
Abstract
Background
In neonatal intensive care units (NICUs) health care professionals typically give most of their attention to the infants and the mothers while many fathers feel uncertain and have an unmet need for support and guidance. This paper describes and discusses participatory action research (PAR) as a method to improve NICUs’ service for fathers. Our goal is to develop a father-friendly NICU where both the needs of fathers and mothers are met using an approach based on PAR that involves fathers, mothers, interdisciplinary healthcare professionals, and managers.
Design and methods
This PAR process was carried out from August 2011 to July 2013 and included participant observations, semi-structured interviews, multi sequential interviews, workshops, focus groups, group discussion, and a seminar. The theoretical framework of validity described by Herr and Anderson's three criteria; process-, democratic-, and catalytic validity were used to discuss this PAR.
Results
Twelve fathers, 11 mothers, 48 health professionals and managers participated in the PAR process. The collaboration ensured the engagement for viable and constructive local changes to be used in designing the concept of the father friendly NICU.
Conclusions
This paper contributed new knowledge of how PAR can be used to ensure that participants engaged in the field are involved in the entire process; consequently, this will ensure that the changes are feasible and sustainable.
Significance for public health
This case study contributed insight into the role and importance of participatory action research (PAR) in clinical practice. By engaging the stakeholders in the process, the culture of the neonatal intensive care unit became open to reflection and action. It was very important to understand the purpose and context of the activities and to use them accordingly to the participants. By using the right activities in the right context, we gained an opportunity to promote participants’ creativity. This required the researchers to be flexible and to be aware of PAR as a time-consuming approach.
Introduction
An early parent-child relationship is important for a child's development, both intellectually and socially. 1 The admission of premature or ill newborns to neonatal intensive care units (NICUs) may make the establishment of the parent-child relationship challenging due to parents’ anxiety, despair, medical circumstances, and the NICUs’ physical environment. 1
Healthcare professionals typically provide most of their attention to the infants and their mothers, while overlooking the fathers’ desires to be equal partners in childcare. 2 Fathers often feel uncertain and find it difficult to establish an optimal father-child relationship. They often experience fear, anger, and guilt. They have a high self-reported stress-level, which is maintained during the entire hospital experience.3,4 Moreover, parents of infants admitted to an NICU have an elevated stress level that has been shown in a systematic review. 1 Various interventions (e.g. individual support, education, and communication programs) have intended to reduce parental stress and have been evaluated;5-12 however, the results have been mixed. 13
According to some researchers, fathers require interventions that differ from those of mothers.9,11 Several descriptive studies have explored fathers’ needs and experiences during the admission of their infants to an NICU.1,3,4,14-22 However, no intervention studies addressing these needs could be identified.
This paper describes and discusses participatory action research (PAR) as a method to improve NICUs’ service for fathers. Our goal is to develop a father-friendly NICU where both the needs of fathers and mothers are met using an approach based on PAR that involves fathers, mothers, interdisciplinary healthcare professionals, and managers.23,24
Design and Methods
To produce practical knowledge that is useful to parents and NICU staff, we initiated PAR, which was inspired by Reason and Bradbury and Herr and Anderson23,24 PAR is defined as: A participatory process concerned with developing practical knowing in the pursuit of worthwhile human purposes. It seeks to bring together action and reflection, theory and practice, in participation with others, in the pursuit of practical solutions to issues of pressing concern to people, and more generally the flourishing of individual persons and their communities(23) p 4.
This process was conducted through systematic cycles of actions and reflections. In action stages, the stakeholders provided knowledge through various activities; in reflection stages, the lived experiences were understood by conversations with the stakeholders. As we deepened our understanding of the topic, future plans were devised.23,25 The PAR process was conducted from August 2011 to July 2013.
Setting
The study was conducted at a 22-bed level II NICU at a regional hospital in Southern Denmark, with approximately 600 admissions per year. 26 The unit was organized into two subunits with thirty-eight nurses, two assistant nurses, and four medical doctors.
Most infants were admitted directly from the maternity ward. The unit was a centre for the treatment of premature infants who were born from a gestation age of ≥28 weeks. Double and quad occupancy rooms were provided for the families. The presence of parents and siblings was unrestricted. The families had an armchair placed next to the infants’ incubators or cradles and the parents could sleep in a patient hotel adjacent to the NICU. Only one of the parents could stay without paying; the second parent was charged. However, during long-term hospitalization, both parents stayed with their newborns in an NICU family room without payment during the last week of hospitalization.
The research team and participants
The first author, BN, was the primary investigator of this research team. As an employee of the Paediatric Centre, she was an insider; however, she had no clinical experience in the NICU. Therefore, her position was changed to an outsider within. 24 Two co-researchers’ positions were insiders as they both worked at the Paediatric Centre and the final two had the position as outsiders since they had no relation to the participants and the setting under study. 24 Two co-researchers, a Masters student in educational anthropology and a service designer were invited to be a part of the research team for August 2011 – January 2012. Both co-researchers were outsiders in relation to participants and the NICU. This insider/outsider research team collaborated with the stakeholders. The key stakeholders were fathers and mothers, whose infants were admitted to the NICU, as well as nursing staff, doctors, and managers who worked in the NICU. 23
Methods
The exact type and number of activities were not decided a priori; rather, they were decided during the process in order to engage relevant stakeholders in an appropriate and meaningful way.23,25 The activities and those involved are illustrated in Figure 1. The actions and reflections were guided by the wish to generate i) knowledge of the everyday lives of and the attitude towards fathers in the unit; ii) detailed knowledge of the fathers’ experiences, needs, and wishes; iii) new ideas and inspiration; and iv) actions towards a father-friendly NICU. Initially, participant observation provided preliminary knowledge of the fathers’ needs and the NICUs’ culture. The participant observation implies proximity to the stakeholders and the starting point to ground the PAR approach in the perspective and interests of those immediately concerned.23,27-29 The purpose of the participant observation was to obtain knowledge of i) the fathers’ and mothers’ presence and actions in the everyday life in the NICU and ii) the staff's daily activities, how they supported the fathers, and how they cared for children and their families.

The activities and the researchers involved in the PAR process. Primary investigator (BN) was in charge of the activities which are marked with blue colours, the master student in the green activities and the service designer in red activities.
The delivery of a premature or an ill newborn was not what the parents had wished or expected. To gain detailed knowledge and understanding of the fathers’ thoughts and expectations at the admission to the NICU, fathers were invited to partake in a semi-structured interview. 30 We wished to provide views on the fathers’ personal story and reflections. As it can be difficult for fathers to share their emotional experiences in a group session, we planned to conduct semi-structured interviews. 31
To explore whether fathers’ needs changed during the hospitalization, we planned multiple-sequential interviews with fathers and mothers. 32 Multi-sequential interviews follow the persons’ daily life and provides the researcher the opportunity to hear about the experiences first-hand, rather than retrospective. 32 In these interviews, we explored the preliminary knowledge obtained from participant observation and the semi-structured interviews. The purpose was to obtain a broader and more detailed account of i) the fathers’ experiences and needs and ii) mothers’ experiences and how they reflected the fathers’ role. The knowledge from the individual activities were included in the group activities, workshops, and focus groups.
To get a broader understanding of the nursing staff's general view of the fathers and their challenges in caring for and cooperating with the fathers, we conducted two focus groups with nurses. 33 In contrast to individual semi-structured interviews, the interaction between the participants in the focus group is an essential source of data. The interaction yielded data on social groups’ interpretations, interactions, and norms, which is of importance to the participants, and the groups agreements and nuances. 33 We were inspired by participatory design methods, 34 and workshops were planned with fathers, mothers, and interdisciplinary staff. The purpose was from a new point of view to share current experiences to deepen our understanding and to prime for and generate ideas for a future, father-friendly NICU.
The workshop was a group activity where the participants were involved in different activities (e.g. making, telling, or enacting). These activities could be performed either individually or collectively. The goals include i) probing, ii) priming, iii) gaining a better understanding, and iv) generating ideas. 34 Using PAR, knowledge obtained from participant observation, semi-structured interviews, multi sequential interviews, focus groups, and visits to other NICUs was used to plan the workshop.
The research team's reflections and analysis of the data obtained from the different activities provided ideas for the concept of a father-friendly NICU. We wanted to check if other fathers could confirm the reflection and plan a group discussion. A group discussion is a focus group where the participants are stimulated to discuss, reflect on, and to confirm the researchers’ preliminary analysis and knowledge.25,33,35
As changes in clinical practice might only be implemented if changes make sense to the staff,23,24 the research team decided to invite all the NICU's nursing staff, doctors, and managers to a one-day seminar. The purpose was to share current experiences and cooperate in developing a father-friendly NICU.
The development of a father-friendly NICU was expected to be a complex intervention as it consisted of various activities, included individual needs and wishes, and engaged several staff members in the final provision at the department. 36 Therefore, the research team chose various methods in the implementation process: staff meetings, clinical practice tests, focus groups, and supervision.
The specific activities in the father-friendly NICU were examined to be able to adjust the concept as needed and so the initiatives made sense for the participants and they could be handled in practice. Furthermore, staff meetings were conducted with an agenda: positive changes to meet fathers’ needs. All staff had the opportunity to be involved, informed, and have ownership to ensure that the concept would be feasible and sustainable.
To understand the nursing staff's self-efficacy concerning supporting the fathers as recommended in the concept of the father-friendly NICU, three focus groups were established. Each group met three times throughout the project to discuss øøtheir experiences of the different concept initiatives.
Analysis
The analytical approach followed the principles of Grounded Theory, as defined by Charmaz. 32 In this approach, it was important to follow participants’ understanding of the matter as well as to investigate what concerns participants may have. In the first step, the field notes, transcriptions, and summaries were repeatedly read to enable familiarity with the text. The next step was initial open coding, which was performed to reveal the informants’ views (i.e what is happening). Then, focused coding, within and across the different datasets, was performed to enable categorization of the initial codes into more abstract, general, and analytically inclusive codes pointing to themes. 32 BN conducted the analyses. Data collection, analyses, and results were discussed with the participants and co-authors.
Ethics
In accordance with Danish law, the Danish Data Protection Agency approved this study. The procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975 (revised in 2008). All participants were informed about the study in writing and face-to-face before participation. They were told that participation was voluntary, and they were guaranteed confidentiality and anonymity. Parents were informed that refusal would not affect the care of their infants or the families and they could withdraw at any time. Participants in semi-structured interviews, focus groups, and workshops provided written consent. The research team shared the value that all participants involved could and had the right to PAR's knowledge and actions; we expected that all participants paid respect to each individuals’ experience, concerns, and values. 37
Results
Participants
Twelve fathers, 11 mothers, and 46 health professionals participated in the PAR process. Table 1 presents the participants in the different activities. Furthermore, several fathers, mothers, and staff members were engaged in informal dialogues with the researchers during participant observation. We focussed primarily on the fathers.
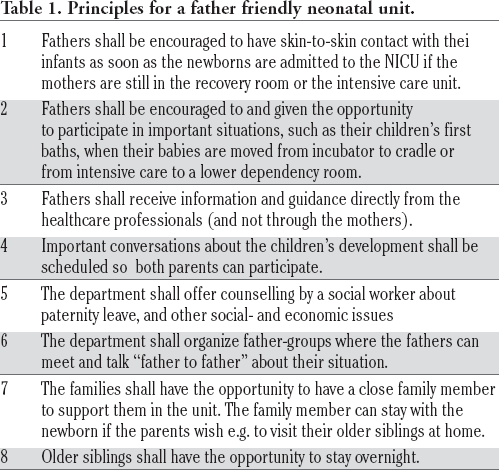
Principles for a father friendly neonatal unit.
Description of the participants involved in the participatory action research.

Participant observation
We spent 29 hours observing during the day, evening, and night shifts. The mothers were always present at the NICU, except when they were either in the recovery room or in the intensive care unit. The fathers were often present late afternoons and evenings on weekdays and during the entire day on weekends. Otherwise, they were at work or at home caring for older siblings. When present in the NICU, the fathers were engaged in feeding or bathing their infants, or helping their wives with practicalities like washing the milking machines. The fathers felt joy and satisfaction being involved; this was illustrated by an observation when a father, who was smiling, told a nurse how he had changed his infant's clothes and diaper several times throughout the night. However, the situation, especially admission to the NICU, was worrying for the fathers. The unease of a father was observed when the doctors and nurses hurried to the NICU with a small newborn laying in an incubator: the intense atmosphere was easily sensed.
The fathers also felt left out. In an informal dialogue, a father stated that there was no attention paid to his situation. He experienced that the staff, as well as the family and relatives, were aware that the situation was hard for the mother, but not for him. He talked about balancing the baby, his wife, work, and the home was difficult for him.
Interviews
We conducted five semi-structured interviews with fathers. Four fathers (28 interviews were conducted) and six mothers (20 interviews were conducted) participated in multi-sequential interviews regularly during their infants’ hospitalization; however, one father was interviewed once after his infant had been discharged. The number of interviews with an individual father and mother ranged from 3-11 and 2-6, respectively.
The interviewed fathers expressed how they felt uncertain at admission because the delivery of their infants turned out differently from what was expected. All fathers expressed a feeling of chaos and of being restless. They felt they were running back and forth to be near their newborns and wives. Two fathers expressed the following: There is chaos inside my mind and My child was delivered by caesarean section, and the mother and child were admitted to different wards; so, I went back and forth between the two wards.
The fathers wished to have paternity leave during the first two weeks after delivery while their infants were in critical condition. I took four weeks of paternity leave because I did not know if our son would survive. I could not work. I thought of them [mother and child] all the time.
Although the fathers had hectic days with work and housework, they still wanted to take part in the care of their newborns at the NICU; however, they also wanted to work. Their needs changed during hospitalization and they were challenged by the everyday humdrum of life when their infants’ health was stable. Two fathers expressed the following: I have never been this stressed before… I take care of the other children at home and of my job; but, I also need to be here. I want to be here, as well and Now, all the days are the same, and every day the same things happen. Maybe I am losing patience because nothing happens, and everything has become routine. Maybe it is the perfect time to start working. The situation is stable now.
The fathers expressed the need to achieve control and oversee their infants progress and they expressed a need to be directly informed: When my wife passes on the information, a little twist cannot be avoided. The mothers supported the fathers’ experiences about being busy. There was little time for fathers to get to know their infants and the fathers felt alone and at unease in the NICU. The mothers needed a place where the couple could talk privately. There is not much time for dad to get to know our infant and I have to be mindful and not to criticize him when he does things incorrect with the child. But it is hard because I am here all the time and know everything.
Focus group with staff
Strategically, an invitation was sent to twelve nurses and two assistant nurses of different expertise (from novice to expert) from the two subunits. Nine nurses and one assistant nurse agreed to participate. Due to suddenly scheduled vacations and sick leaves, four individuals were not able to participate. The nursing staff stated that they barely took care of the fathers. The mothers were more likely to express their feelings; therefore, the focus was turned toward the mothers and infants. When the mothers were ill, the fathers were prioritised, but just until the mothers were healthy. We are not taking good care of father and If the mother is present, she is the one who is given priority because mothers are the most important persons.
Generally, the staff who worked in the afternoons had more contact with the fathers than did the staff working during the day or night shift. Some staff wished the fathers to be more involved in childcare; some staff thought they were too involved: I like when fathers are in the NICU by themselves and they have their own time with their infants and Some fathers take too much space, almost as if they want to take the mothers’ role.
Workshop with parents
We failed to carry out a workshop with the fathers. Twice, they were invited to participate; however, no one accepted. Unfortunately, there were few Danish speaking fathers to ask for participation and those invited gave reasons for not participating (e.g. no babysitter was available for older siblings or the mother was scheduled for a home visit). Therefore, one workshop for mothers was conducted. Five of the invited mothers accepted, five mothers had been discharged at the time of the workshop, and six did not provide any reason for declining the invitation.
From the data already obtained, two reflections were highlighted: i) the importance of the family being together and ii) information and communication. During the workshop, the mothers were provided cards with the following clauses: information and support from the staff, relationship with other parents admitted in the unit, living as a family in the unit, and my child stays in a four-occupancy room. Initially, the mothers individually wrote down their reflections and were asked to choose a material symbolising their reflections (e.g. piece of wood, silver foil, or fur). 34 For example, one of the mothers wrote that she missed her older son, and added a piece of fur symbolizing the love and warm feelings she felt when thinking of him. Afterwards, the mothers worked collectively by telling their stories; finally, they agreed on one good and one bad experience.
The mothers confirmed that the fathers had a tough time in the unit. It was difficult for fathers to network because the physical environment of the NICU did not invite socialization. The mothers expressed that they were always ten steps ahead. Some mother offered the idea of counselling from a social worker. We must pass on all the information to them [partners]. We are here all the time and whatever we do, we are always ten steps ahead (e.g. when taking blood samples and test results) and I wish that a social worker helped my husband about the paternal leave.
Workshop with staff
One workshop for interdisciplinary staff was conducted. All seven invited key staff members agreed to participate. The form of the workshop with the staff members was like the workshop for mothers except for clauses and material. In this workshop, the following clauses were: the importance of the family being together, admission, the child's care and treatment, information and support to the parents, introduction of new colleagues, the family being in a crisis, and the relationship between admitted families. The material was a layout of an imagined NICU where each family was granted a single room. The staff worked individually and collectively on the different issues and how these and new ideas could be implemented in a single-room NICU.
The staff members found that single rooms were an attractive option for the infants and their parents. They also reflected on how they could take care of all family members, if the fathers really wanted to be admitted, if single mothers felt isolated, and if the families could be isolated. The staff also suggested ideas for a father-friendly NICU such as establishing a lounge for families, allowing older siblings to stay overnight, and ensuring that the fathers were treated as importantly as the mothers were.
Study visits
Study visits at 11 NICUs were sources of inspiration. Six NICUs were at university or regional hospitals, which were in different geographical areas of Denmark. Five NICUs were at university or regional hospitals in southern Norway. While visiting the NICUs, the researchers had the opportunity to talk informally with parents about their experiences and with staff about how they cared for the families (especially the fathers).
Focus group with fathers
Three fathers agreed to participate. The fathers confirmed the findings from other activities such as the dilemma between being at the hospital or at work, their wish to be equal co-parents, and experiencing impatience: The focus is on the infant and the mother. As a father, you feel left out and during the first three or four days, I was actually the only one who had contact with him. Of course, my wife was sad that she could not be there; but, for me, it meant that I became closely connected to him, much more than if his mother had been well.
They expressed an idea about setting up a group for fathers, because they wanted to share experiences with other fathers in the same situation: It would be good to have some kind of a network of fathers. We have to be brought together before we can talk to each other, and participation should not be voluntary.
Seminar with staff
Twenty-five nurses, one assistant nurse, one medical doctor, and four managers as well as the first, second, and third authors of this study attended the seminar; there were 34 participants in total. Due to work obligations and illnesses, 14 were unable to attend.
At the seminar, the PAR process and the findings from all activities were presented. Then, to prime the staff, a Norwegian medical doctor discussed his experiences working in a father-friendly NICU. Third, the interdisciplinary staff worked in groups to suggest changes that could meet the identified needs. After the seminar, the research team and the NICU's management discussed the staff's suggestions for changes and agreed on the concept of a father-friendly NICU (Table 1).
Implementation
By testing the concept in clinic practice, we made minor adjustments in the concept based on practical experiences and reflections with participants. For example, a maternal group and a grandparents group were established once a month to supplement the paternal group. To reinforce the implementation process, summaries of the focus group's discussions were sent to the interdisciplinary staff in newsletters; the management and two project nurses discussed the issues. Lastly, supervision of all nursing staff members was planned based on the nursing staff's positive experiences and challenges as articulated during the focus groups.
Discussion
A wide variety of relevant local stakeholders (i.e. 12 fathers, 11 mothers, and 46 health professionals and managers) were involved to capture the complexity of this topic. In collaboration with the participants, the research team obtained knowledge and understanding of the fathers’ needs and wishes that contributed to the concept of a father-friendly NICU.
The validity of PAR is defined by Herr and Andersen's five criteria: i) outcome validity concerns that the solution of the problem be identified; ii) process validity evaluates the actions, reflections, and learning of the individuals or the system under study; iii) democratic validity relates to those involved; iv) catalytic validity refers to the researchers’ and stakeholders’ ability to review the system and their own role in the study and move towards changes; and v) dialogic validity, which is the ongoing reflection with others about the study's validity. 24 We will discuss the validity of this PAR based on the following three criteria: process, democratic, and catalytic validity and discuss PAR as a method to address a key clinical practice problem and thereby improve healthcare. 24
Process validity
Process validity refers to the researchers’ ability to inquire with stakeholders face-to-face to learn about the studied topic. 24 Similar to Charmaz and Swantz,25,32,35 we found that it was essential to be present in the unit, and to be open and interested in every stakeholder's story. Additionally, we learned about everyone's different needs, problems, and challenges by collaboration and communication.
Similar to other research,27-29 we learned that participant observation was an appropriate activity to obtain knowledge of the everyday lives in the NICU and it was an easy way of getting in touch with participants. The participants were available and willing to talk about their daily lives.
Although the researchers were flexible and the interviews were scheduled at a time and location of the fathers’ choice, making appointments was challenging during busy days. It was easy to get in contact with the fathers; however, it was difficult to involve them. Once they had accepted the interview, the fathers were engaged and willing to talk openly about their experiences. Similar to Charmaz, 32 BN experienced a familiarity with the fathers and her confidence was strengthened by the ongoing conversations in the multiple-sequential interviews. Although the fathers’ time was sparse, the interviews provided the opportunity to gain a nuanced story of the lived experiences of the fathers. Surprisingly, the theme of impatience surfaced. This theme might not have been expressed if the researcher had only interviewed the fathers once.
Rahman noted that objectivity in action research means to move from subjective to collective agreement. 38 The group activities in this PAR engaged the stakeholders in new cooperative relations and generated ideas for a father-friendly NICU. Like Rahman, we learned that these group activities advanced both individual knowledge and resulted in a consensus among the participants, displaying social confirmation. 38 For instance, when the nurses in the focus group shared their experiences, each of them articulated why and how they supported fathers; this way, both individual and collective attitudes towards fathers were revealed.
Even though the mothers found it challenging to engage with the different materials during the workshop, it seemed like these materials supported the exploratory process and generated new understandings and ideas. They became engaged and wanted to continue discussing and sharing experiences beyond the time scheduled. Similar to Sanders, 34 we experienced the effect of using individual and collective activities in the workshop. The activities encouraged the participants to share experiences and primed new ideas (e.g. the layout of the imagined NICU made the discussion realistic). After this workshop, the staff had many reflections. A nurse wrote in an e-mail: I felt clearly primed last night when I cared for the small children. I had the image of the imagined NICU. Everything I did, I put into an imagined world of a family-centred unit. It was not so bad. Many of our reservations come from abstractions of our known world and not from the new world.
Unfortunately, we failed to conduct a workshop with fathers. Reinicke found that fathers might find it difficult to participate in a group activity with other men; 39 however, we found that the fathers in this study engaged in the group discussion with other fathers. They did not know each other prior to the group discussion; however, it appeared they felt comfortable talking freely and confidentially about the preliminary knowledge and their own experiences, needs, and wishes. One father said: We men think similarly. It is good to talk with other fathers who have the same experiences.
Although the staff had different attitudes towards fathers, they reached a consensus, which was that the NICU needed to be more father friendly. We also experienced, as also reported by Reason and Bradbury, 23 that when the staff understood their own experiences, they were more focused on the future. They were motivated and engaged in making suggestions for local changes to meet the fathers’ needs. This was an important stage because, like Swantz noted, if knowledge is not incorporated into the NICU's culture, the changes would not be practical or workable. 35
It seemed reasonable to critically reflect on the fathers and mothers nonattendance at the seminar. 24 Could their collaboration in the last activity have provided further positive changes? In addition, focus groups with medical doctors might have provided novel information because doctors had a different relationship with the fathers. However, the medical doctors’ experiences and perspective were included in the study by their involvement in the workshop and the seminar. Furthermore, dialogs throughout PAR with the medical doctors were of importance to nuance the attitudes towards fathers by the different healthcare professionals.
Democratic validity
Democratic validity refers to how the researchers collaborated with the stakeholders. 24 Did we involve all participants who had a stake in the problem? Did the researchers listen carefully and non-judgmentally?
As Herr and Anderson 24 and Charmaz 32 also found, one of the strengths in this study's PAR was the wide variety of relevant local stakeholders involved to capture the complexity of the topic. The stakeholders had different backgrounds, interests, and roles; therefore, they also had different perspectives and experiences. The position of BN allowed her to conduct the study; since she was familiar with the staff, she was a gatekeeper and helped the co-researchers gain access to the staff. Similar to Brydon-Miller and Bergold,25,37 we found that it was important that the researchers had respect for each individual's experiences, concerns, and values. Moreover, it was important to be nonjudgmental if the participants expressed something discrediting to ensure it was a comfortable atmosphere. Based on these principles, we gained the opportunity to learn, understand, and collaborate with the participants; consequently, we feel this gave us valid data. For example, when the nursing staff in the focus group discussed their personal view that fathers were involved too much, it was a sign of an atmosphere of comfort and trust. In a focus group, social roles can affect what is shared. 33
As Herr and Anderson noted in their work, 24 we learned that it was very important to collaborate with the staff and managers to ensure that the concept would be feasible and sustainable because we had no authority over any of those involved. The sample of fathers required critical reflection. Although the sample was relatively small, the involved fathers represented a variety of family constellations. If the project had been extended, we could have enrolled other fathers who perhaps had different needs and experiences (e.g. fathers who were not present in the NICU or fathers who were discharged). However, this was not possible in the context of this project. According to Reason and Bradbury and Herr and Anderson,23,24 we obtained rich and detailed data because of the multiple methods used and the social agreement in the group discussion of fathers.23,24 As discussed earlier, the parents did not participate in the last phase of the PAR, which was a limitation.
Catalytic validity
Catalytic validity refers to the degree that the researchers reflect on the ongoing process and their role as researchers. 24 As Herr and Anderson described in their guidebook, 24 we found that the insider-outsider team captured the needs of different resources in a team. Fruitfully, as an outsider within, BN involved insiders and outsiders with relevant skills and resources to be a part of the research team. Resources and skills in qualitative methods, academic guidance, and participatory design were required. We agree with Herr and Anderson that a team of insider/outsider researchers with different positions and ways of understanding strengthened the self-insight and the reflections when collaborating with participants and analysing data. 24 We benefited from the different skills, positions, and the fact that both sexes were represented in the research team, because there was always one person who was either familiar with the setting or the methods used. Like other researchers,27,29,32 we also found that research notes were an efficient method to use during activities and interviews.
Conclusions
This case study contributed insight into the role and importance of PAR in clinical practice. By engaging the stakeholders in the process, the culture of the NICU became open to reflection and action. It was very important to understand the purpose and context of the activities and to use them accordingly to the participants. By using the right activities in the right context, we gained an opportunity to promote participants’ creativity. This required the researchers to be flexible and to be aware of PAR as a time-consuming approach.
This small case study may have implications on how PAR can be employed to ensure that changes, which will help develop a more father-friendly NICU, are based on participants’ experiences and are feasible and sustainable.
Footnotes
Acknowledgements
We thank fathers, mothers, interdisciplinary staff and managers for taking part in this study. We also thank master student in educational anthropology Mette Rahbek and service designer Rikke Løwenstein for their contributions to the research. The study was supported in part by the Institute of Regional Health Research, University of Southern Denmark, Research Council Lillebaelt Hospital, Sister Marie Dalgaard Foundation, and the Department of Paediatrics, Lillebaelt Hospital.
Conflict of interest: the authors declare no potential conflict of interest.
Contributions: BN was primary responsible for conception and design; analysis and interpretation of data; drafting the article; HJ, contributed to conceptualization of the design and the article, discussed and contributed to the content and theoretical framing of the article; JA and PEK, have substantially contributed to design of the study; analysis and interpretation of data; revising the paper critically for important intellectual; JFG, contributed substantially to study design and practical implementation, data interpretation and revising of the article.