
Abstract
Background
High cancer mortality is a major source of burden. Population-wide programs have been developed to improve cancer outcomes, and although effective in improving outcomes overall, the socioeconomically disadvantaged population have disproportionately benefited. This systematic review evaluated interventions aimed at addressing inequalities in cancer-related outcomes between low and high socioeconomic groups within high-income countries.
Materials and Methods
The Cochrane Register of Controlled Trials, EMBASE, and PubMed searches were completed in October 2018. Data extraction and quality appraisal were guided by established mechanisms. Impact of interventions, using odds ratios, with respective 95% confidence intervals were presented, where available.
Results
Sixteen studies reporting on 19 interventions were included. Seven interventions (37%) reduced socioeconomic inequalities in cancer-related outcomes, focusing on participation in cancer screening. Interventions included pre-formulated implementation intentions; GP-endorsed screening invitations; enhanced reminder letters; text message reminders; and implementation of an organised screening program.
Conclusions
This systematic review found limited evidence on the efficacy of existing interventions that aimed to reduce inequalities in cancer-related outcomes between people living in low and high socioeconomic areas among high-income countries. Future interventions should consider the specific needs of people living in socioeconomically disadvantaged areas to improve the efficacy of an intervention.
Significance for public health
Australia's health system and public health programs have facilitated improvements in cancer outcomes over time. Disadvantaged populations have lower engagement with services and participation in programs, reflective in their worse outcomes and driving disparity between low and high socioeconomic groups. This is a trend in Australia and internationally. The study evaluated interventions aimed at reducing socioeconomic inequalities in cancer-related outcomes within highincome countries. All effective interventions focused on cancer screening participation and reported improvements, decreasing the risk of dying from screen-detected cancer. Lower uptake remained for low socioeconomic groups. The review demonstrated that interventions must be designed to meet the health literacy needs of the population and that they need to be engaged throughout the developmental phase for uptake to improve. Understanding the characteristics of successful and unsuccessful interventions is the first step in ensuring scalability, and therefore, is of public health importance to acknowledge well-planned interventions that have utilised resources effectively.
Introduction
Cancer is the second leading cause of death, responsible for 9.4 million deaths worldwide. 1 This places significant burden on individuals and healthcare systems. Population-wide programs have been developed by many countries to increase early detection and diagnosis of cancer, and accessibility to treatment to improve cancer outcomes, such as survival and mortality.
In Australia, these programs have been effective in improving cancer outcomes overall, but improvements have been disproportionate for the socioeconomically disadvantaged population; the same pattern also clear, internationally. A United States study reported that when screening is provided at no cost, low socioeconomic groups still report lower screening uptake. 2 Personal and structural barriers experienced by low socioeconomic groups could be underlying factors influencing the extent to which they benefit from an intervention. These factors may include fears and attitudes of undergoing a clinical examination, perceived costs, time off work, lack of transport, and difficulty navigating a complex healthcare system. 3
An area-based measure is one of many measures of socioeconomic status representing the environmental, social and geographical conditions of individuals and households of a specified area, including individual-level information on income and employment. 4 Socioeconomic Indexes for Areas are used in Australia to represent relative disadvantage (or advantage) of specified areas. 4 Other area-based measures of socioeconomic status exist, such as England's Indices of Multiple Deprivation which indicate relative deprivation of small areas and the influence of crime, health, housing and living environment conditions on an individual's health outcomes. 5 High socioeconomic groups benefit from an intervention to a much greater extent than low socioeconomic groups, when initially implemented, leading to socioeconomic inequalities widening. 6 Poor health literacy influences an individual's ability to respond to large amounts of written material, and for low socioeconomic groups, information delivered multiple times, using different mediums may be beneficial. 7 Understanding the characteristics of an intervention that has been, both successful and unsuccessful, in reducing socioeconomic inequalities in cancer outcomes is critical.
This systematic review evaluated interventions aimed at addressing inequalities in cancer-related outcomes between low and high socioeconomic groups within high-income countries. The intention is to provide Australia and other high-income countries with examples of ways to manage social equity relating to cancer outcomes for low socioeconomic groups effectively.
Materials and Methods
Search strategy
The Cochrane Register of Controlled Trials, EMBASE and PubMed databases were systematically searched to identify interventions for inclusion. Key search terms included cancer, intervention and socioeconomic disadvantage. The search strategy was completed in October 2018.
Reference lists of all eligible studies were reviewed to identify any potential studies not detected through the above process.
Inclusion and exclusion criteria
Criteria for inclusion were: i) an area-based measure of socioeconomic status; ii) participants in low and high socioeconomic groups within a high-income country, which was defined as a Gross National Income per capita of $12,058 or more; 8 iii) participants diagnosed with cancer or in a population at risk of developing cancer; iv) intervention focused on early detection and diagnosis of cancer or health service utilisation; v) primary outcomes were cancer mortality and survival, and behavioural change; Quality of life (QoL) was the secondary outcome; vi) papers published between 2008 and 2018; and vii) papers available in English.
Experimental and non-empirical studies including editorials, letters, commentaries and narrative reviews were excluded from selection.
Screening and data extraction
AB performed the literature search. AB and KW undertook initial screening of the papers based on title and abstract. Disagreements were discussed and resolved through consensus. AB then assessed the full text of the studies using the eligibility criteria described above.
The following data were extracted from each study: i) country of origin; ii) aim; iii) participant characteristics (sample size, gender and age); iv) patient diagnosis; v) study design; vi) intervention details (format, content, setting, duration, who delivered the intervention); vii) theory underpinning the intervention; viii) comparison conditions; ix) outcome measures; and x) key findings.
AB completed all data extraction, with a sample of 25% of studies extracted by KW. Deferring to KW for the remaining papers was considered unnecessary because no discrepancies between reviewers were found.
Assessment of risk of bias
The methodological quality of each study was independently assessed by AB and KW using the National Health Medical Research Council's level of evidence and Cochrane's risk of bias tool. 9 Areas assessed for risk of bias included: i) sequence generation; ii) allocation sequence concealment; iii) blinding of participants and personnel; iv) blinding of outcome; v) incomplete outcome data; vi) selection outcome reporting; and vii) other potential sources of bias. Disagreements were discussed and resolved through consensus. No studies were excluded based on quality appraisal.
Data analysis and presentation
Analyses were carried out by outcome measured, and these included interventions which aimed to improve: i) attendance to screening; ii) adherence to appointments; iii) cancer survival; and iv) quality of life.
Synthesis of the impact of interventions, using odds ratios (ORs) with respective 95% Confidence Intervals (CIs) were presented, where available.
Results
Study selection
A flowchart of the study selection process is presented in Figure 1. The electronic database search identified 10,138 records. Duplicates were removed, and 7,133 titles and abstracts were screened. Two hundred and seventy-nine full-text papers were reviewed. A total of 16 studies reporting on 19 interventions were included.
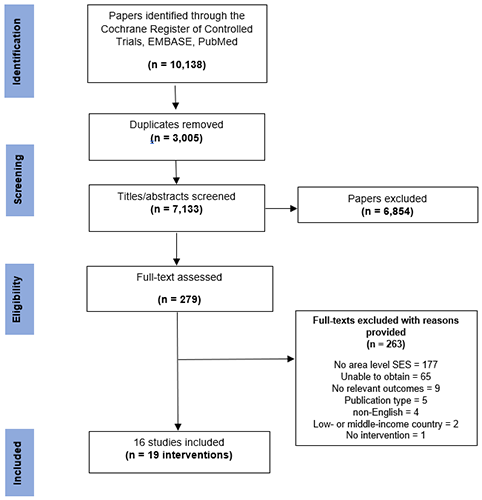
Inclusion and exclusion process.
Risk of bias
Randomised controlled trials or controlled trials were at risk of bias based on AB and KW assessments due to highly selective recruitment methods, incomplete follow-up data, and no masking or blinding techniques. Methodological review findings are presented in Table 1.
Quality assessment for randomised controlled trials or controlled trials.

RCT, randomised controlled trial. Studies assessed using the Cochrane criteria for assessing risk of bias. Four studies were excluded from this analysis because they did not use an RCT or CT design.
Study characteristics
For an overview of study characteristics (n=16), including the intervention type and content see Table 2.
Selected study and intervention characteristics.

NR, not reported; RCT, randomised controlled trial; IRSAD, index of relative socioeconomic advantage and disadvantage; POAs, postal areas; CRC, colorectal cancer; gFOBt, guaiac faecal occult blood test; IMD, Index of Multiple Deprivation; BCSP, bowel cancer screening program; NHS, National Health Service; GPE, general practitioner endorsed; LSOA, lower support output area; CCS, cervical cancer screening; BCS, breast cancer screening; FCS, female cancer screening; OECD, Organisation for Economic Co-operation and Development; SED, socioeconomic disadvantage; FOBt, faecal occult blood test.
Country of origin
Eight high-income countries were represented in this review: England (n=8),10-17 France (n=2),18–19 Australia (n=1), 20 Italy (n=1), 21 Japan (n=1), 22 Portugal (n=1), 23 Singapore (n=1), 24 and the United States (n=1). 25
Study design
Eleven studies were RCTs.10-12,14-19, 23, 25 The remaining were cohort studies (n=4),13,20–21,24 and a quasi-experimental design (n=1). 22 Study duration including follow-up, ranged from 10 days to 75 months.
Participant characteristics
Thirteen studies targeted specific population age groups,10-20,22,23 two recruited participants with a diagnosis of cancer,21,25 and one involved citizens or permanent residents of a country. 24 Median number of study participants was 28, 929 (IQR 2,636-163,525). Most participants in studies were females.
Intervention characteristics
Some percentages exceeded 100% as many interventions (19 in total) involved multiple types of content or were delivered to different settings.
Nearly all interventions (n=16, 84%) improved attendance at cancer screening.10,12-20,22-24 The remaining (n=3, 16%) were designed to improve adherence to appointments, 11 cancer survival, 21 or quality of life. 25 Fourteen (74%) were implemented into existing national cancer screening programs.10–11,13-20,23
Some form of targeted or tailored education was used: fourteen (74%) provided information about the interventions, reporting on the format, content and complexity;10-14,17-20,22–23 ten (53%) involved health professionals and individuals providing feedback or counselling;14-19,25 three (16%) delivered social support in the form of outreach;18–19,24 and one (5%) used self-tracking for symptoms monitored by health professionals. 25 Interventions were directly delivered to study participants. Twelve (63%) were received by mail,12-19,22 and three (9%) delivered face-to-face to participants.18–19,24 Seven interventions (37%) were delivered to study participants by health professionals, such as general practitioners, nurses or social workers.16-19,23-25 Research assistants and medical students also distributed interventions (n=5, 26%).10,15,17,24–25 Two studies (11%) specified following a theory or framework when developing their interventions, such as a stepwise strategy, 23 and the Fuzzy-Trace theory. 17
Impact of interventions on socioeconomic inequalities in cancer-related outcomes
Seven interventions in six studies reduced socioeconomic inequalities in cancer-related outcomes. These reported on cancer screening outcomes, with five (71%) focusing on the National Health Service Bowel Cancer Screening Program. To determine whether an intervention reduced inequalities in cancer-related outcomes between low and high socioeconomic groups, the following criteria needed to be met: i) the cancer-related outcome improved for low socioeconomic groups at a greater rate than high socioeconomic groups; ii) the gap between low and high socioeconomic groups reduced by ≥1%; and iii) for high socioeconomic groups, the change in outcome could not be detrimental for the population and therefore, needed to remain relatively stable, a negative change ≤10%.
All results have been reported on, including interventions that did not reduce socioeconomic inequalities between low and high socioeconomic groups to understand what, and what did not work.
Interventions which aimed to improve attendance to cancer screening
Additional information material
Four RCTs in three studies evaluated the impact of supplementary material to the National Health Service Bowel Cancer Screening Program on faecal occult blood test uptake.12,14,17
An interaction between pre-formulated implementation intentions, addressing the common barriers to colorectal cancer screening, and Index of Multiple Deprivation quintile was observed (p<0.05). 14 The study reported an increase in the odds of participation in the most deprived tertile (OR 1.10, 95% CI 1.01-1.21; p<0.05), but decrease in the least deprived tertile (OR 0.92, 95% CI 0.82-0.99; p<0.05). 14
An RCT that summarised key colorectal cancer screening information was evaluated using a simplified screening information leaflet that could be understood by readers with low literacy, numeracy, or both. 17 The study found an insignificant increase in the odds of participation among both quintiles (p=0.68), with the least deprived quintile demonstrating the greatest benefits in participation (least deprived: OR 1.06, 95% CI 1.01-1.11 and most deprived: OR 1.04, 95% CI 0.96-1.12). 17
Two trials also evaluated the impact of a narrative-based leaflet, and concluded that the intervention reduced the odds of participation in the least (OR 0.98, 95% CI 0.93-1.04; p=0.57) and most deprived quintiles (OR 0.92, 95% CI 0.86-0.98; p=0.02).12,17
Community-based
A cohort study evaluated the impact of an access-enhancing, outreach intervention offering convenient screening for colorectal, breast and cervical cancer on participation in Singapore. 24 Statistically significant increases of 19% and 28.2% were recorded in faecal occult blood test rates (p<0.001), 17.4% and 16.9% in mammography rates (p=0.001), and 25.4% and 47.3% in Pap-test rates (p=0.001) for rental (low socioeconomic status area) and owner-occupied flat dwellers (high socioeconomic status area), respectively. 24
GP-endorsed invitation
Two RCTs evaluated the impact of a GP-endorsed bowel screening invitation on faecal occult blood test uptake in England.16–17 Odds in participation increased for the most (OR 1.07, 95% CI 1.01-1.13; p=0.02) and least deprived quintiles (OR 1.04, 95% CI 0.99-1.08; p=0.08).16–17 The interaction between intervention and Index of Multiple Deprivation quintile was insignificant (p=0.49).16–17
Mass media campaigns
A cohort study evaluated the impact of a mass media campaign on uptake of Pap tests in Australia. 20 Number of women who had a Pap test increased in low and high socioeconomic status areas during the campaign period from 57 to 73 per 100,000 and 76 to 97 per 100,000, respectively. 20
Patient navigation
Two RCTs evaluated the impact of a patient navigation program on faecal occult blood test uptake in France.18–19 Following the initial screening invitation letter, social workers provided navigation services to patients, such as telephone follow-up and home visits to identify barriers to screening, and promote participation. Navigation had a greater impact on the affluent strata, compared to the deprived strata within the target screening population.18–19 Participation increased in the affluent strata by 4.1% (p=0.01), and in the deprived strata by 2.6% (p=0.07) in one study. 18
Reminders
Two RCTs evaluated the impact of an enhanced reminder letter on faecal occult blood test uptake in the National Health Service Bowel Cancer Screening Program.15,17 This consisted of adding a simplified language restatement of the screening offer at the end of the standard screening invitation letter, in addition to a banner at the start which read ‘A reminder to you’. There was an interaction between intervention and Index of Multiple Deprivation quintile (p=0.005), with an 11% increase in the odds of participation in the most deprived quintile (95% CI 1.04-1.20; p=0.003) and no increase in the least deprived quintile (OR 1.00, 95% CI 0.94-1.06; p=0.98).15,17
Another trial evaluated the impact of a text message reminder on faecal occult blood test uptake in England and concluded that among the most and least deprived quintile no improvements were reported. 10 Text-message reminders were sent to patients who had not returned their faecal occult blood test kit within 7-weeks of their receiving the first invitation in the mail. A lower proportion of adults in the most deprived quintile returned a faecal occult blood test kit in the intervention than control arm (OR 0.88, 95% CI 0.62-1.27; p=0.50). 10
A single RCT evaluated the impact of automated and customised text messages, phone calls and reminders on the proportion of women within the target group adherent to cervical cancer screening in Portugal. 23 The screening invitation was sent as a text message 45-days prior to the appointment and customised with the woman's first and last name, name of the primary care unit and appointment date and time. Women were requested to confirm their appointment by texting back, and if a woman did not reply after two text-message reminders, an automated and customised phone call was performed. Although adherence to screening was significantly higher among women allocated to the intervention both in a more deprived area (OR 2.05, 95% CI 1.30-3.21; p=0.002), and less deprived area (OR 1.91, 95% CI 1.31-2.77; p<0.001), the inequality increased slightly. 23
Reducing logistical barriers
A cohort study evaluated the impact of three biennial invitation rounds on uptake in the National Health Service Bowel Cancer Screening Program. 13 Socioeconomic inequalities in uptake persisted across the invitation rounds with greater increases in participation reported for the least deprived quintile (10.8%), compared to the most deprived quintile (7.5%). 13
Removal of out-of-pocket costs
A quasi-experimental study evaluated the impact of removing out-of-pocket costs for Pap tests and mammography on screening uptake in Japan and concluded that socioeconomic inequalities in attendance for mammography reduced (ranging from – 12.9 to – 74.1%), but inequalities in Pap test attendance increased (+100%). 22
Interventions which aimed to improve adherence to appointments
An RCT evaluated the impact of delivering text message reminders to women due for their first breast screening appointment in England. 11 On an intention-to-treat basis, the most deprived quintile benefited from receiving a text message reminder before their first appointment, with an absolute increase in attendance of 13.6% (OR 1.75, 95% CI 0.88-3.51; p=0.11). 11 Whereas for the least deprived quintile adherence to first appointments decreased by 6.5% (OR 0.73, 95% CI 0.47-1.15; p=0.18). 11
Interventions which aimed to improve cancer survival
A cohort study evaluated the impact of implementing an organised mammographic screening program in Italy on 10-year breast cancer survival among women aged 50-69 years, compared with pre-screening groups. 21 Breast cancer survival increased from 52% to 87%, 10-years after the program's introduction for the deprived class (third tertile), and from 64% to 86% for the reference class (first and second tertile). 21
Interventions which aimed to improve quality of life
An RCT evaluated the impact of a telephone care management intervention for participants with cancer-related pain in the United States. 25 Participants with lower socioeconomic status were less likely to experience improvement in cancer-related pain than higher socioeconomic status (OR 0.73, 95% CI 0.56-0.94), but this was insignificant (p=0.016). 25
Discussion
Although all interventions included aimed to address socioeconomic inequalities in cancer-related outcomes between low and high socioeconomic groups, only seven were successful. Most studies were at risk of bias, which reduced the conclusiveness of findings. However, interventions that were added to existing national bowel (colorectal) screening programs had an influential impact on inequalities.
The delivery of interventions to study participants varied, making it difficult to determine modes most appropriate for low socioeconomic groups and their needs. Sending screening notification letters in the mail and text message reminders appeared to have greater effects for low socioeconomic groups compared to high socioeconomic groups. Given low socioeconomic groups are less likely to participate in cancer screening programs, this result is promising. Although the differences in these effects were not large enough to have a significant impact, with improvements ranging from 0.8% to 3.6%. Many countries already send bowel cancer screening invitations in the mail to age groups at highest risk, so utilising this delivery mode requires minimal work to offer it to disadvantaged populations due to existing infrastructure.26–27 Considering different strategies to encourage low socioeconomic groups to engage with interventions that require behavioural change should be prioritised. Smith et al., (2011) reported that low socioeconomic groups are more likely to text message compared to high socioeconomic groups, supporting the findings that using mobile phones to deliver text message reminders for screening may be suitable for this population, prompting responses. 28
Several strategies for informing interventions were evaluated, with many implemented into differing contexts and reporting mixed results. The review found that interventions which considered the common barriers to cancer screening may be a useful strategy in addressing socioeconomic inequalities in participation. Enhanced reminder letters and GP-endorsed screening invitations significantly reduced inequalities in faecal occult blood test uptake between low and high socioeconomic groups, reflecting on the barriers low socioeconomic groups face when accessing early detection and diagnostic services.15-17 Although interventions that used supplementary material, in addition to England's existing Bowel Cancer Screening Program information were largely unsuccessful in reducing socioeconomic inequalities, pre-formulated implementation intentions that specified the when, where and how a behaviour can be modified demonstrated the potential to be successful in greatly improving outcomes for low socioeconomic groups, and therefore reducing socioeconomic inequalities. 12 Interventions that consider the barriers low socioeconomic groups experience in accessing cancer screening services at the developmental phase, as well as the enablers, may have a greater success rate. Although designed to address the needs of people from low socioeconomic groups, it is important to ensure that an intervention which improves cancer-related outcomes for low socioeconomic groups is not at the detriment of other populations and has the possibility to be beneficial for people across all socioeconomic gradients.
Understanding the impact these interventions had on long-term behaviour change were limited because of intervention duration. Narrative-based and informational leaflets with simplified language were run over 10 consecutive days,14,17 and enhanced reminder letters and GP-endorsed screening invitations ran over 20 consecutive days.15-17 No such discussion regarding the reasons for choosing this duration and frequency were provided. Comparing these studies to the study that evaluated the implementation of an organised mammographic screening program over 10-years, 21 implies that short-term interventions are inadequate in developing long-term behaviour change (Done et al., 2011). 29 To ascertain this, longer intervention and follow-up periods need to be implemented, irrespective of the findings in this review, to ensure improvements reported can be maintained for a prolonged period.
A negative effect was reported for some interventions, where uptake was lower among low socioeconomic groups compared to the control group. There are complexities involved in engaging with this population in behavioural change interventions, such as poor health literacy skills.5,30 This was demonstrated in a study that evaluated a narrative-based information leaflet. It was found that for low socioeconomic groups faecal occult blood test uptake reduced from 46% to 42.4%, which could be explained by increased amounts of written material.14,17 The material had to be added to the existing informational material, and for people with lower educational attainment and income (both indicative of socioeconomic disadvantage) are less likely to understand the importance of engaging with health services. 5 Minimising the cognitive effort needed to comprehend an intervention provides low socioeconomic groups with the opportunity to participate. 3 Visual aids with clear and evidential messages should be encouraged to communicate complex, but understandable health information to disadvantaged populations.
Study limitations
The review has some limitations to consider. Firstly, interventions with similar cancer-related outcomes were measured or reported on differently, which made it difficult to summarise the interventions impact. Secondly, the review was subject to some methodological limitations, with many underreporting methods and therefore, building on or replicating interventions was problematic. Thirdly, area-based measures of socioeconomic status were central to this review but the effect of individual components of socioeconomic status were under-estimated. Although this was outweighed because area-based measures provide insights into socioeconomic variations at a geographic level.
Conclusions
Few studies have utilised an area-based measure to account for differences in cancer-related outcomes by socioeconomic status, however, social determinants of health, including where people reside, are known to influence the ability to access health services and cancer outcomes. This systematic review found limited evidence on the efficacy of existing interventions that aimed to reduce inequalities in cancer-related outcomes between people living in low and high socioeconomic areas among high-income countries. The findings suggest that interventions added to existing population- based programs or services, and provision of resources that are developed to support people with low literacy and numeracy skills have the potential for improving outcomes among low socioeconomic groups, as well as reducing inequalities between low and high socioeconomic groups. This indicates that future interventions should consider the specific needs of people living in socioeconomically disadvantaged areas to improve the efficacy of an intervention.
Footnotes
Acknowledgements
The authors would like to thank Professor Jon Emery, Professor Meinir Krishnasamy, Associate Professor Roger Milne and Mr Paul Grogan for their support and advice during the planning of the project. The authors would also like to thank Dr Albert Chetcuti for reviewing the literature search strategy, and Ms Megan Varlow for reviewing the manuscript paper.