
Abstract
Background
We report outcomes on ≥ 4 compared with < 4 exchanges/day in a Chinese cohort on continuous ambulatory peritoneal dialysis (CAPD).
Methods
Data were sourced from the Baxter (China) Investment Co. Ltd Patient Support Program database, comprising an inception cohort commencing CAPD between 1 January 2005 and 13 August 2015. We used cause-specific Cox proportional hazards and Fine-Gray competing risks (kidney transplantation, change to hemodialysis) models to estimate mortality risk on ≥ 4 compared with < 4 exchanges/day. We matched or adjusted for age, gender, employment, insurance, primary renal disease, size of CAPD program, year of dialysis inception, and treatment center.
Results
We modeled 100,022 subjects from 1,177 centers over 239,876 patient-years. Of these subjects, 43,185 received < 4 exchanges/day and 56,837 ≥ 4 exchanges/day. The proportion of patients on < 4 exchanges/day varied widely between centers. Those on < 4 exchanges/day were significantly older, more often female, of unknown employment, and from rural China. In the various models, ≥ 4 exchanges/day was associated with a significantly lower risk of death by 30% – 35% compared with < 4 exchanges/day. This beneficial effect was greatest in younger and rural patients.
Conclusions
In this Chinese CAPD cohort, ≥ 4 exchanges/day was associated with significantly lower mortality risk than < 4 exchanges/day. Analyses are limited by residual confounding from unavailability of important prognostic covariates (e.g., comorbidity, socioeconomic factors) and data on residual renal function, peritoneal clearance, and transport status with which to judge the clinical appropriateness of CAPD prescription. Nonetheless, our study indicates this area as a high priority for further detailed study.
Keywords
It is well accepted that the Chinese are a discrete population in dialysis medicine. They have a significantly lower adjusted mortality rate than European patients, with only half of this difference attributable to race-specific background population death rate (17). A large unknown is whether Chinese patients have different dialysis dose-outcome relationships compared with European ones (18,19). For continuous ambulatory peritoneal dialysis (CAPD), it has been argued that the smaller size of Asians in general allows for higher peritoneal small solute clearance per volume of distribution (Kt/V) despite lower dialysis doses (L/day) (20). The dialysis regimen of 3 2-L exchanges per day represents a common and potentially biochemically adequate practice in China and Hong Kong (21–23). In China, as in many other countries in Asia, the use of 3 exchanges per day is considered cost-effective and is a core component of the economic value proposition of the “PD first” concept for payers and policymakers (24 25 26 27-28).
There are limited data in Chinese patients comparing mortality risk on < 4 times 2-L exchanges per day for maintenance dialysis versus the more usual practice of 4 times per day in most economically advanced countries. In several single-center cohort studies, outcomes on 3 times 2-L exchanges per day appear to be satisfactory (22,23,29–33), albeit often in the presence of considerable residual renal function (22) or in the first 48 months after dialysis inception (32). In 2 clinical trials, however, “more” CAPD was arguably better than “less.” In the first, increasing the CAPD dose from 3 to 4 exchanges per day improved dietary protein intake and possibly reduced hospitalization (34,35). In the second, a Kt/V of ≥ 1.7 resulted in significantly better outcomes for patients than a Kt/V of < 1.7 (30). Overall, it can be reasonably concluded that there is likely to be a minimum solute clearance target that should be achieved for Chinese PD patients. It can therefore not automatically be assumed that 3 exchanges per day is clinically adequate for all patients.
In this study, we explore the question of clinical outcomes for < 4 versus ≥ 4 times 2-L exchanges per day in a modern cohort of Chinese CAPD patients in an observational study, adjusting for a limited range of clinical and socioeconomic variables in cause-specific and competing risk models.
Methods
Study Design
We performed a retrospective cohort study using an “as treated” framework (“did the exposure that the patient actually received affect mortality?”) rather than an intention to treat model (“did the exposure that the patient initially received affect mortality, irrespective of subsequent changes that occurred along the way?”) (36). Of note, all patients in this study were treated with CAPD using twin-bag 2-L Dianeal PD (Baxter International Inc, Deerfield, IL, USA) systems. Also of note, 2.5- or 3-L PD systems and polyglucose PD fluid are not available from or sold by Baxter in China.
The study execution was subjected to the conditions of an established governance pathway developed by Baxter Healthcare (Asia) Pty Ltd that is provided in Appendix 1 (available as online supplementary material). This pathway is applied to epidemiological studies from the Asia-Pacific region if the studies contain substantial contribution and content from Baxter Healthcare. This process is described in detail elsewhere (37). As a result of the pathway, the study was reviewed and approved by an external ethics committee, the study data inspected and analyses replicated by The Arbor Research Collaborative for Health (www.arborresearch.org), and the interpretation of findings in the local healthcare context established by consensus at a face-to-face steering committee meeting of experts convened in collaboration with the leadership of the China Society of Nephrology.
Participants and Data Source
For this research, data were sourced from the Baxter Patient Support Program, in a manner that is broadly akin to similar studies from other countries (38 39 40-41). In China, Baxter (China) Investment Co. Ltd funds support services to patients treated with its PD products, consistent with local regulations applicable to patient support programs and post-marketing research. The program itself is administered by a separate legal entity that provides patients with regular telephone support and contact, value-added supplies such as treatment log books, and material providing dietary and lifestyle information to supplement hospital education. Patients on Baxter products are enrolled with the Patient Support Program provider and given written and in-person notification that provide an “opt-out” option.
After initial contact, there is collection of a limited amount of personal data from patients. The data include date of PD catheter insertion, the date of and reason(s) for discontinuation of Baxter products, basic patient demographics, cause of end-stage kidney disease, PD sub-modality and prescription, details of patient occupation and medical insurance, and center of care. The Patient Support Program provider holds these data in compliance with local regulations, but makes de-identified datasets available to Baxter upon request.
We created a cohort of de-identified patients who initiated PD with Baxter products between 1 January 2005 and 13 August 2015 in China. We excluded patients if they had records of less than 90 days, received automated PD at any time, or were less than 1 year of age. We also excluded those with a recorded age of ≥ 95 years as likely ascertainment or recording error. The remainder were followed up until death, dropout from discontinuation of Baxter PD products, loss to follow-up for other reasons, or 13 November, 2015, whichever occurred first. Although not precisely known, our cohort is estimated to represent ∼70% of China's PD population.
Exposure Variables
The primary exposure was the number of 2-L exchanges of CAPD fluid per day, dichotomized to < 4 exchanges per day and ≥ 4 exchanges per day. In the source dataset, these data are collected from initial patient enrolment and updated at each 3-monthly episode of follow-up between the Patient Support Program provider and patient. These changes are not recorded along the way, but rather overwritten at last follow-up—there is no record of changes in prescription that occur along the way.
We modeled the following patient-related factors: age, gender, primary kidney disease (diabetes, glomerulonephritis, hypertension, other/unknown), occupation (employed, student, unemployed, unknown), size of the PD program, approximately equally-sized tertiles of era of dialysis inception (2005 – 2009, 2010 – 2012, 2013 – 2015), and their de-identified center of treatment. Continuous covariates other than age were modeled as clinically relevant quantiles in order to avoid the assumption of linear relationships.
We also modeled medical insurance status (Medicare for migrant workers, New Rural Cooperative Medical Scheme/ System [NRCMS], self-pay (assuming unknown to be self-pay), Urban Employee Basic Medical Insurance [UEBMI], Urban Resident Basic Medical Insurance [URBMI]). As background, CAPD patients in China who have insurance usually have to co-pay around 20% of the cost of their dialysis. This co-pay differs by insurance—90% of the total cost is reimbursed to hospitals by UEBMI (these patients are urban and employed and tend to be wealthier), and 70% – 80% reimbursed by URBMI and NRCMS. Patients who are self-pay are usually those who cannot make the minimum annual fee to their personal insurance account; these are usually the urban unemployed or from very poor rural areas.
Outcome Variable
The primary outcome for the analysis was patient death. The recorded outcome of “withdrawal from dialysis” was included in models as death.
Statistical Methods
We constructed exposure-outcome models to estimate the effect of CAPD exchange number on mortality. We used 5 approaches in the analysis, described in Table 1. Given the etiological rather than prognostic nature of the research (42), the first analysis we performed was designated as the primary one, using cause-specific Cox proportional hazards analysis censoring for switch to hemodialysis (HD), kidney transplantation, discontinuation of Baxter PD products and loss to follow-up for unrecorded reasons. Hazard ratios (HRs) calculated using this approach can be interpreted as actuarial probabilities: mortality rate ratios “among those patients who are alive, but had not (yet) experienced a competing event.” We included a gamma-distributed shared frailty using the center of initial dialysis treatment as the group, assuming that patients did not change their dialysis center during treatment, implemented using the “shared” facility of Stata (Statacorp, College Station, TX, USA).
Modeling Approaches Used for Analysis
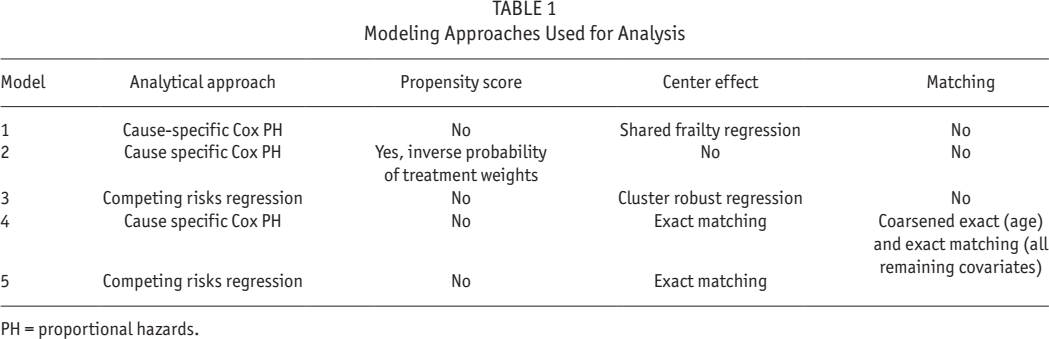
PH = proportional hazards.
In the second approach, we repeated the primary analysis after the weighting by the inverse probability of treatment (≥ 4 versus < 4 exchanges per day) for each individual. This was implemented with a propensity score (PS), using the “iweight” facility of Stata. The PS was computed from a logistic regression model, with < 4 versus ≥ 4 exchanges per day as the dependent variable. All of the available covariates were used in creating this model. We then calculated the inverse probability of treatment as 1/PS for those on ≥ 4 exchanges per day, and as 1/(1-PS) for those on < 4 exchanges per day. Of note, the use of a PS as a stratifier or weight is preferable to using it as a covariate in the outcomes regression model. The former approaches allow more flexible specification of the PS model and clearer interpretation of coefficients and interactions in the outcome model. In this model, we did not account for correlated data within centers of dialysis: shared frailty or robust cluster estimation is not implemented simultaneously with weights using Cox regression in Stata.
In the third approach, we modeled switch to HD and kidney transplantation as competing risks based on Fine and Gray's proportional subhazards model (43). Patients were censored in models at the time of discontinuation of Baxter PD products and loss to follow-up, assuming independent and non-informative censoring (time to event and time to censoring are independent, conditional on the level of covariates). Subhazard ratios (SHRs) calculated using this approach can be interpreted as actual probabilities: mortality risk ratios “among those patients who are alive including those who had been switched to HD or been transplanted, but had not (yet) discontinued Baxter PD products or been lost to follow-up.” We did not model PS: weighting or stratification is not implemented in Fine and Gray's proportional subhazards regression in Stata. In this model, we accounted for correlated data within centers of dialysis by robust cluster estimation.
In the fourth and fifth approaches, we performed analyses between matched samples of patients on < 4 versus ≥ 4 exchanges per day, created with exact 1:1 matching on all covariates (gender, primary kidney disease, occupation, medical insurance, year of dialysis inception, and center of treatment) except age. For age, we used coarsened exact matching by categorizing age into 20 strata of equally sized age intervals of between 4 – 5 years, and matched within those strata. Exact and coarsening exact matching was implemented using the “cem” facility of Stata (44 45-46), with algorithms that have important advantages over other probability-based systems such as those based on PS. (47,48). Exact matching creates samples that are balanced at both subject and population levels rather than just the latter, and avoids modeling assumptions used for defining what constitutes a suitable match. In the fourth approach, we used univariable cause-specific hazards analysis, and in the fifth and final approach we used univariable competing risks regression, as described above.
In multivariable models, we initially included all available covariates, removing those with the highest p value from 2-tailed Wald tests of coefficients, using the partial likelihood ratio test to compare the new reduced model with the older larger one. We based final confounder selection upon both biological plausibility and contribution to the comprehensibility of the model, and also the significance of the covariate within the model as assessed by the 2-tailed partial likelihood ratio test p value at a level of 0.2 when jointly adjusted for other covariates. We modeled primary renal disease, occupation, and type of medical insurance using deviation from means coding (49), since there is no particular rationale for the selection of 1 group over the other as a reference group.
We used 2-way interaction terms in the primary main-effects model to test effect modification by age, primary renal disease, occupation, and medical insurance. We chose these interactions as being clinically plausible, on the basis of both published literature as well as cumulative clinical experience. Interactions were assessed using the 2-tailed Wald test p values as a guide to selecting interaction terms for testing, with significance within the model using the likelihood ratio test (p < 0.05).
The assumption for proportional hazards for the final models was assessed formally by the use of scaled Schoenfeld residuals, and visually by -ln [-ln(survival)] versus ln(analysis time) plots for modality, adjusted for confounders. We assessed overall goodness of fit visually by comparing plots of Kaplan-Meier observed survival curves with the Cox predicted curves for modality.
Where necessary, we made comparisons between groups using the Fisher's exact test, and Mann-Whitney U (or Kruskal-Wallis) tests as appropriate. We computed effect size statistics using Cohen's d for continuous variables and Cohen's w for categorical variables (50,51).
A number of factors were not measured in this study (e.g., other comorbidity, residual renal function, medication, functional status, health literacy, etc.), which might confound the relationship between modality and mortality. We therefore performed sensitivity analyses to estimate the extent to which bias due to unmeasured, hence uncontrolled, confounding may have over- or under-estimated the true effect. We used methods previously described in the literature (52 53 54 55-56), and conducted analyses where significant effect of the primary exposure was observed. We varied the prevalence of the unmeasured confounder among patients on ≥ 4 exchanges per day (reference group) and those treated with < 4 exchanges per day (comparator group), as well as the strength of the association between the unmeasured confounder and mortality risk to reflect various plausible scenarios.
Analyses were performed using Stata Intercooled MP/14.1 (StataCorp, www.stata.com).
Results
Participants
The cohort included 100,192 subjects with 23,838 deaths over 240,116 patient-years of follow-up. There were 87,183 subjects from 1,134 centers with sufficient data for modeling, with 19,463 deaths and 12,003 who were transferred to HD or transplanted over 222,322 patient-years. Other causes of dropout from Baxter products included loss to follow-up in 5,888 patients, transfer to other brands of PD system in 4,835 patients, and other reasons in 3,023 patients. Table S1 summarizes the study cohort and excluded cohort due to missing data at dialysis inception (the point of commencement of dialysis). The excluded cohort comprised 13% of the potential study cohort, 12.8% pertaining to the primary exposure variable being missing, and 0.2% to other covariates being missing. Subjects with missing data were more likely to be older, male, self-pay, with an unknown/other cause of primary kidney disease, and from smaller PD programs. Differences between the included and excluded dataset were small or very small in terms of effect size and clinical significance.
Descriptive Data
The distribution of patients by number of exchanges per day is shown in Figure 1. The distribution between < 4 exchanges per day and ≥ 4 exchanges per day by year of follow-up after dialysis inception is shown in Figure 2. The corresponding distribution by center is shown in Figure 3.
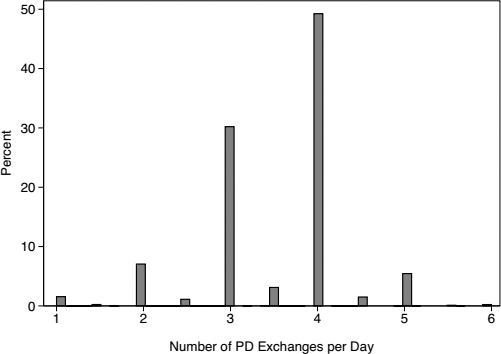
The distribution of number of exchanges per day in the cohort. PD = peritoneal dialysis.
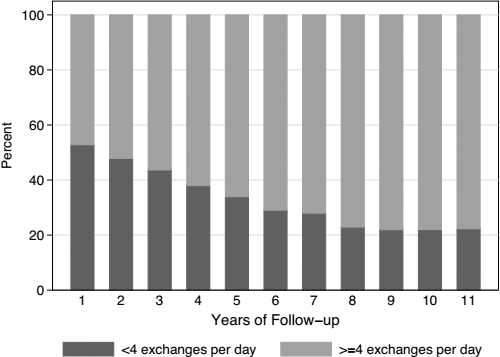
The distribution between < 4 exchanges per day and ≥ 4 exchanges per day over years of follow-up time.
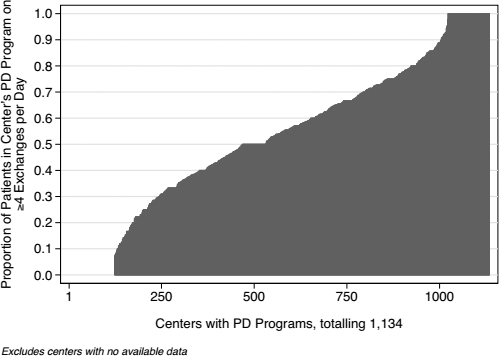
The proportion of patients on ≥ 4 exchanges per day, by peritoneal dialysis (PD) center. PD = peritoneal dialysis.
Table 2 summarizes the clinical characteristics of the final dataset, comparing these characteristics by number of exchanges per day. Those on < 4 exchanges per day were significantly older, more likely to be female, more likely to be of unknown employment, and insured through NRCMS and likely from rural China. These differences were statistically significant, but other than for type of insurance, associated with a small or very small effect size.
Clinical Characteristics of Patients at Dialysis Inception, by Number of Exchanges
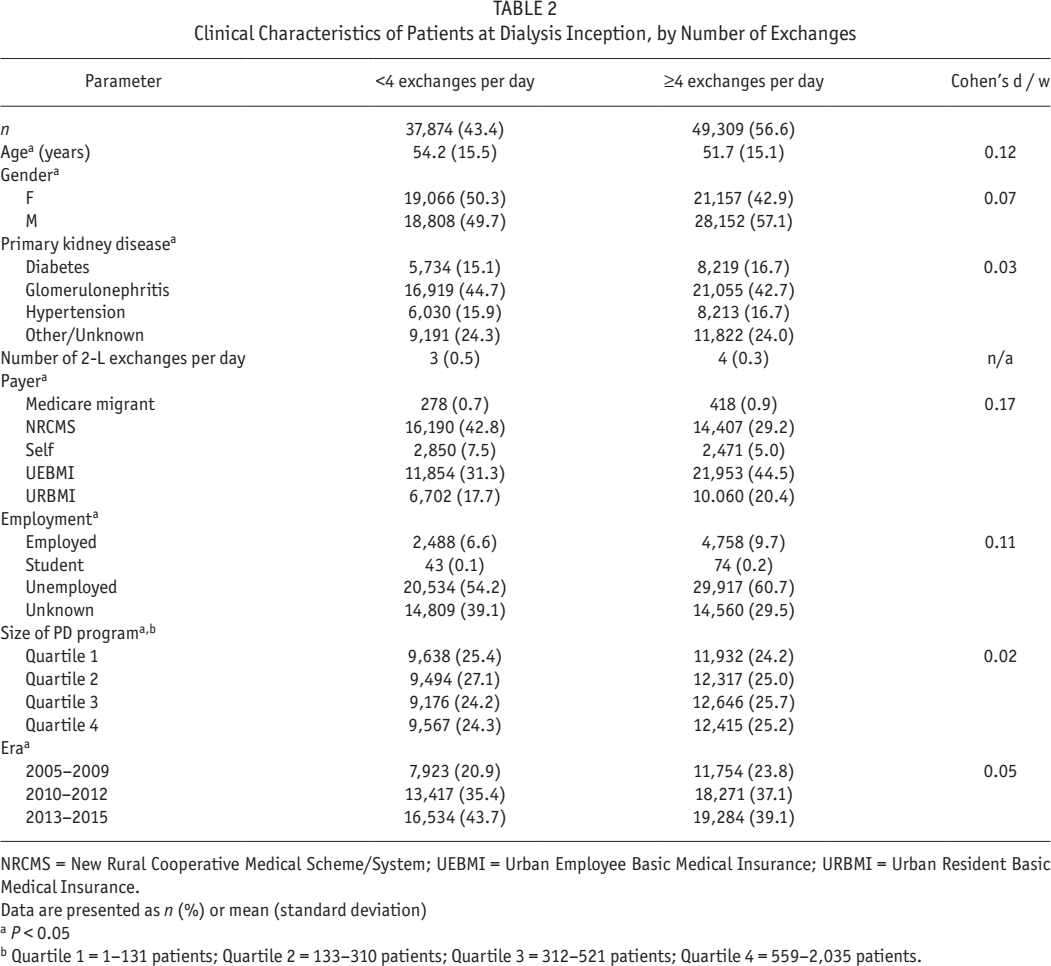
NRCMS = New Rural Cooperative Medical Scheme/System; UEBMI = Urban Employee Basic Medical Insurance; URBMI = Urban Resident Basic Medical Insurance.
Data are presented as n (%) or mean (standard deviation)
P < 0.05
Quartile 1 = 1–131 patients; Quartile 2 = 133–310 patients; Quartile 3 = 312–521 patients; Quartile 4 = 559–2,035 patients.
Main Results
Figure 4 illustrates actuarial and actual probabilities of death. Figure 5 shows main effects from the primary analysis, demonstrating a statistically significant 36% decrease in mortality risk with ≥ 4 exchanges per day relative to < 4 exchanges per day in the final fully-adjusted model. Of note, there is no violation of the proportionality of hazards in the primary model assessed visually (Figures S1 and S2), with good agreement between actual and modeled mortality risk (Figure S3), and no violation of the proportional hazards assumption on formal testing of scaled Schoenfeld residuals for the primary exposure (p = 0.20).
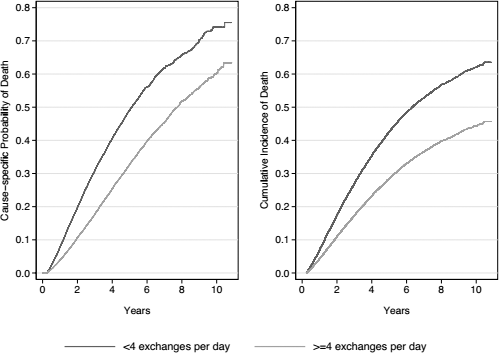
Estimates of actuarial (from Kaplan-Meier estimates) probability of death (left), and actual cumulative incidence (from the competing risks regression) of death (right).
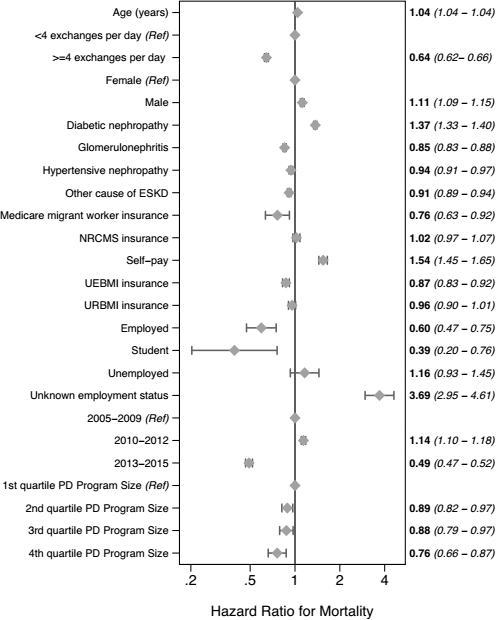
Main effects of the primary model, fully adjusted for the confounders listed in Table 2 (the marker represents point estimates, the whiskers, 95% confidence intervals). ESKD = end-stage kidney disease; NRCMS = New Rural Cooperative Medical Scheme/System; UEBMI = Urban Employee Basic Medical Insurance; URBMI = Urban Resident Basic Medical Insurance; PD = peritoneal dialysis.
Figure 6 shows the effects associated with ≥ 4 exchanges per day relative to < 4 exchanges per day from all models and analytical approaches listed in Table 1. Of note, the matching procedure resulted in 8,015 matched pairs, with the characteristics as shown in Table S2. All of the models show an approximately 30% to 35% decrease in mortality risk with ≥ 4 exchanges per day relative to < 4 exchanges per day in the final fully-adjusted models.
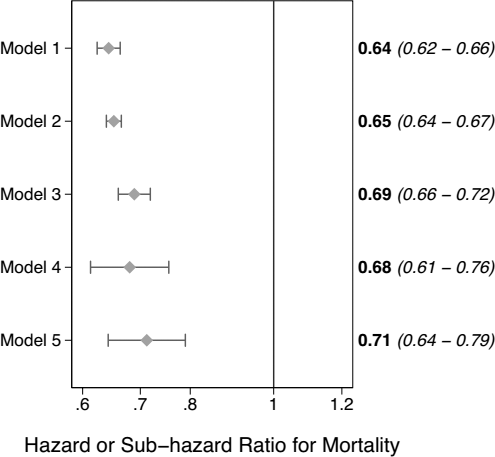
Effects of ≥ 4 exchanges a day relative to < 4 exchanges a day from the models listed in Table 1 (the marker represents point estimates, the whiskers, 95% confidence intervals).
There were significant interactions (p < 0.05) involving age, type of medical insurance, and occupation. There were no significant interactions involving gender and size of center. Figure 7 shows the mortality risk of ≥ 4 exchanges per day relative to < 4 exchanges per day using the primary model with identical confounder control, within subgroups of age, type of medical insurance, and occupation. As can be seen in this figure, the model failed to fit for subgroups of patients with Medicare migrant worker insurance and also for students. These were the 2 smallest groups in their covariate categories at n = 696 and n = 117 respectively, almost certainly leading to violations in the assumption of experimental treatment assignment (or positivity) (57). Overall, the results show that the beneficial effect associated with ≥ 4 exchanges per day is greatest in those who were younger, employed, or had NRCMS insurance. In contrast, the beneficial effect is least in those who are older, of unknown employment, or with urban medical insurance.
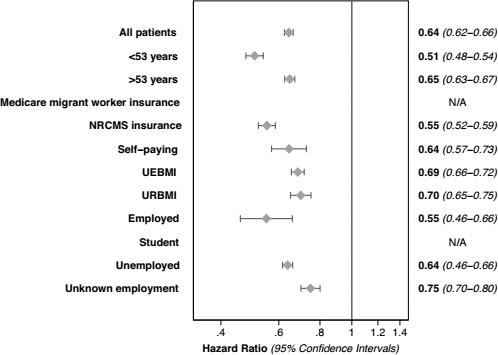
Separate models comparing ≥ 4 exchanges a day with < 4 exchanges, fully adjusted for the confounders listed in Table 2, showing effect modification by categories age, type of insurance, and occupation (the marker represents point estimates, the whiskers, 95% confidence intervals). NRCMS = New Rural Cooperative Medical Scheme/System; UEBMI = Urban Employee Basic Medical Insurance; URBMI = Urban Resident Basic Medical Insurance.
Other Results
Figure 8 summarizes the effect associated wit h ≥ 4 exchanges per day over different landmark start times. The results show that the beneficial effect associated with ≥ 4 exchanges per day is greatest in the early part of a given patient's CAPD course, and decreases with time.
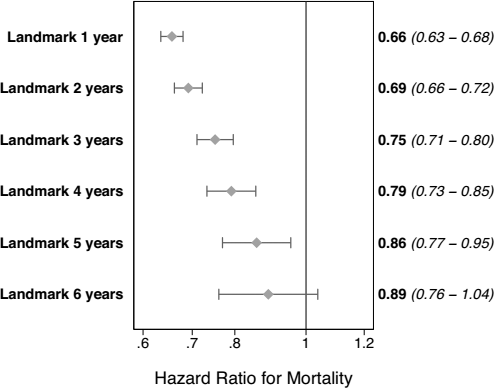
Separate models using the primary analysis comparing ≥ 4 exchanges a day with < 4 exchanges, fully adjusted for the con-founders listed in Table 2, over different landmark start times (the marker represents point estimates, the whiskers, 95% confidence intervals).
The sampling frame for our study included all patients other than infants. There were therefore 791 patients (0.9%) who were less than 18 years of age. Of these, 31 were 5 years old or younger, 79 between 5 and 10 years of age, and the remainder 10 years old or over. The HR (95% confidence interval) for death was 0.64 (0.42 – 0.97) in the sample restricted to those less than 18 years of age, and not different from the main effects model when restricted to those 18 years and over. The difference between the HRs can be assessed using a z-test, which shows that the 2 estimates are not statistically different (p = 0.29).
Table 3 summarizes the results of our sensitivity analyses for unmeasured confounding. These suggest that the associations that we observed for ≥ 4 exchanges per day are unlikely to have been due to confounding only. It is only after adjustment for a strong confounder (i.e., one that produces a greater than 2- to 5-fold decrease in risk of death), with very different distribution between ≥ 4 exchanges per day and < 4 exchanges per day groups (i.e., differing in prevalence between the groups by greater than 20% – 50%), that we see attenuation of the association between number of CAPD exchanges and mortality risk. Adjustment for more moderate confounding produced little change in the results.
Sensitivity of the Main Effects Model to the Inclusion of a Hypothetical Unmeasured Confounder, CD
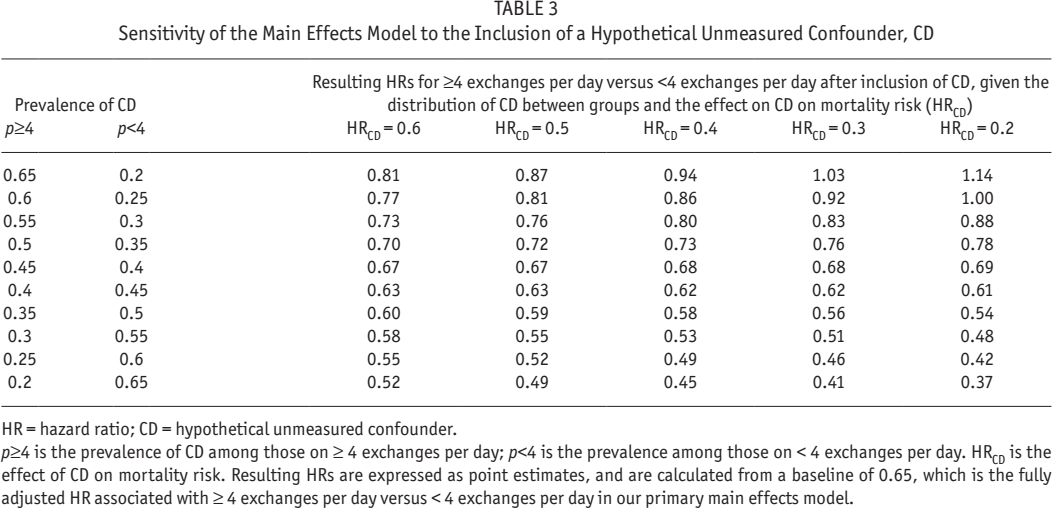
HR = hazard ratio; CD = hypothetical unmeasured confounder.
p≥4 is the prevalence of CD among those on ≥ 4 exchanges per day; p<4 is the prevalence among those on < 4 exchanges per day. HRCD is the effect of CD on mortality risk. Resulting HRs are expressed as point estimates, and are calculated from a baseline of 0.65, which is the fully adjusted HR associated with ≥ 4 exchanges per day versus < 4 exchanges per day in our primary main effects model.
Discussion
Overall, there was a 9.9% annual mortality rate in our cohort, excluding the known high mortality risk in the first 90 days after dialysis inception (58,59). This calculation suggests excellent survival on PD in China in comparison with other similarly calculated estimates in the literature from other countries or settings.
The results of our analyses show that the survival of patients receiving ≥ 4 CAPD exchanges per day in the cohort was superior to that of those receiving < 4 exchanges per day, adjusted for a number of other covariates. Our results also suggest that the benefit associated with ≥ 4 CAPD exchanges per day decreases with time on PD. It is important to note, however, that these results cannot be considered definitive, and the causal effect of number of exchanges per day on patient survival is still a matter for further investigation. This is because of 2 important limitations of our study, which are discussed below.
Firstly, our data do not contain important recognized risk factors for mortality, such as details of clinical comorbidity, biochemical, socioeconomic, medication, and health services data. We were, however, able to include and adjust for the usual core demographics and primary kidney disease, and some other important predictors that many other studies do not include. As with the companion articles published along with this one, insurance status and occupation were powerful predictors of outcome, as would be expected (60 61 62-63). Size of the PD program was also included and was a significant predictor of outcomes; this variable is accepted as a general indicator of program infrastructure and expertise (64 65 66-67).
Secondly, our data do not contain peritoneal clearances and peritoneal ultrafiltration (UF). Although we have used sophisticated statistical methods, a causal relationship between number of CAPD exchanges, increase of peritoneal clearances/UF, and survival cannot be confirmed because of the study design. To explain further, it could be that the risk factor of < 4 exchanges a day is just an epiphenomenon or “marker,” and those patients subjected to this practice pattern are also subjected to other risk factors that are more responsible per se for this excess mortality. Such associated risk factors might include inadequate PD training, inadequate chronic PD management, lack of cardioprotective medication, excess peritonitis, etc. However, in the absence of other data and in the cumulative clinical experience of the research team, it seems likely that inappropriate prescription of PD exchanges per day is contributing to at least some part of the observed excess mortality.
In economically advanced countries, < 4 dextrose exchanges per day is a prescription most often seen in those patients who are starting dialysis, administered as an incremental prescription that increases over time (68 69 70-71). Observational evidence suggests that incremental PD can provide adequate dialysis in those with sufficient residual kidney function (72 73 74-75). Cumulative clinical experience with this approach is increasing (76,77), as both a means of achieving better outcomes and also managing constrained resources (78,79). There are specific conditions that need to be met for incremental dialysis to be successful: it requires a timely start to dialysis to ensure adequate residual renal function, close monitoring and prompt intervention to meet total solute clearance and ultrafiltration targets, and patients who are adherent to both dietary and lifestyle restrictions as well as the monitoring plan (80).
In China, the practice of < 4 exchanges per day is clearly different from that reported by developed nations. This is can be seen by comparing Figures 1 – 3 (practice patterns in our cohort) to Figures S4 – S6 (corresponding practice patterns from the Australia and New Zealand Dialysis and Transplant [ANZDATA] Registry [personal communication Prof Stephen McDonald]). Overall, there is a larger proportion of patients treated with < 4 exchanges per day in China, across all vintages of those on PD, with wider center variation in their routine prescription of < 4 exchanges per day.
Our data suggest that the selection of patients for < 4 exchanges per day may not always be appropriate in China. There is a preponderance of older patients and females treated in this manner, which at face value does not seem inappropriate. However, there is also a preponderance of patients with unknown employment status and rural patients treated in this manner, suggesting that patients may be resorting to this practice for reasons of financial burden and limited access to care. All of these patients have an excess mortality associated with this practice pattern, suggesting that they may not be meeting total minimum solute clearance and ultrafiltration targets. Our study demonstrated a decreasing benefit associated with ≥ 4 CAPD exchanges per day over time. This could be because healthcare workers shift inappropriate or deteriorating patients from < 4 exchanges per day to ≥ 4 exchanges per day, as their inadequate response to therapy becomes apparent. This speculation is consistent with the cumulative clinical experience of the authors. As stated above, we are not able to test these hypotheses because of limitations in the study design and included data.
Notwithstanding these uncertainties, our study suggests some opportunities for further study within target populations. Self-pay patients are clearly the patients with the least access to healthcare and poorest outcomes on CAPD in China, but are in fact a decreasing demographic—the vast majority of patients in China are insured these days. Patients of unknown employment are probably the next most disadvantaged in terms of access to healthcare and are usually defined as having only episodic or seasonal work. These patients receive < 4 and ≥ 4 exchanges per day in equal amounts, but curiously have the least benefit associated with prescription of ≥ 4 exchanges per day. In the authors’ cumulative clinical experience, this is because when such patients are prescribed ≥ 4 exchanges per day, they often do not adhere to the prescription—due to financial reasons, they stay on < 4 exchanges per day, with relative under-dialysis, thereby reducing the apparent benefit of being treated with a higher dose prescription.
Finally, rural patients with NRCMS insurance are preferentially treated with < 4 exchanges per day in our cohort but have a greater-than-average benefit associated with prescription of ≥ 4 exchanges per day. Of note, a given patient's insurance status reflects both personal socioeconomic status and also the center effect arising from their care setting. For NRCMS patients, both factors may be important. It is therefore desirable to separate the effect of rurality-associated personal socioeconomic status on mortality risk from the effect of rurality-associated center practice patterns. Accordingly, further research by this team is underway to categorize each center in our study by rurality, level, and province and then quantify the independent effect of center characteristics on patient outcomes. In this way, we hope to identify opportunities for improved health service delivery in potentially underserviced and sensitive populations.
Conclusion
There are several other limitations to our study in addition to those discussed already. In terms of external validity, practice patterns in China are often different from those in published cohort studies, which in themselves mostly come from International Monetary Fund advanced economies. For instance, icodextrin is unavailable and automated PD (APD) uncommon in China. Both have an uncertain effect on patient mortality in randomized controlled trials, but are associated with improved mortality in several cohort studies, especially in high peritoneal transporters. As such, the external validity of our study is limited for developed or advanced economies but still high for the majority of the world's PD population, which is to be found in Asia and for whom icodextrin is similarly unavailable.
In terms of internal validity, and perhaps most importantly, we could not model dynamic changes in the number of PD exchanges since the database only captured prescription at last contact with the Patient Support provider. Therefore, some of the patients might have been on ≥ 4 exchanges per day initially and then moved to < 4 exchanges per day at a palliative stage of their course, so-called “decremental dialysis.” The absence of any longitudinal dose information in our study does not allow us to rule this out, although it is anecdotally not particularly common in China as a customary practice. Moreover, Figures 2 and 3 suggest that < 4 exchanges per day is a prevalent practice at all points post-dialysis inception, and a customary practice in some centers but not others. It is our speculation the if any causal relationship exists between < 4 exchanges per day and mortality risk, then it is directionally arising from the practice pattern, rather than the outcome.
As a final comment, many factors may influence survival independently of peritoneal clearance and ultrafiltration. However, many of these factors will also have an impact on the decision as to how many CAPD exchanges will be prescribed. For example, in patients with worse prognosis and/or functional impairment, a lower number of exchanges may be prescribed, since nephrologists feel that these patients’ quality of life is more important than reaching high levels of adequacy. Nevertheless, these latter patients would have a high mortality independent from the number of CAPD exchanges. It must be remembered that mortality alone is not only or indeed always the most important outcome of dialysis therapy, and that even if it is generally accepted that ≥ 4 exchanges per day is superior for mortality, the decision of what CAPD prescription is best for the patient has to be made on an individualized basis.
In conclusion, our study suggests that there is a relationship between “as treated” PD dose and mortality risk in China, with lower mortality risk associated with those treated with ≥ 4 compared with < 4 exchanges per day in that country. Despite the generally good survival of PD patients in China, this represents a major potential opportunity to improve outcomes in the future.
Footnotes
Acknowledgments
We would like to thank Dr Jarcy Zee for her expertise and patience in providing an analytical review of our models and data, and the Arbor Research Collaborative for Health for their support of this initiative.
The results presented in this paper have not been published previously in whole or part, except in abstract format. MRM, QY, and JS are full-time employees of Baxter Healthcare. MRM is also an adjunct Associate Professor of the University of Auckland (New Zealand) and a part-time employee of Counties Manukau Health (New Zealand) as a clinical nephrologist.