
Abstract
Background and aims
Parents’ empowerment is advocated to promote and preserve an informed and autonomous decision regarding their children’ immunization. The scope of this study is to develop and evaluate the psychometric properties of an instrument to measure parents’ psychological empowerment in their children's vaccination decision and propose a context-specific definition of this construct.
Materials and methods
Grounding in previous qualitative data, we generated an initial pool of items which was later content and face validated by a panel of experts. A pretest allowed us to reduce the initial pool to 9 items. Convergent and discriminant validity measures included the General Self-Efficacy Scale, a Psychological Empowerment Scale, and the Control Preference Scale. Vaccination-related outcomes such as attitude and intention were also included.
Results
Principal Component Analysis revealed a 2-factor structure, with each factor composed of 2 items. The first factor concerns the perceived influence of one's personal and family experience with vaccination, while the second factor represents the desire not to ask other parents about their experience with vaccination and their lack of interest in other parents’ vaccination opinion.
Conclusions
In light of its association with positive immunization-related outcomes, public health efforts should be directed to reinforce parents’ empowerment.
Significance for public health
Suboptimal vaccination coverage is associated with increased risk of disease outbreak. Increasing parental acceptance of childhood vaccinations will help public health systems to reach the recommended threshold to eliminate a number of preventable diseases. This study contributes to our knowledge of the antecedents of parental immunization decision, showing that parents who excessively rely on their peers and are less self-determined have lower levels of vaccination knowledge and decreased intention to vaccinate their children. The results of this study can be used to design effective public health communication campaigns aimed at increasing vaccination acceptance.
Introduction
With the emergence of a patient-centered healthcare model, most developed countries have started to pay increasing attention to the empowerment of patients as well as parents as decisionmakers for their children's health.1,2 The principle of promoting and preserving parents’ involvement in the decisions and actions concerning their children has been applied to a number of pediatric health conditions such as prematurity, autism, obesity and disability.2-5 Interventions aimed at promoting parents’ empowerment were found to have positive effects both on parents’ psychological outcomes and on the child's health.3-5
In the past few years, parent's empowerment in the immunization context has started to receive the same attention. Within the ubiquitous and unceasing debate about the safety and efficacy of vaccinations, an ethical discourse has emerged on compulsory vaccination, calling for parents’ informed and self-determined immunization decisions. Public health authorities assume parents make an informed decision when they formally acknowledge the risks and benefits of the vaccination and its target disease(s) by signing a consent a form. The use of non-compulsory immunization is assumed to promote a self-determined parental choice. However, beyond the mere use of informed consent forms 6 and the non-compulsoriness of vaccination,7,8 it is so far unknown how parents have interpreted this call for empowerment. Furthermore, no research has been conducted so far to test whether psychological empowerment could be a predictor of parents’ vaccination-related choices. 9
Psychological empowerment
Empowerment, which is often referred to as psychological when it applies to individuals rather than groups, has become a ubiquitous word. 10 Despite being often called for in the health domain as a strategy to improve health-related outcomes, an agreed definition of empowerment is still missing as both practitioners and scholars have used it to mean different things in different settings. Rappaport defines empowerment as a process by which people, organizations and communities gain mastery over their affairs. 11 In this sense, empowerment is viewed as a process by which people increase control over their lives and health, and can be applied to individuals or communities. 10 For our purposes, it will suffice to define psychological health empowerment as the belief and claim that it is within reach of a person to contribute substantially to protect and regain his or her own health.
Psychological empowerment is not a one-dimensional concept. According to Zimmerman, empowerment is both a process and an outcome whose attributes include perceived control, perceived competence, motivation, understanding of the socio-political environment, self-esteem and proactive behaviors. 12 Another popular list of the attributes of psychological empowerment comes from the organizational literature. Grounding in the definition proposed by Conger and Kanungo first, 13 and refined by Thomas and Velthouse later, 14 Spreitzer15,16 sees psychological empowerment as a motivational construct manifested in four cognitions: meaning, competence, self-determination and impact. The scholar adds that, taken together, these characteristics represent an active orientation to a work role, meaning that the individual aspires at shaping his role and environment, and feels competent in doing it.15,16 A large literature review that investigated the effectiveness of empowerment interventions found that empowerment strategies were promising in their capability to improve health- related outcomes. 17 Another review on the effectiveness of empowerment on health and wellbeing suggested 5 key areas to group all health-related outcomes that can benefit from empowerment interventions on the basis of the available literature: 1) improved self-efficacy and self-esteem, 2) greater sense of control, 3) increased knowledge and awareness, 4) behavior change, and 5) a greater sense of community, broadened social networks and social support.10,18-21 More recently, research has called for further exploration of this construct in the context of the vaccination decision-making, based on the speculation that higher levels of empowerment, if connected with inaccurate information on the vaccination, might lead to vaccine hesitancy. 22 Previous qualitative findings indicate that, 23 when making a decision for their children's immunization, parents interpret empowerment as a set of different characteristics. Feelings of control are strictly linked to the perception of being competent and free to choose whether to be guided by trusted professionals, and autonomy can be interpreted by taking responsibility of one's decisions and having the freedom to choose whether or not to vaccinate. 22 However, no instrument is currently available to quantitatively assess whether these issues can be grouped under the same umbrella and become part of a single empowerment construct or its sub-dimensions. Furthermore, a meaningful definition of empowerment is needed in such a context. Scholars agree that it can be misleading to apply a single definition and measure of psychological empowerment to different populations and settings,24,25 as it might not appropriately reflect the uniqueness of different behavioral contexts. 26 Furthermore, the literature on psychological empowerment mostly refers to the degree individuals perceive themselves to be competent and autonomous in their actions, rather than in their decisions. 24
Aim of the study
The aim of the current study was to describe the development and evaluate the psychometric properties of a scale to measure parents’ psychological empowerment in the context of the vaccination decision for their children. Furthermore, we aimed at adjusting the original definition of this construct so that it can adequately reflect this particular decisional context on the basis of our findings. To ensure consistency with previous work we conducted on psychological empowerment in the vaccination decision,22,23,27 the present study was partly grounded in the conceptualization of psychological empowerment as a set of four sub-dimensions proposed by Spreitzer.15,16 These dimensions are (a) meaning, or the extent to which parents think that their vaccination decision is important; (b) competence, or the degree to which parents feel able to make a vaccination decision; (c) impact, or the extent to which parents perceive their vaccination decision as impactful; (d) self-determination, referring to the degree to which individuals believe that their vaccination decision is made in autonomy. In the development of the scale, we nevertheless employed other sources as well as qualitative data that we personally collected. The next paragraph will describe all the steps we took to generate and validate a Vaccination Psychological Empowerment Scale (VPES).
Materials and Methods
Item generation, content validation and item reduction
Item generation
Two researchers (MF and EG) independently generated items based on previous qualitative data collected on parental perceptions of empowerment in the MMR (Measles, Mumps, and Rubella) vaccination decision, 23 the conceptualization of psychological empowerment proposed by Spreitzer15,16 and other validated empowerment scales in the context of health. 24 We employed qualitative data because they can be a valid and enriching tool to inform the design of a survey.28,29
The items were later compared and agreement was reached between the two researchers through extensive discussion and by referring to the sources employed. During this phase, the number of items was reduced, and the items retained were changed and often relocated into a different component. Feedback was also provided on the initial item pool by a team of psychologists from the University of Erfurt, Germany, which allowed for more refinements. A 5-point scale measuring frequency and anchoring at Never and Always was chosen. The initial item pool consisted of 62 items, generated across six components: (a) self-determination (21 items), (b) perceived competence (11 items), (c) perceived impact (8 items), (d) perceived meaning (9 items), (e) information orientation (12 items), and (f) gender role preference (1 item). The initial set of items was later submitted for revision to a panel of content and face validity judges.
Content and face validation of the scale
A panel of content experts was asked to review the potential scale items and validate that they are appropriate indicators of the empowerment construct. We contacted 9 individuals based in Italy with expertise in the field of health or psychology and previous experience with survey design, and asked them to participate in this study as content validity judges. All the contacted professionals agreed to participate: four specialists in hygiene and public health, two nurses, one pediatrician, one psychiatrist, and one professor of pedagogy. We created an online survey containing the 62- item pool and sent it to them via e-mail. The survey included the division of items into components, instructions about the revision, an introduction that described the purpose of the study, and a request to provide feedback both on each single item according to clarity and appropriateness, and on the questionnaire as a whole according to completeness and accuracy. Answers were collected between August 1st and September 30th, 2015.
Ninety recommendations were provided for 47 items out of the initial 62. Recommendations involved the rewording of items to reduce ambiguity of meaning (n=54) or their deletion (n=36). The recommendations for item revision were addressed only when they were suggested by at least three jury members. Changes resulted in the rewording of 17 items and the deletion of 5. The 5 deleted items came from 5 different components, and did not eliminate the measurement of any of the scale's components. The final scale resulted in 57 items. Following the panel's suggestion, response options were changed into a 6-point Likert scale measuring agreement and anchoring at Absolutely disagree and Absolutely agree.
Descriptive assessment and item reduction
We conducted a pretest with 113 participants to allow for item reduction. The sample goal was to have at least 30 parents answering our questionnaire. This is because, according to the Central Limit Theorem, 30 observations are usually enough to observe a normal distribution for a single item. A convenience and snowball sampling was used, employing multiple social media platforms to minimize the risk of selecting parents all belonging to the same social network tribe (e.g. Facebook, WhatsApp). To be eligible, parents had to have at least one child aged up to 10 years old. We sent a link to an online questionnaire to the participants including the content validated 57-item pool and socio-demographic questions such as gender, age, education, origin, number of children and age of the youngest child. Eligibility was assessed through a screening question at the beginning of the survey.
As primary criterion for retaining items, we explored the items’ frequency of endorsement and we selected the items showing an endorsement frequency between 0.20 and 0.80. Basing on this criterion, a score from 1 to 5 was attributed to each item. Items were ordered according to their score, and those items scoring 1 or 2 were deleted (n=30). As a secondary criterion to include an item, we used the discrimination index, particularly the Corrected Itemtotal correlation index. Items with an item-total values higher than 0.3 were selected. Using these criteria, 9 items were retained for the PCA, 3 assessing self-determination, 2 assessing competence, 1 assessing impact, 1 assessing meaning, and 2 assessing information orientation (Appendix 1).
Construct validation
Participants
To assess the convergent and discriminant validity of the scale, participants were recruited through three Vaccination Centers (V Cs) in Milan. The diversity of the recruitment locations allowed for different social and cultural backgrounds to be represented in the sample. A consent form was signed by each participant prior to the administration of the questionnaire. To ensure both pro- and antivaccination parents could be represented in our sample, we adopted two recruitment strategies. Parents taking their child for the vaccination were invited to fill out a pen-and-pencil questionnaire in the VCs’ waiting room either before or after their child's vaccination. Inclusion criteria (being a mother/father and having a child younger than 6 years) were checked by the researchers. To recruit vaccination-adverse parents, the three VCs provided an anonymous list of 72 parents refusing part or all of their child's vaccinations and their telephone numbers. These parents were contacted by phone by the main researchers and asked to fill out online the same survey administered to the pro-vaccination parents. Of the 72 parents contacted, 27 never answered the phone, 15 refused to participate for either lack of time or interest in the study, and 30 accepted to fill out the survey. Of the 30 who accepted, 15 eventually filled out the survey (response rate 33%).
Materials
Participants received a demographics form, and the revised 9- item Vaccination Psychological Empowerment Scale. The scale was scored on a six-point Likert scale, with higher scores indicating higher empowerment. The scale anchors ranged from Absolutely disagree to Absolutely agree. In addition, measures of convergent and discriminant validity constructs were administered, as well as vaccination-related outcome measures.
Measures of convergent and discriminant validity constructs
Three instruments originally designed to measure specific components of psychological empowerment and unrelated constructs were used: (1) the General Self-Efficacy Scale; 30 (2) Spreitzer's Psychological Empowerment Scale adapted to the context of the vaccination decision and used in previous studies;15,16,31 (3) the Control Preference Scale adapted to the context of the vaccination decision. 32
The General Self-Efficacy Scale (GSES). The GSES consists of 10 items scored on a 4-point scale anchoring at Not at all true and Exactly true. 30 The scale is one-dimensional and was created to assess a general sense of perceived self-efficacy in order to predict coping with daily worries as well as adaptation after stressful life events. 33 The final score, ranging between 10 and 40, results from the sum of all answers’ scores.
The Psychological Empowerment Scale (PES). The original version of the four-dimensional empowerment scale in the work context developed by Spreitzer15,16 consists of 12 items scored on a 7-point Likert scale, although the version used in the current study was adapted to the context of the vaccination decision and scored on a 6- point Likert scale. 31 Spreitzer's multidimensional empowerment scale was designed to measure psychological empowerment as a motivational construct manifested in four cognitions (meaning, competence, self-determination, and impact) reflecting an active, rather than a passive, orientation to a work role and, thus, to an active decision-making process.15,16
The Control Preference Scale (CPS). The CPS consists of five cards that portray a different role in treatment decision-making using a statement and a cartoon. 32 The CPS was developed to assess the role that patients want to play in treatment decision-making, 32 ranging from the individual making the treatment decisions alone, through the individual making the decisions jointly with the physician, to the physician making the decisions alone. While the original CPS asked subjects to provide their total preference order over the five cards, the scale used in the current study was adapted to the vaccination context by replacing doctor with pediatrician and asking subjects to indicate their preferred role in their decision-making about their child's vaccination. No cartoon was provided.
Vaccination-related outcome measures
In addition to the construct validation measures listed above, we included a number of vaccination-related outcome measures to explore their association with psychological empowerment, since previous studies speculated that higher level of empowerment can lead to vaccine hesitancy.22,23,31 These include general knowledge about vaccination using the Vaccination Knowledge scale developed by Zingg and Siegrist, 34 parents’ attitude towards vaccination, their confidence in their vaccination decision, the probability they would recommend the vaccination to other parents, their intention to have their child vaccinated at the next due date, and whether the participants perceived the risks of the vaccination higher than the risks associated with it. 35 Moreover, we provided a list and asked participants whom they had talked to about vaccinations in the previous six months. The list included the following options: pediatrician, other medical professionals, homeopath, other complementary and alternative medicine (CAM) professionals, family, friends, and others. Finally, we asked participants whether they had the same opinion for all vaccinations or whether they would discriminate among them. A blank space allowed the participants to explain for which vaccination they had a different opinion.
Socio-demographic variables
In terms of socio-demographic variables, we asked participants about their gender, ZIP code, number of children, month and year of birth of the youngest child, and both parents’ year of birth, level of education and origin (Italy, EU, non-EU).
Results
Characteristics of the sample
The final sample included 231 pro- and 14 anti-vaccination parents (Table 1). Mothers’ mean age was 36.9 years (SD=5.25; range=24-49) while fathers’ mean age was 39.6 years (SD=5.8; range=25-56). Most participants were mothers (74%) and were Italian nationals (85%). More than half of the participants owned an academic degree (66%), resulting in a highly educated sample compared to the statistics for the Lombardy region. 36 In line with the statistics for the Province of Milan, about half of the participants (55%) had only one child while the other half (42%) had two or more chil- dren. 37 Mean vaccination knowledge was found to be 5.5 (SD=2.4; range=0-9). Most participants (66%) reported not to discriminate among vaccinations. Those who reported to have a different opinion for measles or MMR (n=21), all non-compulsory vaccinations (n=8; in Italy, diphtheria, tetanus, polio and hepatitis B are mandatory and currently administered as a hexavalent vaccine which also includes pertussis and haemophilus influenzae type B), chickenpox (n=7), meningitis (n=6), influenza (n=5), tetanus (n=4), hepatitis B (n=4), pneumococcal (n=3), HPV (n=2), pertussis (n=2), polio (n=2), diphtheria (n=1) and yellow fever (n=1).
Characteristics of the sample.

Factor analytic and rational item selection
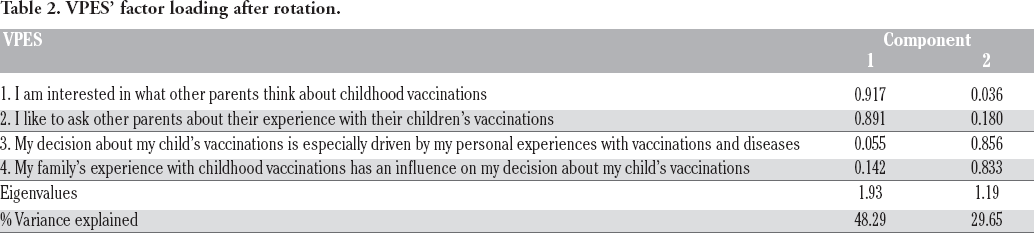
We applied principal component analysis (PCA) to analyze the latent structure of the 9-item VPES. The analysis was conducted on the 9 items with orthogonal rotation (Varimax with Kaiser Normalization). 38 The initial solution explained 55% of the variance with a 3-factor structure. The results showed that the items 1, 6, and 8 loaded on all of the three factors. For this reason, we excluded them from the analysis and the PCA was then conducted on the remaining 6 items. The new solution explained 55.5% of the variance with a 2-factor structure. The results showed that the items number 4 and 5 loaded on both factors, therefore they were excluded and the PCA was conducted again on the remaining 4 items. The new solution explained 77.9% of the variance with a 2-factor structure. The two factors had Eigenvalues over the Kaiser's criterion of 1. Results showed that the Keiser-Meyer-Olkin measure used to verify the sampling adequacy for the analysis (KMO=0.554) could be considered good.39,40 Barttlett's Test of Spherecity was statistically significant [χ2=(6)209.037; P<0.0001], indicating that correlation between the items is strong enough for PCA. Table 2 shows the factor loading after rotation. The items that cluster on the same components suggest that component 1 represents parents’ perceived influence of their personal and family experience with vaccination and that component 2 represents parents’ desire to ask other parents for their experience with vaccination and their interest in other parents’ immunization opinion. The psychometric characteristics of the VPES were investigated for each component. In terms of reliability, the VPES and its components were evaluated for internal consistency as estimated by coefficient alpha. The Cronbach's alpha of the VPES was 0.64. The Cronbach's alpha for the 2 subscales were 0.62 (perceived influence of personal and family experience) and 0.79 (desire to know peers’ opinion and experience), respectively. Since the scoring of the VPES was set on a six-point Likert scale, and the anchors adopted for score reporting are one to six, the possible total scale score range is 4-24. The descriptive statistics for the VPES as a whole and for each component are presented in Table 3. The mean interitem correlation was found to be r = 0.305.
VPES’ factor loading after rotation.
Descriptive statistics for the VPES as a whole and for each component.

Convergent and discriminant validity
The convergent and discriminant validity of the VPES was evaluated by investigating correlations with measures of related and unrelated constructs. The VPES did not correlate with the General Self-Efficacy Scale (r=0.045, P=0.485) or with the Control Preference Scale either (τ b =-0.012, P=0.825). In order to compare the VPES with a traditional definition and measurement of psychological empowerment, we computed correlations between the four components of the PES and the two factors of the VPES. We hypothesized that high scores on the first factor (EE) would indicate lower empowerment, while high scores on the second factor (EI) would indicate higher empowerment. Results confirmed our hypothesis, showing that the perceived influence of one's personal and family experience had a positive, significant correlation with self-determination (r=0.152, P=0.019) and competence (r=0.158, P=0.015). The two dimensions of competence and self-determination showed to be highly close concepts, correlating strongly and significantly (r=0.705, P=0.000). Correlations with meaning and impact were weak and almost reached statistical significance (r=0.127, P=0.05 and r=0.122, P=0.061, respectively). As we hypothesized, the empowerment component related to the desire to ask for other parents’ experience and know their opinion was negatively correlated with self-determination and the relationship almost reached statistical significance (r=-0.124, P=0.055). A negative, non-significant and weak correlation was also found with competence (r=-0.052, P=0.424). Correlations with meaning and impact were weak and non-significant (r=0.115, P=0.075 and r=0.033, P=0.617, respectively). Following these results, we decided to reverse code the empowerment component related to other parents’ experience and opinion in order to compute the final score of the VPES. Thus, the following analyses were conducted using the reverse version of this component.
Associations between the VPES and vaccination- related outcome measures
We performed non-parametric analyses since our data did not meet the assumptions of the parametric test. The VPES was found to correlate significantly and positively with parents’ vaccination opinion (r=0.323, p<9.000), confidence in the decision (r=0.266, P<0.000), intention to recommend vaccinations to other parents (r=0.152, P=0.02), intention to vaccinate (r=0.116, P=0.001), and knowledge (r=0.315, P<0.000). We computed an index to represent the number of people each participant had spoken to about vaccinations (pediatrician, CAM professionals, etc.). The VPES was significantly and negatively correlated with the number of people the participant had referred to (r=-0.176, P=0.007). We also explored whether there was a significant difference in the VPES score between participants who had spoken about the vaccination with the pediatrician in the past 6 months and those who did not. We computed an independent sample Mann Whitney U test and found that there was a significant difference (U=2945; P=0.005). Those who had not spoken to the pediatrician had a higher score on the VPES. There was a significant difference also between those who discriminate across vaccinations and those who do not as computed through the Mann Whitney U Test (U=7244, P=0.002). Those who have the same opinion for all vaccinations (M=14.69, SD=2.74) have a higher VPES compared to those who discriminate among vaccinations (M=13.42, SD=3.02).
Association between the VPES and socio-demographic variables
We did not find significant difference in the VPES score according to gender, origin and number of children. The same applies to age and level of education.
Discussion
The purpose of the current study was to develop a valid and reliable measure of psychological empowerment to be used in the context of parents’ vaccination decision, as well as to propose a context-specific definition of this construct. Contrary to the traditional conceptualization of psychological empowerment proposed by Spreitzer as a set of four sub-dimensions (perceived competence, self-determination, impact and meaning),15,16 our findings indicate that empowerment in the vaccination decision is a construct composed by two sub-dimensions, one indicating parents’ perceived influence of their own and family experience, and one indicating their desire to know other parents’ vaccination experience and opinion. The latter dimension was reverse coded, indicating higher empowerment among those parents who do not wish to know their peer's experience with vaccination and who are not interested in their immunization opinion. The first dimension, whose items were originally designed to measure the sub-dimension of self-determination, stresses the perceived influence of parents’ personal and family experience with vaccinations when it comes to make an immunization decision. In Empowerment Theory, the ability to identify the factors that influence one's decision-making is crucial to reach critical awareness, or the understanding of one's social situation. 25 The second dimension's items were originally designed to measure the sub-dimension of information orientation. Traditionally, empowerment refers to an active role orientation, the understanding of one's environment, and the strive to obtain needed resources.15,16,25 In this case, this is translated into the desire to actively ask for their peers’ opinion and their interest for their peers’ experience. The two dimensions move in opposite directions.
Concerning the first dimension, the role of one's previous experience with diseases and vaccinations on the immunization decision has been studied extensively. Freeman & Freed found that parents who vaccinated or intended to vaccinate reported past experience with a disease among family members or friends more frequently compared to non-vaccinators. 41 Furthermore, studies found that parents who had previously vaccinated their children had higher intentions to vaccinate.42,43 As for the second dimension, which stresses the importance of peers in the vaccination decision, the importance of vaccinating as a social norm has also received significant attention. Family member's belief that the child should be vaccinated predicted vaccination status, 44 while the belief that immunization is a social norm has been found to predict both intention 45 and receipt. 46
We did not find an association between the VPES and the General Self-Efficacy Scale. Our data seem to suggest that, in the context of the vaccination decision, the dimension of perceived competence does not play an important role. The final VPES measures parents’ perceived importance of their own and family experience with vaccination and their desire to know and ask for their peers’ experience and opinion on immunization, while Bandura's original concept of self-efficacy indicates people's beliefs about their ability to perform a given behavior. 47 Furthermore, the General Self-Efficacy Scale is not context-specific. This can explain the lack of correlation with the VPES, stressing the need to adapt scales to their specific context of application. The VPES did not correlate with the Control Preference Scale either. This is because the CPS aims to assess the role that parents want to play in the vaccination decision-making against that of the pediatrician. 32 The VPES does not consider the role of the pediatrician, but rather that of one's family or other parents.
We found that the personal and family experience component of the VPES had a positive correlation with two empowerment's sub-dimensions, i.e. self-determination and competence. This indicates that the more parents rely on their personal and family's experience, the more they feel able to make a sound vaccination decision and the more they feel autonomous in their decision-making. This is in line with self-determination theory (SDT), according to which perceived autonomy and competence are two strictly related concepts that contribute to fostering motivation and engagement.48,49 On the other hand, our results indicate that the desire to know peers’ opinion and experience was negatively correlated with self-determination, meaning that those who tend to look for external reassurance and confirmation among their peers will perceive themselves as less autonomous in the vaccination decision. This finding is confirmed by previous studies grounded in the SDT that found that self-determined behaviors are those that spring from the self, in opposition to those that are pressured by others. 50
Another finding is that parents consulting multiple categories of people as well as those avoiding any talk about vaccination with the pediatrician scored higher on their empowerment. In practice, this can be explained because, according to the vaccination system in the Lombardy region, parents do not necessarily have to consult a pediatrician or other medical professionals before taking their child for the vaccination, since they receive all medical forms and information leaflets at home from the local vaccination center before the appointment. From a more theoretical point of view, this confirms once again the idea that empowered decisions originate from oneself rather than following consultation with others.48,49
Regarding the relationship between empowerment and vaccination-related outcome, it appears that highly empowered parents, that is parents who base their immunization decision more on their personal experience rather than on their peers’ opinion and experience, are objectively more knowledgeable about vaccinations, more likely to vaccinate and to recommend the vaccination to other parents, more confident with their vaccination decision, and more in favor of vaccinations. The interpretation of this finding is twofold. On the one hand, this reiterates the importance of parents’ personal experience with vaccination and disease on different vaccination outcomes. As indicated above, other studies found that previous experience is a predictor of vaccination intention or behaviour. 41 On the other hand, these results shed more light on the potential perils of asking peers for their vaccination opinion and experience. Considering that previous studies found that parents are more likely to trust other parents when it comes to receive vaccination-related information 51 and that the Web is rich in anti-vaccination narratives proposed by anti-vaccination advocates,51-53 it does not surprise that lower empowerment scores are associated with negative vaccination-related outcomes.
A last finding is that having the same opinion for all vaccinations is also associated with higher empowerment. This can be explained by previous findings that self-determination predicts satisfaction with one's behavior and decisions.54-56 Thus, having a high empowerment leads to a more stable opinion about immunization, with a resulting spillover effect that invests all vaccinations.
From a theoretical point of view, our results show that decisional empowerment is different from behavioral when applied in the vaccination decision context (in our case, where parents chose for their children rather than for themselves). In this study, psychological empowerment has lost most of its traditional references to competence, impact and meaning,12,16 narrowing down to a mere matter of basing the decision on one's personal and family experience vs. the desire to know and actively ask for other parents’ opinion and experience.
Conclusions and limitations
Our study showed that the VPES is a valid and reliable instrument to measure psychological empowerment among parents who are making a vaccination decision for their children. Furthermore, the low number of items and the high explanatory power of the instrument make it a parsimonious, effective and easy administration tool.
Our results allowed for a new, context-specific conceptualization of psychological empowerment as a two-dimensional construct. Empowerment seems to be constituted by a combination of two dimensions: the tendency to base one's decision on one's own and family experience, on the one hand, and the desire to know and ask for other parents’ opinion and experience, on the other. Moreover, the two dimensions appeared to be working in opposite directions.
This study is not without limitations. First of all, our recruitment system might have led to self-selection biases in the sample, which resulted in a low number of anti-vaccination parents. Secondly, validating a scale in a different region or country might have led to different results and, thus, to a different conceptualization of the empowerment construct. Third, recruiting from local Vaccination Centers might have resulted in a sample predominantly composed by pro-vaccination parents.
While the literature on the predictors of the vaccination decision abounds, 57 parents’ empowerment in the vaccination decision as a possible driver of their immunization behavior has not catalyzed sufficient attention. Our results confirm the importance of recognizing, promoting and maintaining empowerment in the vaccination decision. In practical terms, institutions in charge of carrying out vaccination promotion activities and vaccine administration should work along two parallel lines. On the one hand, they should make sure parents always take home a positive experience with their children's vaccination, from the moment they are contacted for their first appointment (perhaps, from the moment they make the first encounter with the service during pregnancy), until when they are discarded from the vaccination center and return home. This could be done by offering continuous support, providing tailored information, and asking parents’ for feedback about their children's immunization outcome. On the other hand, institutions should pay attention to parents’ social networks, by monitoring them, presenting accurate information whenever they are needed and promoting safe information exchanges. The results of this study showed that interactions on vaccination have important implication for parents’ both empowerment and knowledge, and that parents themselves can be a primary source of information for hesitant parents.
Finally, since empowerment reflects an internal psychosocial factor, future research should employ the VPES with a larger, more representative sample by also measuring children's vaccination status, in order to understand whether the scale is able to discriminate significantly between parents who accepted, rejected or delayed their children's immunization.
Footnotes
Acknowledgments
the authors would like to thank the participants who devoted their time to participate in the study, all the members of the validation panel, and Dr. Cornelia Betsch and her team for providing constant and enriching feedback on the development of the VPES. The authors would also like to thank the Swiss National Science Foundation for funding this study as part of a larger project focused on MMR vaccination refusal (FNS_147333).
Conflict of interest: the authors declare no potential conflict of interest.
Contributions: MF, EG and PJS designed the study; LR, AZ, MF and SS contributed to the design of the study and its implementation; MF and EG collected the data and conducted all analyses; all authors participated in the drafting of the manuscript and approved this final version.