steps of integrated management (Figure 2).

The modifications of the 5 steps of integrated management based on the original IMCI framework.

The knowledge and skills incorporated in the training module based on the modified IMCI framework.
Phase 2: Training workshop for the community volunteers
A total of 39 community members were recruited based on the eligibility criteria, and they were called as Sukarelawan Rakan Stop Tibi (SSRT), translated as Stop TB Partner Volunteers. The training workshop was conducted through a total of 8 sessions within a span of 3 months beginning March 2017 using the developed training module as the guidance. Both the knowledge and attitude domains among the volunteers have demonstrated significant improvement at post-training (Table 2).
Pre- and post-training assessment on knowledge and attitude among the community volunteers.

Phase 3: Community empowerment by the volunteers
The training module developers monitored the process of the trained volunteers empowering the community on several sessions, including health education talks, nutritional demonstrations, and PTB cases detection (Figures 3 and 4).

Knowledge sharing between trainers and the community volunteers in one of the training workshop sessions.

Healthy food preparation demonstration by the volunteers to the community.
Discussion
Major immediate health impacts observed through this KTP are the ability of these volunteers to detect and diagnose PTB, monitor DOTS treatment, counsel the members of the community on preventing PTB spread and malnutrition. The developed training module has shown to be effective in short-term for improving the knowledge and attitude of the trained community volunteers in the effort to impart knowledge and skills through KTP. The module was successful in moulding new healthcare providers for PTB control in the community setting based on the adapted IMCI framework. However, this evaluation was conducted among a single set of community members with a relatively small number of volunteers. Such form of assessment on the knowledge and attitude would, therefore, require a more robust form of evaluation before implementing the KTP at a larger scale. Although our study evidently showed significant changes statistically, the differences have to undergo a more thorough analysis with a larger sample population to ensure the differences are meaningful from the public health perspective.
The feasibility for adopting IMCI framework is influenced by healthcare facilities availability, resources for cultivating skills among health care workers, strengthening health care systems through supported supervision, and counseling of caregivers for community health practices. 12 However, within community settings with limited health accessibility, implementing the IMCI framework is made feasible through transferring knowledge to the community. 13 The idea is to empower the community through education and training with equivalent knowledge to act as the frontline health workers so that the IMCI strategy can be implemented despite limited access to healthcare. This acts as the motivational drive in our study to successfully develop the training module by adapting the IMCI framework.
Although this study has demonstrated a positive short-term impact among the trained community volunteers, further evaluations on a wider scale and longer-term health impacts of implementing such KTP are warranted. Looking from the public health perspective, two major indicators to be evaluated are the figures of PTB cases detected, and the number of PTB treatment failure in the community. These data require permission and collaboration with the centralised health governments in which this information is not readily available at the time of writing. It is stipulated that the KTP should yield a higher positive PTB cases detection and a lower rate of PTB treatment failure from poor medications compliance. We did not achieve the targeted number of volunteers, and the extend of the community empowerment from this KTP was solely focused in the nearby villages, hence not covering the whole island. For this reason, it is probably that the indicators would change as stipulated but might not reach a significant difference statistically. A longitudinal study on a larger scale is needed to objectively demonstrate long-term health impact from such KTP.
Empowering the volunteers through KTP for educating the community members based on adapted IMCI framework would benefit the key players; the volunteers, the community, and the academicians. This training module is developed in such a way that the content delivered during the KTP can be accepted by those with a lower level of education than the expected academic background required for healthcare professionals. As the IMCI framework emphasises on the 5 steps of integrated management in managing a health condition, it is vital that specific knowledge and skills are embedded into the training module to ensure reasonable but relevant information are transferred to the volunteers. The content thus remains medically relevant while avoiding high levels of complexity that would demotivate the learner. Theoretically, applying the modified IMCI framework as the basis for developing the training module can be viewed as a comprehensive approach due to its integrated management concept. 14 The practicality of the module requires the volunteers to cultivate leadership skills and communication abilities in order to engage with the community members.
From a more holistic point of view, successful implementation of this program would increase the level of community awareness towards PTB, including understanding the disease and related treatments, the complications among affected individuals and the impact to the community if preventive measures are not instigated. Attaining such level of community awareness would enhance collective efforts for the betterment of societal health needs through people-centred healthcare systems. 15 Hence, these benefits should be extended towards communicable and non-communicable diseases. On that note, more opportunities for academic-community partnership should be fostered in the effort to tackle other prevalent health issues, for instance, leptospirosis, stroke and mental health illness.
One unique distinguishing factor of this developed training module is that it places additional emphasis on psychological issues, which are not prioritised in the IMCI framework. Psychological stigma towards PTB has been a subject of interest not only to healthcare professionals but also to governing authorities. Casual transmission as a mode of contagion spread is one big factor within public stigma towards TB. 16 This stigma can be ascribed through three attributes; controllability (one's aptitude for controlling tuberculosis from infecting others), responsibility (being responsible on the infection such as compliance towards treatment), and blame (accepting that the infection occurred due to own fault). 17 To alleviate such public stigma, it would be highly relevant to integrate psychological domains as part of the training module.
In contrast to the IMCI framework that can be trained as a distance- learning module, the training module developed specifically to empower the community for PTB control has to be implemented through series of hands-on workshop sessions for the volunteers. Hence, one foreseeable challenge with this form of KTP is the issue of sustainability. Continuous monitoring by the health authorities and community leaders is essential to ensure that long term provision of this program is feasible and accountable. Fiscal analysis of implementing such KTP is warranted for an objective appraisal of its cost-effectiveness, due to a significant proportion of the module that requires practical and hands-on sessions, before implementing such program at a larger scale. 18
Conclusions
IMCI framework can be adapted for training volunteers in the community with limited access to healthcare facilities. The original framework is modified to be compatible with adult and for pulmonary tuberculosis. Feasibility of adapting modified IMCI framework to other communicable and non-communicable diseases should be explored as a feasible solution to promote better health among minority and marginalised people with limited health accessibility. Further works are needed to demonstrate long term health impact and cost-effectiveness of implementing such a program in the community.