
Abstract
Native Hawaiians and Pacific Islanders (NHPIs) in aggregate experience greater health burdens than non-Hispanic Whites, such as a higher incidence of cervical cancer and COVID-19. Given the importance of vaccinations in preventing and reducing the severity of diseases, such as the flu, cervical cancer, and COVID-19, the receipt of vaccines during childhood and adolescence is crucial. Therefore, this qualitative study aimed to explore the factors associated with NHPI parents’ decisions regarding vaccinating their children with these elective vaccinations—that is, vaccinations not required for child care, preschool, or K-12 admissions in California but highly recommended. A total of 15 NHPI parents were recruited through a community-based organization. Semi-structured interviews explored parents’ reasons for accepting or denying each vaccine for their child(ren). Results demonstrated variable acceptance of each vaccine, though consistent themes included protection and concerns over side effects. This study also found two general types of parents—those who treat vaccines the same and those with varying opinions about each vaccine. Results from this study demonstrate the family- and community-oriented nature of NHPI communities, suggesting that future interventions target not only parents but also their families and communities to cultivate vaccine acceptance through social networks. Furthermore, addressing all three vaccines during well-child visits may benefit parents who view each vaccine as separate entities with individual pros and cons. Such interventions could contribute toward reducing the burdens of particularly chronic health disparities.
Keywords
Roughly, 1.7 million (0.4% of the population) Native Hawaiians and Pacific Islanders (NHPIs) alone or in combination with one or more races reside in the United States. From 2010 to 2020, the NHPI population increased from roughly 1.4 to 1.7 million people (Association of Asian Pacific Community Health Organizations, 2022). Of the approximately 19,000 NHPIs in Orange County, California, the majority are Native Hawaiians, Samoans, Chamorros, Tongans, and Marshallese (Monte & Shin, 2022; Orange County Asian and Pacific Islander Community Alliance [OCAPICA] & Asian Americans Advancing Justice [AAAJ], 2014). Despite being one of the fastest-growing populations in the United States, NHPIs continue to experience a greater burden for certain diseases than all other racial groups.
NHPIs are at higher risk for all human papillomavirus (HPV)-associated cancers, particularly cervical cancer for women and oropharyngeal cancer for men (Shing et al., 2023). Though most information about NHPIs on HPV-associated cancers is aggregated with Asians, available data exemplify disparities for NHPIs. Between 2012 and 2017, NHPIs’ cervical cancer mortality rate was 7.1 times higher than non-Hispanic Whites in California (Medina et al., 2021). Between 2013 and 2015, NHPIs (8.3 per 100,000) also had the highest mortality rate for oropharyngeal cancer compared with non-Hispanic Whites (3.4 per 100,000) and Asians (2.3 per 100,000; Gopalani et al., 2021).
For COVID-19, NHPIs have the highest cases in 15 of the 21 states that disaggregate NHPI data and the highest mortality rate in 13 of the 16 states reporting COVID-19 mortality rates (Samoa et al., 2022). In California, the crude mortality rate was higher among NHPIs (123 per 100,000) compared with the overall state (84 per 100,000) in 2020 (Ponce et al., 2021). Given that both HPV- and COVID-related diseases are vaccine-preventable, encouraging vaccine uptake is essential for reducing the severity of infection.
Immunizations can prevent many infectious and chronic diseases. According to California’s immunization requirements, the influenza, HPV, and COVID-19 vaccines are highly recommended but not mandatory for child care, preschool, and K-12 admissions (California Department of Public Health [CDPH], 2022). In 2021, the Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices recommended that children ≥ 6 months receive an annual influenza vaccine. Children ≥ 9 years, but ideally aged 11–12, should receive two doses of the HPV vaccine over 6 months or three doses for adolescents ≥ 15. Children ≥ 5 years should receive the Pfizer-BioNTech COVID-19 vaccine, with adolescents ≥ 12 years approved to receive two doses administered 3 weeks apart (Grohskopf et al., 2020; Markowitz et al., 2014; Wallace et al., 2021).
Of interest is influenza, HPV, and COVID-19 vaccine uptake among NHPIs, as such vaccines are elective (i.e., optional) and preference-sensitive. Disaggregated data on HPV vaccination rates for NHPI youth are unavailable. However, analyses of the 2014 NHPI National Health Interview Survey (NHIS) reported that 24.9% of NHPI adults aged 18–26 initiated the HPV series, and only 11.5% of NHPI adults completed the series (Gopalani et al., 2021). The rate of initiation among NHPI adults was lower than the rates reported for White (44.7%), Black (38.0%), Asian (36.3%), and Hispanic/Latinx (35.7%) women aged 19–26 in the 2015 NHIS, which excluded NHPI data (Williams et al., 2017). Though the 2014 NHPI NHIS did not include NHPIs less than 18-year old, the low initiation and completion rate in adults indicates vaccine disparities experienced among NHPIs, as well as the importance of disaggregating data from Asians. Disparities may exist due to a lack of knowledge or impeding sociocultural beliefs (Dela Cruz et al., 2017; Shing et al., 2023).
Limited data also exist for COVID-19 vaccine coverage among NHPI children and adolescents. The California COVID-19 Vaccine Progress Dashboard showed that NHPIs have higher vaccination rates than Black and Hispanic/Latinx children and adolescents. As of December 1, 2021, 3.2% NHPIs aged 5%–11% and 70.4% of NHPIs aged 12–17 completed their primary COVID-19 vaccine series (CalHHS, 2021). NHPI youth had lower vaccination proportions than Asians aged 5–11 (5.7%) and 12–17 (72.4%). In addition, NHPIs aged 5–11 had lower vaccination proportions compared with Whites aged 5–11 (5.8%) but higher vaccination proportions than Whites aged 12–17 (65.5%). Other studies, however, indicate that NHPIs have lower receipt of and less willingness to receive the COVID-19 vaccine (Asian & Pacific Islander American Health Forum [APIAHF], 2021; Ta Park et al., 2021). Lower receipt of the COVID-19 vaccine among NHPIs may be associated with higher consumption of information from unofficial sources, mistrust in health services, upstream factors (e.g., economic inequity and poor education access) that drive NHPI communities’ decisions, and inequitable allocation of COVID-19 vaccines in NHPI-dense regions (Juarez et al., 2022; Kaholokula et al., 2020; Kamaka et al., 2021; Samoa et al., 2022).
On a positive note, the CDC’s 2014 Vital and Health Statistics documented influenza vaccination rates for NHPI children 6 months–17 years (58.1%) to be higher among all children in the United States (49.9%; Zelaya et al., 2017). Unlike the HPV and COVID-19 vaccines, influenza vaccination rates for NHPI children and adolescents were similar to Asian children and adolescents (58.2%; Zelaya et al., 2017). Though disparities in influenza hospitalizations and deaths have not been reported among NHPIs, continual promotion and encouragement of the influenza vaccine will protect the health and wellbeing of their communities.
Given the importance of vaccinating children to prevent infection and transmission of influenza, HPV, and COVID-19, this study explored the reasons for and against these elective and preference-sensitive vaccinations among NHPI parents in Orange County, California. Parents’ acceptance is important for increasing vaccine uptake. Thus, we hope findings from this study can inform future research and interventions to increase vaccination and eventual disease prevention in this important priority population.
Methods
In fall 2021, we undertook a qualitative cross-sectional study of NHPI parents to better understand the reasons for vaccinating their children. This study was conducted in collaboration between researchers from an academic university (the University of California, Irvine) and leaders from an NHPI community-based organization (the Pacific Islander Health Partnership [PIHP]). The study was informed by the Theory of Planned Behavior (TPB), previously used to explore factors associated with vaccine acceptability (Askelson et al., 2010; Fernandez-Pineda et al., 2020; Li et al., 2021). The TPB assumes that health decisions are made based on attitudes (negative or positive), subjective norms (the expectations, approval, or opinions of others), and perceived behavioral control (the belief that the person can implement the behavior; Fishbein & Ajzen, 2009). Our focus was specifically on vaccination behavior; thus, we also consulted literature on vaccine hesitancy. Vaccine-hesitant individuals hold varying degrees of indecision about vaccines (Kestenbaum & Feemster, 2015). Factors that influence parents’ positions along the vaccine hesitancy continuum include their attitudes and knowledge, expectations from their social networks, doctor’s recommendations, sociocultural considerations, or social media (Askelson et al., 2010; Chung et al., 2017; Dela Cruz et al., 2017; Kestenbaum & Feemster, 2015; McElfish et al., 2021; Walker et al., 2021; Wilson et al., 2018).
Data Collection Instruments
A preinterview survey contained demographic questions, including age, gender, NHPI ethnicity, highest level of educational attainment, marital status, and age and gender of each child (derived from the PhenX Toolkit). The survey also included health care and vaccination questions, including whether their child/children had a regular doctor and the vaccination status of each child for flu, HPV, and COVID-19. Parents were also asked to indicate if they were ever hesitant about influenza, HPV, and COVID-19 vaccines.
The TPB guided the development of the semi-structured interview guide (Ajzen, 1991; Fernandez-Pineda et al., 2020). Open-ended questions were developed based on the five constructs of the TPB—actual behavior, attitudes, perceived subjective norms, perceived behavioral control, and intentions. A sample of questions included: (1) Why did you vaccinate your child/children? (2) What are your concerns, beliefs, and feelings about the vaccine? (3) What do you think people most important to you would think about you vaccinating your child/children? (4) What factors promote or hinder your initiation to vaccinate your child? and (5) If your child/children are not vaccinated, do you intend to? This framework was used to gauge parents’ decision-making factors. Questions were repeated per vaccine to allow for an in-depth discussion of each vaccine.
Discussions were also tailored depending on participants’ responses to the preinterview survey. If a participant indicated hesitancy or did not vaccinate their child for certain vaccines, the interview guide would include additional probing questions to explore these decisions.
Participant Recruitment and Data Collection
Four community liaisons from PIHP recruited participants based upon the following criteria: identified as Native Hawaiian or Pacific Islander, have at least one child under 18, reside in Orange County, CA, and are English-speaking. Once a participant was recruited, the liaison scheduled an interview on Zoom and sent each participant a Qualtrics preinterview survey link. This community-assisted recruitment ensured the anonymity of the participants’ identities, which the university’s Institutional Review Board (IRB) approved as exempt research. Sample size was determined based on projected data saturation (consistent themes and no novel themes after five consecutive interviews; Guest et al., 2020). All participants received a U.S.$50 Amazon or Walmart gift card.
The primary author held semi-structured, one-on-one key informant interviews on Zoom in early 2022, each lasting 30–60 minutes. Participants’ screen names were changed to assigned pseudonyms. Interviews were audio-recorded only; participants provided verbal consent. All interviews were transcribed for analyses.
Data Analysis
The primary author conducted all coding using Dedoose 9.0.46 to organize and code the qualitative data. An abductive approach was chosen because it allowed the researcher to establish preidentified codes while being receptive to new codes and themes (Timmermans & Tavory, 2012). Preidentified codes were based on factors influencing acceptance and hesitancy discussed in the existing literature. The TPB constructs were an initial guide rather than a directed content analysis. The first round of coding included reviewing and coding each transcript line-by-line. This allowed for the conception of emerging themes or sub-codes and consideration for saturation. The second coding round ensured coding consistency while generating categories and themes. Reclassification of coded data occurred upon consultation with all authors. The final set of codes informed the development of this paper. Research findings were reviewed by our collaborating community leaders for feedback and expert validation.
Results
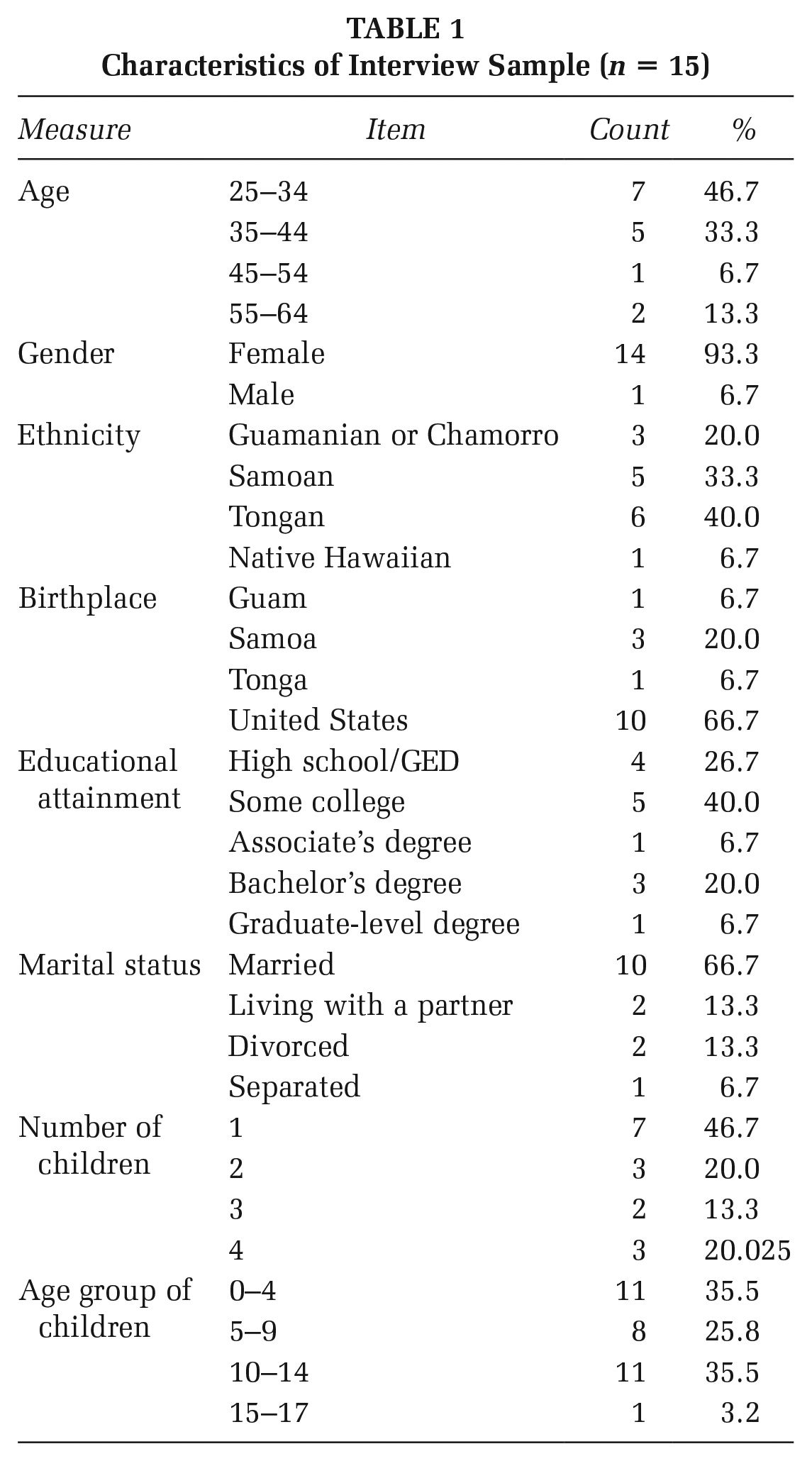
A total of 15 parents were interviewed; all but one were female. The majority identified as Tongan (n = 6) or Samoan (n = 5) and were born in the United States (n = 10). Most parents’ highest educational attainment was high school (n = 4) or some college (n = 5). The majority of parents were 25–34 (n = 7) or 35–44 (n = 5) years old. In addition, most parents have one child (n = 7), and the majority of participants’ children were aged 0–4 or 10–14 (see Table 1).
Characteristics of Interview Sample (n = 15)
Most participants indicated that their children have a primary provider or pediatrician (n = 13). In addition, most parents reported hesitance for the HPV (n = 10) and COVID-19 (n = 11) vaccines, unlike the influenza (n = 6) vaccine. The majority of age-eligible children received the flu and HPV vaccines, whereas most age-eligible children did not receive the COVID-19 vaccine (see Table 2).
Health Care and Vaccination (n = 15)
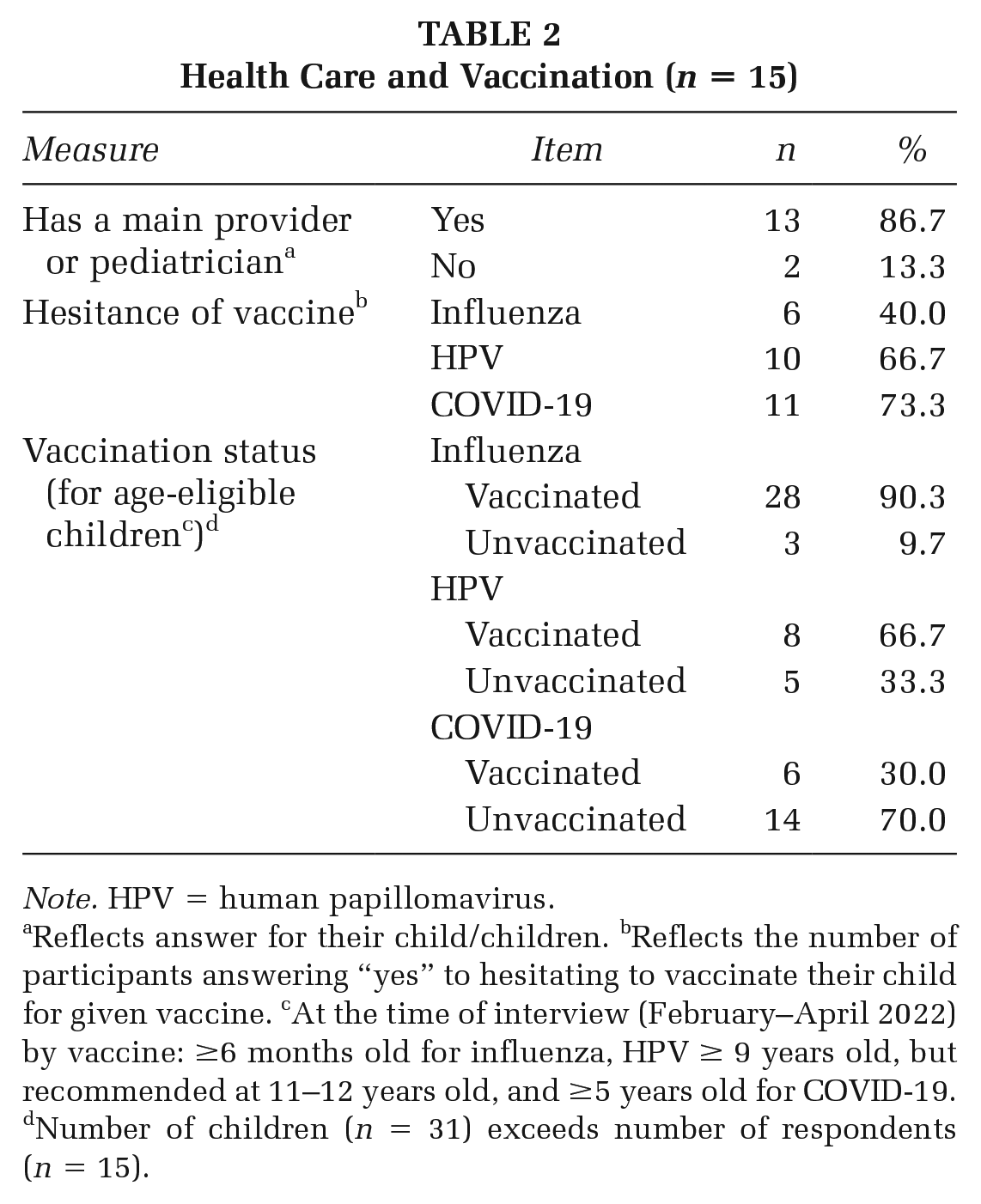
Note. HPV = human papillomavirus.
Reflects answer for their child/children. bReflects the number of participants answering “yes” to hesitating to vaccinate their child for given vaccine. cAt the time of interview (February–April 2022) by vaccine: ≥6 months old for influenza, HPV ≥ 9 years old, but recommended at 11–12 years old, and ≥5 years old for COVID-19. dNumber of children (n = 31) exceeds number of respondents (n = 15).
Themes Regarding Parental Vaccine Decision-Making
As shown in Table 3, consistent and different themes emerged specific to each vaccine; we discuss these themes briefly in the following sections.
Themes Influencing Parental Decision-Making, by Vaccine
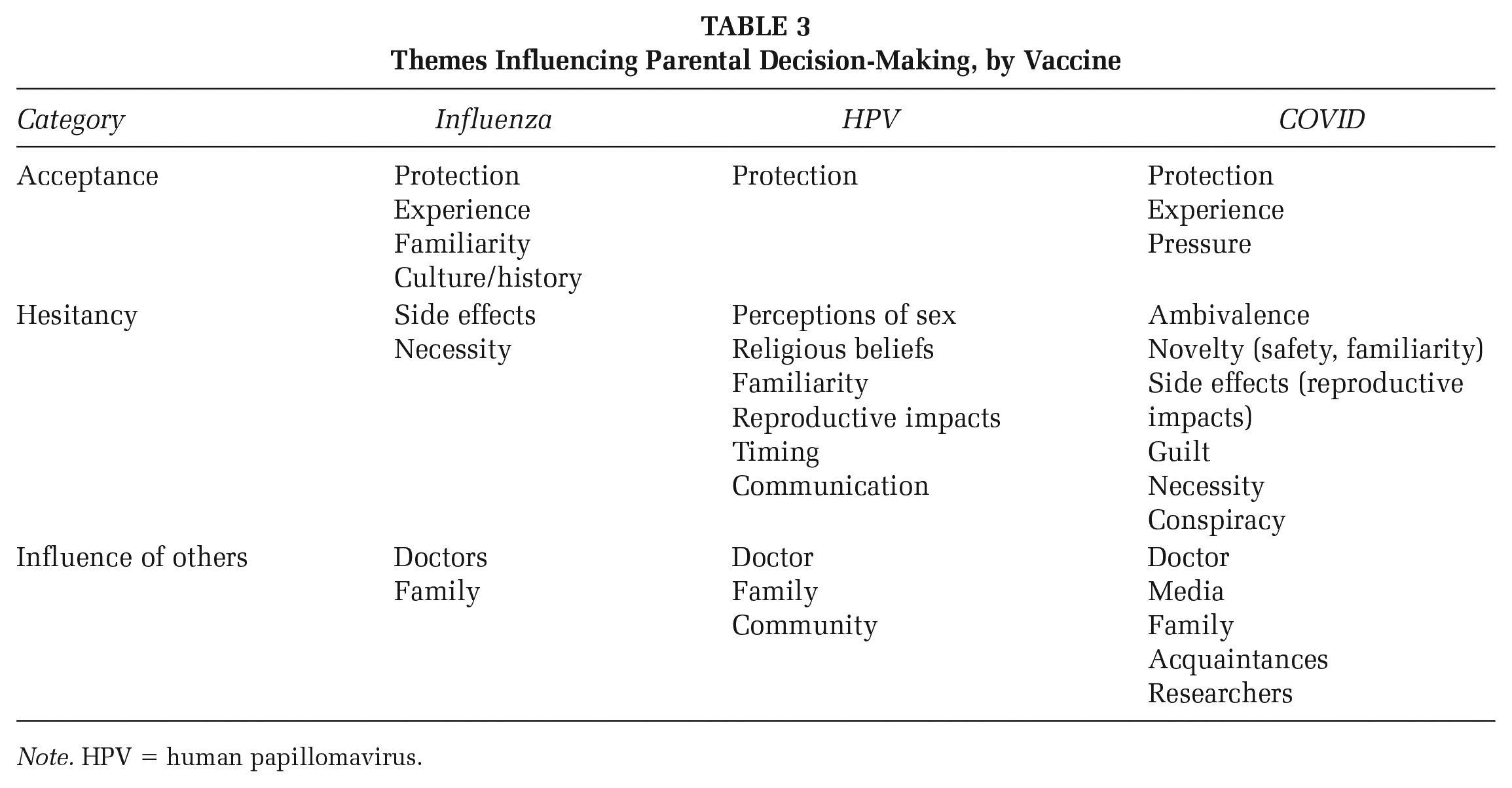
Note. HPV = human papillomavirus.
Influenza
All parents who vaccinated their children against the flu vaccine stated that the primary reason for acceptance was to protect their children and others. Ten parents indicated that their familiarity and positive experiences with the flu vaccine were reasons they were comfortable vaccinating their children against the flu annually. Two participants shared that the flu epidemic in the Pacific Islands heightened the preciousness of life, and the flu vaccine was one way to preserve this. One Samoan mother whose two children are vaccinated against the flu explained, “The big flu epidemic back in the Islands . . . wiped out almost a whole generation of people . . . As far as the benefit of having a [flu] vaccine, yes [there is].”
Nearly, all (n = 13) parents indicated that their doctors played a role in their decision-making. Some might not have vaccinated their children if their doctor did not recommend it. Older families positively influenced decision-making for four parents.
Though most parents accepted the flu vaccine, some indicated they were initially hesitant. These parents were concerned about the side effects or believed the vaccine was unnecessary. One Tongan mother whose three children are not vaccinated against the flu stated, “I believe that all kids get sick with the flu yearly. The reason why I do not have my kids get the flu shot is because they’re going to get sick.” Two parents felt their children’s bodies could naturally fight the illness.
HPV Vaccine
All but one parent discussed their belief that the HPV vaccine was for their children’s protection, particularly cancer prevention. One mother was a cancer survivor, while another parent discussed how cancer was prevalent in their family. Another parent expressed pressure from their cultural community that strongly believes a parent’s role is to protect their child with any opportunity, including the HPV vaccine.
All participants mentioned sex perceptions and the HPV vaccine. Nine acknowledged that discussing sex-related topics, such as the HPV vaccine, is taboo in NHPI cultures; however, such sex taboos did not influence their decisions. For six parents, perceptions about sex played a role in their hesitancies or refusal of the HPV vaccine. One parent expressed that their child was too young to consider a vaccine correlated with sexually transmitted infections (STIs). Another parent discussed how their religion teaches sexual abstinence, which is one reason for denying the vaccine.
Ten parents stated their unfamiliarity with the HPV vaccine as a reason for hesitancy. Two parents’ unfamiliarity was because they did not receive the vaccine as adolescents. A Chamorro mother, initially hesitant toward the HPV vaccine but proceeded to vaccinate her 16-year-old son, shared, “I don’t think I ever got that. So, this is me being, ‘Well, I never got that; I turned out fine.’ I think that was my only hesitation was like, ‘Why do they need it now?’” Three parents also expressed concerns about how the vaccine would impact their child’s reproductive health.
As with the flu vaccine, medical professionals’ recommendations played important roles in the overwhelming majority of parents’ HPV vaccination decisions. In the words of one Samoan parent who was also hesitant about the HPV vaccine but decided to vaccinate her 13-year-old son: “I did it because the doctor said that’s what he needed at that age, not because I knew what she was talking about, [and] not because I was very much educated on it.” The profession, however, did not have to be a doctor. One Chamorro mother with a vaccinated 12-year-old daughter implied this by stating, I think the doctor was just more matter-of-fact, like almost a numbness to it because it’s like desensitized. But with my cousin [an RN], it was more comfortable just because she knows my daughter, she knows how I think, and so it just made it more easier to talk about with her.
COVID-19
As with the flu and HPV vaccines, the majority (n = 11) of parents stated that protection was the primary reason to vaccinate their children against COVID-19. Though some parents were initially hesitant, they were later acceptant due to the protective measures of the vaccine. One Samoan mother who, along with her husband, had COVID-19 stated that they vaccinated their children because “We just don’t want them to go through what we went through.”
Parental attitudes toward COVID-19 varied widely, unlike the previous two vaccines. Many parents felt ambivalent about the COVID-19 vaccine, pondering whether the pros outweighed the cons. For instance, two parents cited the lack of data on NHPIs. In the words of one Native Hawaiian mother with a vaccinated 12-year-old daughter, “I did have a little bit of hesitancy because I really couldn’t see anything positive. They certainly didn’t do any of those children studies on Native Hawaiian and Pacific Islanders.” Some parents also felt the vaccine was pushed out too quickly for children and wanted more time for investigation of the vaccine’s long-term effects, such as on their reproductive health. As explained by one Chamorro mother whose 12-year-old daughter is vaccinated against the flu and HPV but not COVID-19, We are a huge family. I hope my daughter can have that for herself, but I think that’s one thing that comes into my mind, “What if we get her vaccinated, and then there’s something wrong with her being able to have her own family one day?”
Indeed, six parents conveyed that although they were vaccinated, they were or would be hesitant to vaccinate their children because their bodies may not tolerate the vaccines as well as adults. Others expressed guilt should the vaccine negatively impact their child’s health, such as harming their reproductive capabilities. Finally, some parents felt that the COVID-19 vaccine was unnecessary, as explained by one Samoan mother with an unvaccinated 5-year-old son and unvaccinated 8-year-old daughter: Both my husband and I caught it [COVID-19]. And, even one of my kids caught it, and he’s five, but he had absolutely no symptoms. . . As adults, we had symptoms . . .If it’s not targeting the kids as much as the adults, then I feel like they shouldn’t really get it [the COVID-19 vaccine].
One parent felt that COVID-19 was a government control factor and that the COVID-19 vaccine was unnecessary.
Finally, the influence of others was important but also varied. Due to the relative recency of COVID-19, many (n = 12) parents stated that the media played a role in their attitudes. Media had a negative influence if parents heard or saw the vaccine’s adverse effects. Media outlets primarily highlighting professional opinions from doctors and scientists had a positive influence. Eight parents said their acquaintances, including friends and co-workers, influenced their opinions on the COVID-19 vaccine negatively and positively. Nine parents indicated that their family influenced their opinions of the COVID-19 vaccine; generally, family members played a more positive role. For instance, one Samoan mother whose 10- and 11-year-old sons are vaccinated against COVID-19 shared, “I was waiting to see if they [nieces and nephews] happen to have any side effects. But yeah, none of them [did], so that kind of made my decision for giving them the vaccine.”
Two parents felt socially pressured to vaccinate their children. One parent indicated that other people made them feel negligent for not vaccinating their children, while the other felt that getting the vaccine would help her daughter “socially fit in.” Finally, for six parents, doctors’ professional opinions presented in the news articles or media played a role in easing parents’ concerns. One mother whose daughter is a cancer survivor stated that their oncologist did not promote the urgency of the COVID-19 vaccine, unlike the flu vaccine.
Consistency in Parental Decisions Across Vaccines
Overall the key informants tended to fall into one of two groups: those who treated all vaccines the same and those for whom vaccination depended greatly on the type. Parents who believed all vaccines are the same generally viewed them as protective measures. One Samoan mother who vaccinated their child with all three vaccines described this from a culturally significant standpoint: Diseases that were brought over [to the Pacific Islands] by other non-natives had wiped out generations of people . . . [This] could have been combated by vaccines . . . History, institutions, social pressure of peers and families, and older generations encourage our children to be vaccinated.
More parents, however, were less consistent in how they viewed vaccines. One Tongan mother stated, “I believe in vaccinations, so my kids are vaccinated with the shots that they get when they’re born.” However, this mother also discussed how she chose not to vaccinate her children against influenza and COVID-19, primarily because she felt them unnecessary. Generally, parents (regardless of their children’s ages) with differing opinions of the vaccines had more favorable attitudes toward influenza and HPV vaccines. Many parents who were hesitant or unaccepting of the COVID-19 vaccine conveyed openness to future acceptance with more research on its impact on children’s health.
Discussion
To our knowledge, this is the first study that explores NHPI parents’ decision-making toward elective child and adolescent vaccinations. Protection of children from sickness emerged as a common theme across all vaccines, similar to past research that suggests parents generally associate vaccines with protection and prevention (Hopfer et al., 2022; Painter et al., 2019; Xiong et al., 2021).
We found the TPB construct of attitudes to be an important factor in parental decision-making for all three vaccines. Similar to prior studies, parents’ attitudes often indicated their acceptance of the vaccines (Li et al., 2021; Painter et al., 2019). However, attitudes did not always reflect actual behavior or intention, especially if parents had unresolved reluctance. Unlike the influenza vaccine, approval of the HPV and COVID-19 vaccines did not necessarily indicate parents’ acceptance of the vaccine, with novelty influencing reluctance. This is similar to findings where parents’ positive outlook on the COVID-19 vaccine did not always lead to vaccine acceptance (Hopfer et al., 2022). Parents’ attitudes are dynamic. Their judgment of vaccines, particularly the COVID-19 vaccine, is subject to change due to new research that could increase acceptance or lead to vaccine hesitancy.
Parents’ attitudes toward the vaccine may also arise from cultural beliefs. This was evident with parents’ concerns about the impact of vaccines on their children’s reproductive health. Similar to a study conducted among Hmong-American parents’ perceptions of the HPV vaccine, NHPI parents expressed hesitancy about the HPV vaccine’s impact on their children’s reproductive capabilities (Xiong et al., 2021). Prior studies have also shown parents’ concerns about the side effects of the COVID-19 vaccine (Hopfer et al., 2022; Middleman et al., 2022). However, none have mentioned concerns over reproductive capabilities. Like the HPV vaccine, parents were concerned about how the COVID-19 vaccine would impact their child’s reproductive capabilities, especially if they heard stories of the vaccine’s side effects on women’s menstrual cycles and reproductive organs. Parents’ concerns for their children’s reproductive capabilities may extend from “family” being a core value in NHPI cultures, where aiga/’ohana (“family,” including community, in Samoan and Hawaiian) serves to preserve cultural values and practices intergenerationally (Godinet et al., 2019). Future studies may further explore the role of aiga/’ohana in decision-making.
Another finding that warrants more research is the change in sex perceptions toward the HPV vaccine. Contrary to prior studies exemplifying a negative association between the HPV vaccine and sexual promiscuity (Fernandez-Pineda et al., 2020; Lee et al., 2018; Lin et al., 2021), most NHPI parents did not express fears about the vaccine leading to increased sexual activity. Instead, parents expressed having open conversations about sex, considering the younger generation’s sex culture. Some parents accepted the vaccine as a precautionary measure, suggesting that the HPV vaccine is not an initiator of sexual activity (Krawczyk et al., 2015). Parents’ willingness to vaccinate their children was similar to the protective measures against the flu and COVID-19 but in the context of cancer prevention. These findings suggest that NHPI parents may be primed for future interventions.
For many parents, subjective norms also influence attitudes (Li et al., 2021). With an overwhelming amount of anti-vaccine rhetoric on the internet, parents turned to their families, acquaintances, and community to resolve or reaffirm the information gathered from the media. Parents felt at ease if other parents did not vaccinate their children for similar reasons, likely due to conformity to peer groups. However, parents took a “wait-and-see” approach with their family, where observing their nieces and nephews allowed parents to assess the vaccine’s efficacy (Wang et al., 2014). Parents were more acceptant of vaccines if knowledge was acquired from a trusted source, especially health care providers (Chung et al., 2017). Parents’ social networks, particularly within their family or community, may have played an important role in decision-making, given the value of aiga/’ohana in NHPI cultures (Godinet et al., 2019; Kaholokula et al., 2018).
Despite our novel findings, the study design had several limitations. First, convenience sampling relied on community leader recruitment, which may have biased the sample toward those with higher knowledge due to their previous interaction with PIHP. Second, many parents had children who were not age-eligible for certain vaccines, leading them to discuss their beliefs and intentions in more hypothetical rather than real terms. Another limitation was that coding was conducted by one investigator only. This limitation was necessitated by the time of the study, which occurred in early 2022. At this time, university instruction was remote, and research guidelines limited face-to-face interactions. This presented considerable challenges to the recruitment and training of additional student coders. In addition, we have found that there are many challenges to cloud-based collaboration in coding due to the limitations of qualitative software programs themselves, often necessitating the involvement of a qualitative data manager (a position we did not have during COVID lockdowns) to ensure multiple subfiles are always bundled together. To adapt to these challenges, we turned to our collaborating community leaders for expert consensual validation of research findings. Receiving their confirmations increased our confidence that findings are credible and reflect NHPI community perspectives (Brink, 1993; Bruce, 2008; Sandelowski, 1998). Our departure from traditional coding processes may suggest the necessary step of incorporating community opinions during qualitative data analyses to determine the validity and relevance of research findings.
Implications For Practice
Despite the limitations, we hope this study provides valuable insights that inform future work for vaccination interventions with NHPI communities. Our findings suggest that education targeting parents should highlight the benefits of each vaccine in protecting their children’s health. Since parents may not have excessive time to research each vaccine in detail, resources should summarize current research for easier and more convenient access. NHPIs are also family- and community-oriented. Thus, educational methods should target children, adolescents, parents, family members, and community leaders to cultivate support through social networks. Future research and resources should also be culturally appropriate, addressing cultural concerns, such as the impact of vaccines on reproduction. Finally, in line with the American Academy of Pediatrics’ recommendations, medical providers should be educated to strongly recommend all three vaccinations at every well-child visit. More universal vaccinations for NHPIs could significantly reduce their health disparities in the future.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399231193707 – Supplemental material for Decision-Making Regarding Elective Child and Adolescent Vaccinations Among Native Hawaiian and Pacific Islander Parents in Orange County
Supplemental material, sj-docx-1-hpp-10.1177_15248399231193707 for Decision-Making Regarding Elective Child and Adolescent Vaccinations Among Native Hawaiian and Pacific Islander Parents in Orange County by Cynthia L. Fok, Melenaite Fifita and Sora Park Tanjasiri in Health Promotion Practice
Footnotes
Authors’ Note:
We would like to thank the community members who participated in the interviews, the University of California, Irvine Program in Public Health, Stanford Center for Asian Health Research and Education, and the Pacific Islander Health Partnership. This study was funded by the University of California, Irvine’s Undergraduate Research Opportunities Program, and Stanford University’s Center for Asian Health Research and Education.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.