
Abstract
Background
We examined paradoxical and barrio advantaging effects on cancer care among socioeconomically vulnerable Hispanic people in California.
Methods
We secondarily analyzed a colon cancer cohort of 3,877 non-Hispanic white (NHW) and 735 Hispanic people treated between 1995 and 2005. A third of the cohort was selected from high poverty neighborhoods. Hispanic enclaves and Mexican American (MA) barrios were neighborhoods where 40% or more of the residents were Hispanic or MA. Key analyses were restricted to high poverty neighborhoods.
Results
Hispanic people were more likely to receive chemotherapy (RR=1.18), especially men in Hispanic enclaves (RR=1.33) who were also advantaged on survival (RR=1.20). A survival advantage was also suggested among MA men who resided in barrios (RR=1.80).
Conclusions
The findings were supportive of Hispanic paradox and MA barrio advantage theories. They further suggested that such advantages are greater for men, perhaps due to their greater spousal and extended familial support.
Significance for public health
Hispanic Americans are three-times as likely to live in poverty as non-Hispanic white Americans. Despite this, Hispanic enclaves, Mexican American barrios, in particular, seem to be relatively protective. Considering cancer care in California, for example, Hispanic men who live in such Hispanic enclaves/barrios are particularly advantaged in their access to cancer care and survival. Such communities may effectively double the protective effects of familialism that many Hispanic men already enjoy through marriage.
Introduction
Kyriakos Markides and Jeannine Coreil's germinal paper suggested the Hispanic paradox theory and began a generation-long debate on its soundness. 1 They described diverse morbid and mortal advantages among Hispanic people, many of whom lived in Hispanic enclaves, especially in barrio neighborhoods prevalently populated by first generation immigrants from Mexico. The related barrio advantage theory suggested that though barrios tend to be high poverty places, they provide their residents with relatively more supports. 2 They may have more social capital than other neighborhoods; their residents, including extended family members, assisting each other with direct and indirect health care costs. Pointing toward hopeful notions of cultural strengths and resiliencies the theory has much appeal and evidence has been produced in support of it. 3 Some credible studies have not supported it however, inferring that the phenomenon is well-explained by methodological artifacts.
A few studies found evidence of the Hispanic paradox only among the socioeconomically vulnerable with low incomes or the uninsured. 4 Such analyses seemed especially intriguing and were clearly important as Hispanic Americans are not a homogeneous population. Though statistically powerful, those analyses were limited in several ways. First, they did not study poverty, per se. Second, they focused on all-cause mortality. Third, their models controlled for personal and contextual characteristics that might be better described. We aimed to create complimentary knowledge with a descriptive epidemiologic approach, focusing on treatment access and survival among the most socioeconomically vulnerable people with colon cancer.
Prevalent among Hispanic and Non-Hispanic White (NHW) women and men, colon cancer is treatable when diagnosed early. 5 Studies of cancer have ranged from highly supportive of the Hispanic paradox to counter-hypothetical. Those studies tended to suffer the same limitations of the field in general. Our research group studied colon cancer care in California and Ontario and observed that the more impoverished were the people and places, the larger was the Canadian universal health insurance-based advantage. 6 Focusing on the most vulnerable patients seemed to magnify policy and human significance. The same likely analogously applies to study of the Hispanic paradox, a notion that we had a secondary opportunity to analyze. Because we oversampled people with colon cancer in California's poorest neighbourhoods we also oversampled Hispanic people, including MAs. Consequently, we hypothesized no Hispanic/NHW differences among the socioeconomically diverse. But among the socioeconomically vulnerable, principally the poor and inadequately insured, we hypothesized paradoxical colon cancer treatment and survival advantages of being Hispanic and living in a Hispanic enclave.
Methods
A registry-based colon cancer cohort of 6,300 people was established in California between 1995 and 2000, joined to the 2000 census by census tracts and followed until 2015. A third of them were randomly selected from high poverty neighbourhoods (>30% poor), the remainder equally from these strata: 5% to 29% or <5% poor. This secondary cohort was restricted to 3,877 NHW and 735 Hispanic people. A sample of 201 MAs were identified through medical records or with a validated algorithm using Hispanic names, birthplace and other record linkages (sensitivity = 84%, specificity = 99%). 7 Hispanic enclaves and MA barrios were defined as neighborhoods where 40% or more of the residents were Hispanic or MA as this was the most predictive criterion. Inadequate health insurance was defined as uninsured or Medicaid-insured. Age can confound any cancer analysis and chemotherapy was indicated experimentally, therapeutically or as palliation for stages II, III or IV colon cancer. Therefore, all rates were age and stage-adjusted and reported as percentages. Surgery was received by 9 of every 10 of the study participants and did not differ significantly by ethnicity or poverty so we did not analyze it. Five-year survival analyses included stages I to IV to account for diagnostic and treatment differences. Standardized rate ratios (RR) were reported with 95% confidence intervals (CI). Exploratory analyses of small subsamples reported 90% CIs. Further methodological details were reported.6,8 The original study was reviewed and cleared by the University of Windsor research ethics board.
Results
Cohort description
Hispanic people, generally, and MAs, specifically, were threetimes more likely to live in high poverty neighborhoods, and three to five-times more likely to live in Hispanic enclaves or MA barrios and to be inadequately insured. Furthermore, annual household incomes among Hispanic people and MAs were much lower than those of NHW people. Respective mean incomes in neighborhoods were $36,845 and $34,365 vs $55,310; both P<0.001. Being much younger than their NHW counterparts, members of both Hispanic samples were more likely to have never been married and less likely to be widowed. Restricting cohorts to those living in high poverty neighborhoods resulted in NHW, Hispanic and MA samples that were quite similar economically and biologically. Their average incomes did not differ significantly ($23,340 and $23,450 vs $23,850) and their tumors were of similar stages and grades. Both ethnic minority groups, however, were still two to three-times more likely to be inadequately insured.
Protections associated with being Hispanic or living in a Hispanic enclave
Findings related to the receipt of chemotherapy and 5-year survival are respectively displayed in the top and bottom of Table 1. First displayed are analyses of the overall samples. Among these overall samples, no significant differences were observed between either the Hispanic or MA and NHW groups. Hispanics of diverse national origins, MAs and NHWs with colon cancer enjoyed equal access to chemotherapy and were equally likely to be alive five years after their diagnoses. Next, we examined the possible protections of being a Hispanic person or of living in a Hispanic enclave among the socioeconomically vulnerable. No such Hispanic enclave or barrio advantages were observed among female or male NHW participants. They were the comparison group for these analyses. In high poverty neighborhoods, Hispanic people were more likely to receive chemotherapy (RR=1.18) a benefit that was most pronounced among Hispanic men residing in Hispanic enclaves (RR=1.33). A similar pattern was observed for survival among the poor. Hispanic men residing in Hispanic enclaves seemed most advantaged (RR=1.20). Among the inadequately insured, MA women seemed quite advantaged on chemotherapy access (RR=1.43). In fact, this advantage was most pronounced for MA women who lived in poverty and were inadequately insured (RR=2.05, 95% CI 1.09, 3.86, data not shown). Advantaged survival among MA men residing in barrios was also suggested (RR=1.80).
Description of the protective effects of being Hispanic or living in a Hispanic enclave by gender on the receipt of chemotherapy and 5-year survival among people with colon cancer (N = 4,612).
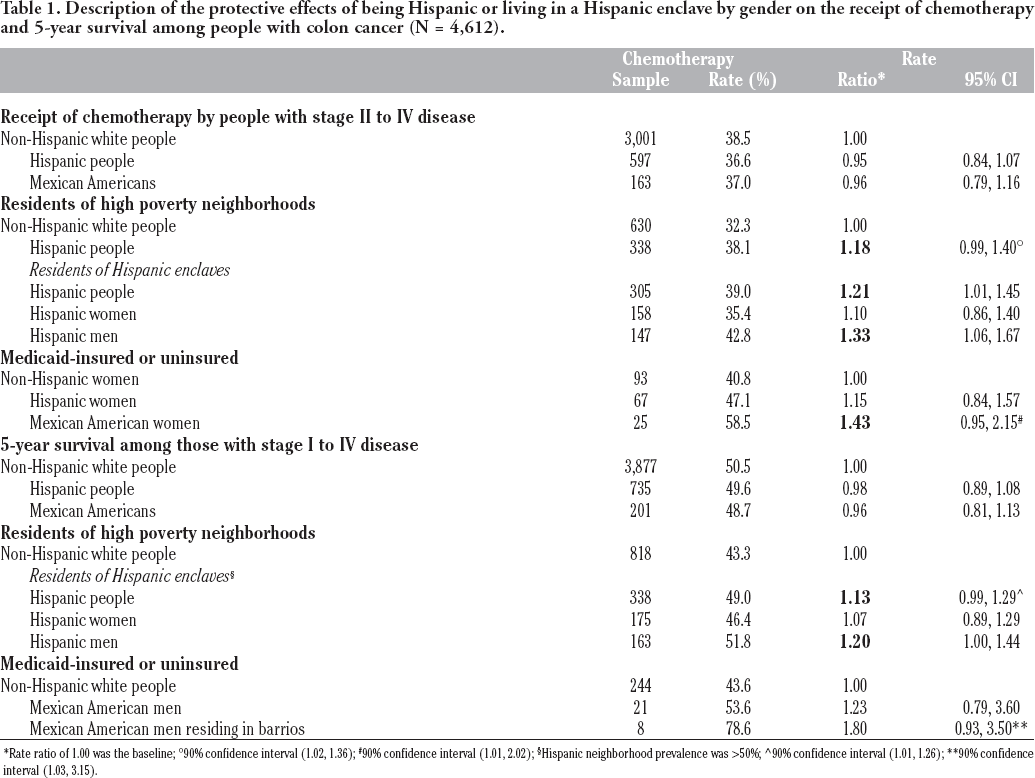
Rate ratio of 1.00 was the baseline
90% confidence interval (1.02, 1.36)
90% confidence interval (1.01, 2.02)
Hispanic neighborhood prevalence was >50%
90% confidence interval (1.01, 1.26)
90% confidence interval (1.03, 3.15).
Discussion
We tested all the main effects of being Hispanic or MA as well as all their interacting effects within Hispanic enclaves, exploring any potential gender differences as well. Most findings were null and were not presented. Even such null findings lent support to Hispanic paradox and enclave or barrio advantage theories recalling that Hispanic people and places are much more socioeconomically vulnerable than those of their NHW counterparts. Ten hypothesis tests were significant, eight in support of Hispanic advantages and two in support of NHW advantages. Additionally, all the non-significant point-estimates were in the direction of Hispanic enclave or barrio advantages. The overall pattern of findings seemed largely supportive of Hispanic paradox and Hispanic enclave or MA barrio advantage theories especially among the most socioeconomically vulnerable populations such as the poor and or the inadequately insured.
Interpretations and Future Research Direction
Consistent with a recent study of lung cancer in California, 9 our pattern of findings strongly suggested that general Hispanic enclave and specific MA barrio advantages are greater for men. Such also seems consistent with a recent systematic review of familism. 10 The concept refers to the special cultural emphases; allegiances, attachments and supports associated with nuclear and extended family networks that may attend being Hispanic, particularly a first-generation Hispanic American. We were not able to study familism, per se, with this secondary analysis, but we did uncover a potentially important descriptive addendum. Hispanic men living in Hispanic enclaves were much more likely to be married (70%) than were Hispanic women (43%) living in the same enclaves. In addition to more prevalently enjoying the support of a spouse, such men may also double their extended family network through marriage, and thereby double its protective familismbased effects. Future qualitative studies of key informing Hispanic residents who reside in Hispanic enclaves are needed to advance theory-building knowledge about the most probable explanations for the paradoxical enclave or barrio-based advantages that we and many others have observed.
Some of our analyses could be fairly categorized as powerful, especially the overall Hispanic-NHW hypothesis tests that analyzed the experiences of 3,598 to 4,612 participants. Those precise analyses probably engendered confidence. Restricting samples to the lowest socioeconomic strata and depicting interactions of ethnicity, enclave status and gender, we analyzed smaller samples. Those related to the experiences of Hispanic women and men residing in ethnic enclaves ranged from 350 to 50. Similar subsamples of MAs within key strata ranged from 200 to as small as 8. Finally, we tested multiple hypotheses, some of which only approached statistical significance, across several treatment and survival outcomes. Admittedly, these were exploratory, theory building analyses. We encourage researchers with access to national data to systematically replicate them.
Footnotes
Acknowledgements
We gratefully acknowledge the administrative and logistical assistance of Kurt Snipes, Janet Bates and Gretchen Agha of the Cancer Surveillance and Research Branch, California Department of Public Health (CDPH) and Dee West and Marta Induni of the Cancer Registry of Greater California (CRGC). We also gratefully acknowledge the research assistance of Glen Halvorson, Donald Fong and Arti Parikh-Patel of the CRGC and Madhan Balagurusamy, Daniel Edelstein and Nancy Richter of the University of Windsor. Finally, we are grateful for the assistance we received from Eric Holowaty of the University of Toronto, Caroline Hamm and Guangyong Zou of Western University and Emma Bartfay of the University of Ontario Institute of Technology in obtaining funding to create the primary database for this secondary analysis.
The collection of data was supported by the CDPH as part of the statewide cancer reporting program mandated by California Health and Safety Code Section 103885; the National Cancer Institute's Surveillance, Epidemiology and End Results Program under contracts awarded to the Cancer Prevention Institute of California, the University of Southern California and the Public Health Institute; and the Centers for Disease Control and Prevention's (CDC) National Program of Cancer Registries, under an agreement awarded to the CDPH. The ideas and opinions expressed herein are those of the authors and endorsement by the State of California, the Department of Public Health, the National Cancer Institute and the CDC or their contractors and subcontractors are not intended nor should be inferred.