
Abstract
Background
Incremental dialysis utilizes gradually increasing dialysis doses in response to declines in residual kidney function, and it is the preferred renal replacement therapy for patients who have just transitioned to end-stage renal disease (ESRD). Incremental peritoneal dialysis (PD) may impose fewer restrictions on patients’ lifestyle, help attenuate lifetime peritoneal and systemic exposure to glucose and its degradation products, and minimize connections that could compromise the sterile fluid path. In this study, we utilized a 3-pore kinetic model to assess fluid and solute removal during single daily icodextrin treatments for patients with varying glomerular filtration rates (GFR).
Methods
Single icodextrin exchanges of 8 to 16 hours using 2- and 2.5-L bag volumes were simulated for different patient transport types (i.e., high to low) to predict daily peritoneal ultrafiltration (UF), daily peritoneal sodium removal, and weekly total (peritoneal + residual kidney) Kt/V (Kt/VTotal) for patients with residual renal GFRs ranging from 0 to 15 mL/min/1.73 m2.
Results
Daily peritoneal UF varied from 359 to 607 mL, and daily peritoneal Na removal varied from 52 to 87 mEq depending on length of icodextrin exchange and bag volume. Both were effectively independent of patient transport type. All but very large patients (total body water [TBW] > 60 L) were predicted to achieve adequate dialysis (Kt/VTot al ≥ 1.7) with a GFR of 10 mL/min/1.73 m2, and small patients (TBW: 30 L) were predicted to achieve adequate dialysis with a GFR of 6 mL/min/1.73 m2.
Conclusions
A single daily icodextrin exchange can be tailored to augment urea, UF, and Na removal in patients with sufficient residual kidney function (RKF). A solitary icodextrin exchange may therefore be reasonable initial therapy for some incident ESRD patients.
An incremental approach to dialysis, where the dose of dialysis is progressively increased over time as required to accommodate for gradual loss of kidney function, may provide a solution for several of the above issues. While the potential benefits of incremental dialysis are just now being evaluated for HD, recommended dosing of PD has conventionally been guided by successive measurement of total clearance (RKF clearance and dialysis clearance), with progressive increases in PD dosing as RKF decreases over time (8–11).
Nearly half of all patients in the United States initiate dialysis with an estimated glomerular filtration rate (eGFR) of > 10 mL/min/1.73 m2 (12,13). Similarly, the mean eGFR at initiation of RRT in the United Kingdom is 8.6 mL/min/1.73 m2 (14). While this is not necessarily representative of practices elsewhere in the world, it is likely that patients incident to end-stage renal disease (ESRD) often start dialysis with some level of RKF. While application of incremental PD using 2–3 glucose-based exchanges could well be applicable to many of these patients, use of a single exchange using icodextrin, a 7.5% glucose polymer long-dwell peritoneal dialysis (PD) solution (Baxter Healthcare Corporation, Deerfield, IL, USA) devoid of glucose and with low levels of glucose degradation products, may be even more palatable and effective in addressing the needs of these incident patients. The colloidal properties of icodextrin that enable effective removal of solutes and water over extended dwell times independent of peritoneal membrane transport status have been amply described (15 16-17).
In this study, we utilized a 3-pore kinetic model to predict fluid and solute removal for different patient transport types and evaluated the adequacy of single daily icodextrin treatments for patients with RKF.
Methods
Single daily icodextrin (7.5%) exchanges of 8 to 16 hours with 2- and 2.5-L bag volumes were simulated using a modified 3-pore kinetic model identical to one described previously (18). Simulation runs representative of different patient transport types (i.e., high, high-average, low-average, and low) were per formed using patient parameters determined from peritoneal equilibration tests (PETs) performed in centers around United States and Canada as a part of the TARGET adequacy initiative, as described in previous publications (18,19). Patients who participated in the TARGET study were categorized according to patient transport types as determined from 4-hour PET creatinine dialysate-to-plasma concentration ratios. Model parameters for each patient were estimated using the PD Adequest software (Baxter Healthcare Corporation, Deerfield, IL, USA), and average values of model parameters were calculated for each patient transport type (Table 1). Residual renal Kt/V was calculated for GFR values of 0 up to 15 mL/min/1.73 m2, and weekly total (peritoneal + residual) Kt/Vurea (Kt/VTotal) was calculated for patient total body water (TBW) values ranging from 30 to 60 L. Residual renal urea clearance rate (KR,urea) was calculated as 2/3 of GFR (19,20), and GFR was adjusted for patient body water using the Dubois-Dubois body surface area equation assuming an average patient height of 5’ 7” (170 cm). Total body water was assumed to be 55% of patient body weight. Adequacy of treatments based on urea clearance was assessed by Kt/VTotal being greater than or equal to 1.7. Daily ultrafiltration (UF) and sodium removal were calculated to complement adequacy assessment of single daily icodextrin exchanges.
Patient Characteristics
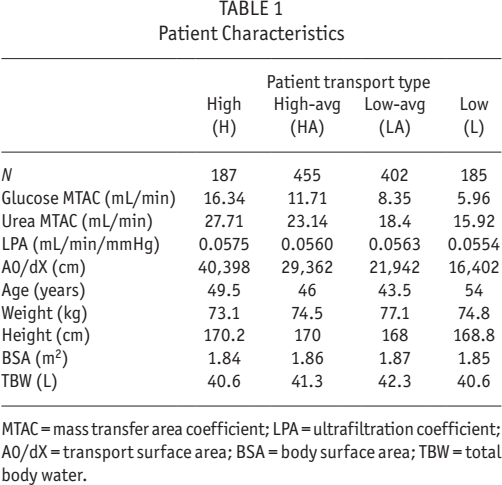
MTAC = mass transfer area coefficient; LPA = ultrafiltration coefficient; A0/dX = transport surface area; BSA = body surface area; TBW = total body water.
Results
Figure 1 illustrates the relationship between the intrinsic patient GFR and the weekly peritoneal Kt/V needed to achieve adequate urea clearance (Kt/VTotal = 1.7). Based on the assumed relationship between GFR and residual renal urea clearance rate (KR,urea = 2/3 GFR), a residual GFR value of 8 mL/min/1.73 m2 is predicted to provide the greater part of Kt/VTotal adequate for most patients. For example, a patient with TBW of 40 L (73 kg body weight) and GFR of 8 mL/ min/1.73 m2 is expected to require a weekly peritoneal Kt/V of only 0.4 to achieve adequate urea clearance. A GFR of 12 mL/min/1.73 m2 is predicted to provide adequate Kt/VTotal for all patients except very large ones (TBW > 60 L).
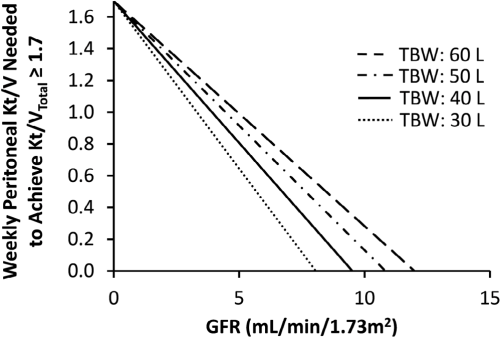
The relationship between renal glomerular filtration rate and supplemental dialysis dose needed to achieve a weekly total (peritoneal + residual kidney) Kt/V of ≥ 1.7. TBW = total body water; GFR = glomerular filtration rate.
Weekly peritoneal Kt/V delivered by single daily icodextrin exchanges of 2 and 2.5 L of solution volume is illustrated in Figure 2 and Table 2. After long icodextrin dwells, urea is predicted to be close to equilibrium between the blood and the dialysate compartments, relatively independent of patient transport type; thus urea clearance is expected to be proportional to the prescribed solution volume. Conversely, weekly peritoneal Kt/V is a strong function of patient size, ranging between 0.25 and 0.71 for TBW of 30 to 60 L, respectively. All but the very largest patients (TBW > 60 L) with a GFR of 10 mL/min/1.73 m2 are predicted to achieve adequate Kt/VTotal when they perform a single daily icodextrin exchange of minimum 8 hours with 2 L or 2.5 L solution volume, irrespective of their transport type or body size (Table 3). For a 40-L (73-kg) patient, a GFR of 8 mL/min/1.73 m2 is predicted to provide adequate Kt/V when a single daily icodextrin regimen is used, while a GFR as low as 6 mL/min/1.73 m2 used in conjunction with a single daily icodextrin exchange may suffice for smaller patients (TBW ≤ 30 L).
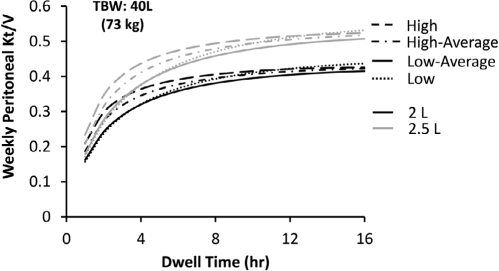
Weekly peritoneal Kt/V delivered by single daily icodextrin dwells with 2- and 2.5-L bag volumes to patients of different transport types with total body water of 40 L. TBW = total body water.
Weekly Peritoneal Kt/V Provided by Single Daily Icodextrin Dwells
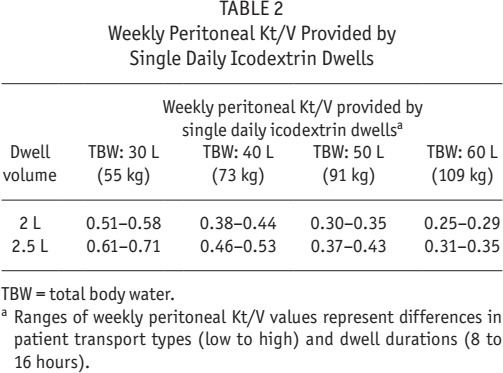
TBW = total body water.
Ranges of weekly peritoneal Kt/V values represent differences in patient transport types (low to high) and dwell durations (8 to 16 hours).
Residual GFR Needed to Achieve Adequate Kt/VTotal for Single Daily Icodextrin Therapy
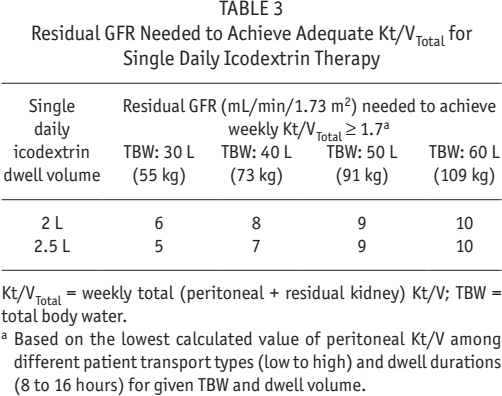
Kt/VTotal = weekly total (peritoneal + residual kidney) Kt/V; TBW = total body water.
Based on the lowest calculated value of peritoneal Kt/V among different patient transport types (low to high) and dwell durations (8 to 16 hours) for given TBW and dwell volume.
Figures 3 and 4 and Table 4 show UF and sodium removal for single icodextrin exchanges of 8 to 16 hours. In this analysis, solution volumes of 2 and 2.5 L were used for patients of all transport types. Both UF and sodium removal are predicted to increase with dwell time except for high transporters with longer dwell times (i.e., 12 to 16 h). Overall, a single daily icodextrin exchange of 8 to 16 hours is predicted to provide daily UF and sodium removal in ranges of 359 to 607 mL, and 52 to 87 mEq, respectively.
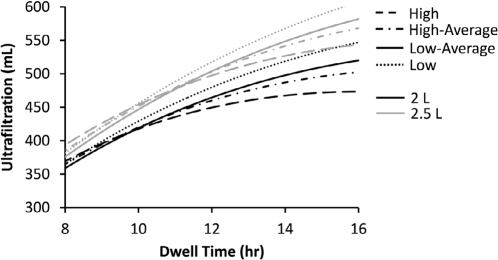
Daily ultrafiltration volume achieved with single daily icodextrin dwells of 2- and 2.5-L bag volumes for different patient transport types (low to high).
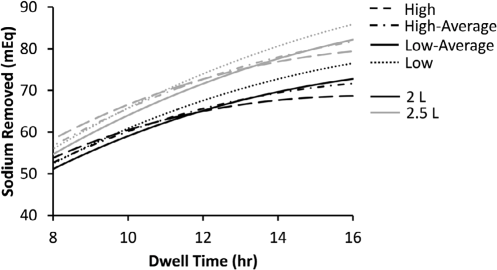
Sodium removal achieved with single daily icodextrin dwells of 2- and 2.5-L bag volumes for different patient transport types (low to high).
Range of Ultrafiltration Volume and Sodium Removal During 8- to 16-Hour Single Icodextrin Dwells Across Patient Transport Types
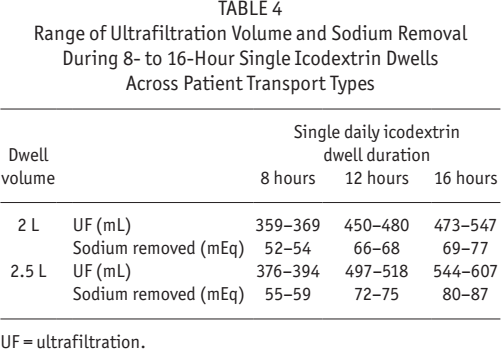
UF = ultrafiltration.
Discussion
Incremental dialysis is not a new concept, but rather has been used as a prescriptive method of initiating dialysis since the 1990s, if not before (21–24). Incremental dialysis is not intended as a means to start patients with failing renal excretory function on dialysis at an earlier time; rather, it is a means to supplement failing kidney function, providing removal of residual waste and excess salt and water, in order to attenuate or resolve symptomatology related to uremia and volume overload. Most patients starting dialysis do so with some level of RRF (12,13). This is in keeping with recent published recommendations suggesting that dialysis be started when the GFR is < 15 mL/min/1.73 m2 and/or when the patient becomes symptomatic, but before GFR falls below 6 mL/min/1.73 m2 (25,26).
Published studies of incremental dialysis have suggested a positive impact on patient quality of life due to lesser burden of dialysis procedures, enabling a more gradual, palatable immersion to dialysis initiation (27,28). They have also demonstrated reduced peritonitis rates attributed to decreased manual connections and an extended peritoneal “dry period,” lower systemic and peritoneal glucose exposure (improved preservation of peritoneal membrane function and fewer metabolic alterations), and better preservation of RKF (22,27,29,30). These benefits have the potential of not only improving uptake of PD (27), but also enhancing both technique and patient survival. These benefits must be counter-balanced by the risk of under-dialysis, the need for closer monitoring of RKF, and the need to educate patients about the future need to increase dialysis dose as RKF declines (21,22).
Previously published data on use of incremental PD have primarily utilized glucose-containing solutions. The effectiveness of this approach is highly dependent upon the patient's membrane transport status and the duration of the dwell time. For many patients, this represents a significant limitation given development of osmotic equilibration between the dialysate and the blood over relatively short intervals. This might compromise both UF and solute removal for either daytime or nighttime treatment, potentially precluding the convenience of “incremental” continuous ambulatory PD nighttime exchanges altogether. Conversely, icodextrin is limited neither by membrane transport nor by extended dwell time, typically producing similar UF and solute removal irrespective of membrane transport type, and allowing dwell times of 8 to 16 hours (18,31). Application of a solitary exchange of icodextrin as the nidus of incremental PD might therefore not only simplify the initial PD prescription for incident patients with RRF and their providers, but might further lessen the procedural burden, as well as infectious and metabolic risks inherent to PD therapy. We therefore sought to understand whether a solitary exchange of icodextrin for incident patients with residual renal Kt/V with GFR values up to 15 mL/min/1.73 m2 might provide an easier means of providing incremental dialysis.
The long duration of icodextrin exchanges allows for complete or near complete equilibration of urea (and other solutes) across the peritoneal membrane. As such, urea clearance will be proportional to the prescribed solution volume, independent of peritoneal membrane transport status. Similarly, as would be anticipated, Kt/V is highly dependent upon patient size (i.e., V). We demonstrated that achieving adequate weekly total Kt/V (≥ 1.7) with a single daily icodextrin exchange is highly dependent upon residual GFR and patient size. Nonetheless, most patients with a GFR of 10 mL/min/1.73 m2 are predicted to achieve adequate urea removal with a single daily 8-hour icodextrin exchange. Smaller patients would achieve adequate urea removal with lower levels of RKF. The latter findings may suggest that this practice may have its greatest applicability in areas of the world where greater numbers of patients exhibit a smaller body habitus. Duration of icodextrin exchange and the solution volume were shown to be determinants of peritoneal sodium removal and UF, allowing the treatment to be customized to augment sodium and volume removal in patients with RKF.
These results demonstrate that patients with significant RKF at the start of dialysis may be able to successfully achieve small uremic solute, volume, and sodium removal with a solitary long dwell exchange of icodextrin, either done during the day or, more conveniently, at nighttime. Incremental dialysis using icodextrin rather than dextrose-based solutions offers significant advantages. Use of dextrose-based solutions would not only require more frequent exchanges for comparable patients, impacting patient burden, the number of daily connections, and touch-contamination risk, but also increase both systemic and peritoneal exposure to glucose (32).
Patient transport parameters used in this simulation study were determined from PETs performed on 1,229 patients in the United States and Canada, which allows for the assessment of urea Kt/V, UF, and sodium removal for different patient transport types. Nevertheless, the outcomes of this study depend on the accuracy and extrapolability of estimated patient parameters to fluid and solute kinetics during icodextrin exchanges, and to populations outside of the United States and Canada. Furthermore, assessment of total weekly urea Kt/V is dependent upon the assumed relationship between urea clearance and GFR (KR,urea = 2/3 GFR). Due to these limitations, validation of this simulation study in future clinical trials is warranted.
A solitary daily nocturnal icodextrin exchange may be a more palatable means for patients to transition to life requiring RRT, lessening the procedural burden of care. Incremental PD using icodextrin rather than dextrose-based solutions can also attenuate systemic and peritoneal glucose exposure. One might conjecture that a once daily exchange using icodextrin offers the potential to reduce the risk of touch contamination and peritonitis more than what has been shown with incremental PD using 2 to 3 dextrose-based solutions, due to fewer manual connections and possibilities for contamination of the sterile fluid path. Given that the occurrence of peritonitis early in the course of PD therapy is associated with a higher risk of technique failure, the impact of incremental PD with using a once per day exchange, might impact technique survival (33,34).
Published clinical experiences with incremental PD utilizing a solitary exchange of icodextrin are limited, though results support some of the above contentions. In 2002, Foggensteiner et al. (24) described a non-randomized prospective trial, initiating dialysis with a single daily exchange of icodextrin, incrementally increasing the dialysis prescription to meet adequacy requirements as kidney function declined. The final results of their study demonstrated that incremental PD using a solitary exchange was acceptable to patients and could be implemented with minimal problems, including low bacterial peritonitis rates. However, icodextrin used as the solitary exchange in the first 24 subjects of this 39-patient study resulted in a high incidence of sterile peritonitis. Clusters of sterile peritonitis cases associated with Extraneal (Baxter Healthcare Corporation, Deerfield, IL, USA) usage in PD at that time, and again in 2007, were shown to be related to the presence of peptidoglycan (PG) in the solution. Peptidoglycan is a bacteria cell wall component known to elicit an interleukin (IL)-6 response in peripheral blood mononuclear cells (35). Implementation of exclusive icodextrin raw material sourcing (from Liverpool only), process improvements in icodextrin manufacturing, and employment of high-sensitivity PG testing of both raw material and Extraneal finished product has improved the quality of the product, attenuating the risk of PG-induced peritonitis. In 2013, Jeloka et al. (36) described their 5-year, single-center experience using a nocturnal exchange of “Ico-Alone” to initiate PD in 13 patients with a mean of 7.8 ± 2.6 mL/min of RRF (eGFR). Results were compared with a cohort of 28 patients with similar baseline characteristics started on conventional PD. Median period on “Ico-alone” was 9.6 months in this study. While selection bias may have played a role in the outcomes seen, peritonitis rates demonstrated an encouraging trend, though not reaching statistical significance (1 in 56.22 patient-months in the “Ico-alone” arm vs 25.29 in the conventional arm). Conversely, patient survival in the icodextrin-only arm was 42.84 months vs 25.29 months in conventional dialysis (p = 0.01), a finding that might suggest either therapeutic benefit of initiating PD with a solitary exchange of icodextrin or unmeasured confounding. Adequacy parameters were similar between the groups. No episodes of aseptic peritonitis were noted.
Conclusions
Most patients starting RRT in the US and the UK, and probably elsewhere around world, do so with > 8.6 mL/min/1.73 m2 of RKF. Our analysis using 3-pore kinetic modeling suggests that incremental dialysis using a solitary daily exchange of icodextrin can provide adequate small uremic solute, sodium, and volume removal for the majority of these patients. A solitary icodextrin exchange may be reasonable initial therapy for most incident ESRD patients. The impact of this novel prescriptive intervention on attenuating the burden of disease, maintaining the peritoneal membrane, slowing the decline of RKF, reducing infection related to touch contamination, and attenuating payer economic burden needs to be evaluated in clinical trials.
Footnotes
Acknowledgments
All funds for this work were provided by Baxter Healthcare Corporation. This study was presented as a poster at American Society of Nephrology, Kidney Week 2016, Chicago, Illinois. We thank Dr. John K. Leypoldt for his valuable advice on the kinetic modeling methods used in this study. We thank Dr. Kamyar Kalantar-Zadeh for his careful review of this manuscript and his insightful comments.
We have read and understood Peritoneal Dialysis International's policy on conflicts of interest disclosure and declare the following interests: BUA and JAS are employees of Baxter Healthcare Corporation with ownership interests.