
Abstract
We have previously reported successful induction of transient mixed chimerism and long-term acceptance of renal allografts in MHC mismatched nonhuman primates. In this study, we attempted to extend this tolerance induction approach to islet allografts. A total of eight recipients underwent MHC mismatched combined islet and bone marrow (BM) transplantation after induction of diabetes by streptozotocin. Three recipients were treated after a nonmyeloablative conditioning regimen that included low-dose total body and thymic irradiation, horse Atgam (ATG), six doses of anti-CD154 monoclonal antibody (mAb), and a 1-month course of cyclosporine (CyA) (Islet A). In Islet B, anti-CD8 mAb was administered in place of CyA. In Islet C, two recipients were treated with Islet B, but without ATG. The results were compared with previously reported results of eight cynomolgus monkeys that received combined kidney and BM transplantation (Kidney A) following the same conditioning regimen used in Islet A. The majority of kidney/BM recipients achieved long-term renal allograft survival after induction of transient chimerism. However, prolonged islet survival was not achieved in similarly conditioned islet/BM recipients (Islet A), despite induction of comparable levels of chimerism. In order to rule out islet allograft loss due to CyA toxicity, three recipients were treated with anti-CD8 mAb in place of CyA. Although these recipients developed significantly superior mixed chimerism and more prolonged islet allograft survival (61, 103, and 113 days), islet function was lost soon after the disappearance of chimerism. In Islet C recipients, neither prolonged chimerism nor islet survival was observed (30 and 40 days). Significant improvement of mixed chimerism induction and islet allograft survival were achieved with a CyA-free regimen that included anti-CD8 mAb. However, unlike the kidney allograft, islet allograft tolerance was not induced with transient chimerism. Induction of more durable mixed chimerism may be necessary for induction of islet allograft tolerance.
Introduction
The recent development of a potent induction immunotherapy protocol by a group of researchers in Minnesota, using a T-cell depleting antibody and tumor necrosis-α (TNF-α) inhibition, significantly improved short-term results of pancreatic islet transplantation (PITx) (1). However, 5-year graft survival was still only 50%, which is significantly lower than the survival rate for solid organ transplants. In addition to alloimmunity, multiple factors, such as exhaustion (20) and autoimmunity (23), may be involved in the loss of the islet allograft, but islet injury by chronic calcineurin inhibitor (CNI) use may also play an important role (2). Therefore, induction of tolerance of the islet allograft remains a desirable solution for improving long-term results of PITx (1,15,18).
We have previously reported a nonmyeloablative conditioning regimen that can induce mixed hematopoietic chimerism and renal allograft tolerance in nonhuman primates (NHPs) (4,7,10). This approach has been successfully translated to both human leukocyte antigen (HLA)-matched and HLA-mismatched human kidney transplant recipients with the longest immunosuppression-free survival of the latter group now exceeding 13 years (5,8,9). In the current study, we attempted to extend this mixed chimerism approach to islet transplantation in NHPs.
Materials and Methods
Animals
A total of 32 male cynomolgus monkeys weighing 3–5 kg were used (Charles River Primates, Wilmington, MA, USA). Recipient and donor pairs were selected for compatible ABO blood types and mismatched cynomolgus leukocyte (CyLA) major histocompatibility complex (MHC) antigens. CyLA class I antigenic disparity was determined by serologic typing with allele-specific anti-HLA class I monoclonal antibodies (mAbs) (H38, One Lambda; Thermo Fisher Scientific, Canoga Park, CA, USA) that cross-react with cynomolgus alleles. CyLA class II antigenic disparity was confirmed by a positive mixed lymphocyte response and polymerase chain reaction assay using primers specific to cynomolgus D-related (DR) as previously described (10). All surgical procedures and postoperative care of animals were performed in accordance with National Institute of Health guidelines for the care and use of primates and were approved by the Massachusetts General Hospital Institutional Animal Care and Use Committee.
Mixed Lymphocyte Reaction
An equal number of responding and irradiated (3,000 cGy) stimulating peripheral blood mononuclear cells (PBMCs) were cocultured for 4 days in medium containing RPMI-1640 (Mediatech, Inc., Manassas, VA, USA) and 10% monkey plasma. Negative controls included autologous PBMCs and irradiated cells cultured in medium alone. During the last 24 h, the plates were pulsed with 1 μCi/well [3H]thymidine (DuPont, Boston, MA, USA), and its uptake was quantitated in a β counter (PerkinElmer, Waltham, MA, USA). Results were expressed as stimulation index (SI) ratios, which were mean cpm of experimental/autologous stimulators.
PCR-Southern Blot
DNA extraction from whole blood was performed using a Qiagen blood kit (Qiagen, Valencia, CA, USA). PCR was performed using the following nine primer pairs to cynomolgus DRB: I) CGTTTCTTGGAGCAGGTTAAGTT and TGCACACTTTGTCCACCTC, II) CGTTTCTTGG AGTACTCTACA and CACCGAGGCCCGCTGGTCT, III) GTTTCTTGGAGCAGGTTAAACA and GTCTGC AGTAGGTGTCCACTG, IV) TTCTTGTGTCAGTTTA AGTT and GTCCACCGCGGTCCTCGC, V) TTCTT GGAGCAGGTTAAACA and GTCCACCCGGGCCC GCCT, VI) GTACTCTACATCTGAGTGTCAC and TC TGCAGTATTTGTCCACCCG, VII) TTCTTGAAGCA GACTAAGGC and CCCGCGTCCGCTCCAGGTA, VIII) TTCTTGGAGCAGGCTAAGTC and GTCCCGCTTCT CCTCCAGGATGC, IX) TTCTTGGAGCAGGCTAAA CG and GGTGTCCACCGCGGCCCGA.
Amplification was carried out in the GeneAmp PCR System 9600 (PerkinElmer). Evaluation of PCR reactions was performed by traditional agarose electrophoresis and staining with ethidium bromide. Southern blotting was used to further increase the sensitivity of the assay. The blot was hybridized with a biotinylated probe utilizing a chemiluminescent system for detection (Tropix, Bedford, MA, USA).
Conditioning Regimens
Islet A
The original conditioning regimen for combined kidney and bone marrow transplantation (CKBMT) was initially used for the combined islet and bone marrow transplantation (CIBMT) recipients. The regimen consisted of nonmyeloablative total body irradiation (TBI; 1.5 Gy × 2) on days –6 and –5 (relative to the CIBMT), thymic irradiation (TI; 7 Gy) on day –1, horse Atgam (ATG; 50 mg/kg/day on days –2, –1, and 0; Pharmacia and Upjohn, Kalamazoo, MI, USA), and anti-CD154 monoclonal antibody (aCD154 mAb; 20 mg/kg on days 0 and +2, and 10 mg/kg on days +5, +7, +9, and +12; American Type Culture Collection, Manassas, VA, USA). The recipients underwent CIBMT on day 0 and were treated with a 1-month course of intramuscularly administered cyclosporine (CyA; tapered from an initial dose of 15 mg/kg/day; Novartis, Basel, Switzerland) to maintain therapeutic serum levels (> 250 ng/ml). CyA was discontinued on day 27 posttransplant (Fig. 1 and Table 1), after which serum CyA levels typically became undetectable by day 60 (data not shown).

Standard regimen of CIBMT or CKBMT. The conditioning regimen for the Islet A group (n = 3) and Kidney A group (n = 8) included nonmyeloablative TBI (1.5 Gy × 2) on days –6 and –5, TI (7 Gy) on day –1, horse ATG (50 mg/kg/day on days –2, –1, and 0), and anti-CD154 monoclonal antibody (aCD154 mAb; 20 mg/kg on days 0 and +2, and 10 mg/kg on days +5, +7, +9, and +12). The recipients underwent CKBMT or CIBMT on day 0 and were treated with a 1-month course of CyA to maintain therapeutic serum levels (> 250 ng/ml). In the Islet B group (n = 3), CyA was replaced with anti-CD8 monoclonal antibody (aCD8 mAb) at 5 mg/kg on days –1, 0, and +2 and continued at 1 mg/kg weekly until day 28. The Islet C group (n = 2) was subjected to the same regimen as the Islet B group, except ATG was removed.
Conditioning Regimens in All CIBMT and CKBMT Monkeys

BM, bone marrow; TBI, total body irradiation; TI, thymic irradiation; ATG, Atgam; CyA, cyclosporine.
Islet B
CyA was replaced with anti-CD8 mAb (cM-T807 provided by Centocor Inc., Horsham, PA, USA) at 5 mg/kg on days –1, 0, and +2 and continued at 1 mg/kg weekly until day 28 (Fig. 1 and Table 1).
Islet C
ATG was removed from the Islet B regimen (Fig. 1 and Table 1).
Kidney A
The results in Islet A, Islet B, and Islet C recipients were compared with historical observations in CKBMT recipients summarized here as Kidney A. The conditioning regimen used for the CKBMT group was exactly the same as that administered for the Islet A group (Fig. 1 and Table 1).
Induction and Management Diabetes
One week before transplantation, diabetes was induced with an intravenous injection of streptozotocin (STZ; Sigma-Aldrich, St. Louis, MO, USA) at a dose of 55 mg/kg (12). Blood glucose (BG) levels were then monitored two times per day, and the diabetic monkeys were treated with neutral protamine hagedorn (NPH; Eli Lilly Co., Indianapolis, IN, USA) and regular insulin (Humalin N and R; Eli Lilly) to maintain blood glucose levels of 80–300 mg/dl.
Isolation of Donor Pancreatic Islets
Our method for islet isolation was reported in detail previously (17). Briefly, after being perfused with Viaspan (Bristol-Myers Squibb, New York, NY, USA), the pancreas was digested with Liberase HI (Roche, Indianapolis, IN, USA). The digested tissue was applied to a discontinuous gradient with Ficoll (Sigma-Aldrich) at a ratio of 1:11 (tissue/Ficoll). Islets were then collected from the two interfaces, washed, and counted for transplantation.
PITx
Under general anesthesia, a small midline celiotomy was made, and a 22-gauge × 0.75-inch catheter was inserted into the inferior mesenteric vein. Alloislets were suspended in 10 ml of normal saline with 100 U/kg heparin (Hospira, Inc., Lake Forest, IL, USA) (Table 2) and infused into the portal circulation through the venous cannula.
Clinical Features of CIBMT and CKMBT Recipients

Kidney Transplantation (KTx)
Donor
Through a midline incision, the abdomen was explored to ensure the presence of two normal-appearing kidneys. The left kidney was then exposed, incising the retroperitoneal attachments. The renal vein was then cleared right down to the vena cava. The renal artery was isolated by ligating and dividing the adrenal artery. The ureter was freed up, carefully sparing the vascular supply. The ureter was then divided, and the distal ureter was ligated. A small Satinsky clamp was then placed on the aorta. The kidney was perfused with approximately 6–8 cc of cold Ringer's lactate solution (Baxter Healthcare Corporation, Deerfield, IL, USA) containing mannitol (1.25 g/500 cc; Hospira). The renal vein was divided first; then the renal artery was taken with a small patch of donor aorta. The kidney was immediately placed in a Petri dish containing cold Ringer's lactate solution.
Recipient
The incision in the recipient was midline, but extended down to the symphysis pubis. Exposure of the aorta and vena cava was just above the bifurcation of these great vessels. Approximately 3–4 cm of the distal aorta and vena cava were cleared. When the donor kidney was available, the recipient aorta and vena cava were cross-clamped together using a single Satinsky clamp. The donor kidney was then brought into the field, and an end-to-side anastomosis between donor renal vein and recipient cava was performed using 8-0 Prolene (Ethicon, LLC, Somerville, NJ, USA). The arterial anastomosis between donor and recipient aorta was completed using 7-0 Prolene (Ethicon). The renal vessels were temporarily occluded with small forceps while the Satinsky clamp was removed. After the aorta had perfused for a few seconds, the renal artery was released, allowing perfusion of the kidney. When hemostasis (3–5 min) had been assured, the kidney was held in place using the previously placed stay sutures, which were sutured to the retroperitoneum. At this point, bilateral kidneys were removed.
The bladder was then opened by dividing the serosa and musculature over a centimeter length, taking care not to open the mucosa. A 3-mm-diameter stoma was made in the most distal mucosa. The bladder mucosa-to-mucosa anastomosis was then completed using 7-0 chromic gut (Ethicon). Finally, the bladder musculature was closed over the ureter using 5-0 Vycril (Ethicon). The abdomen was washed out with warm saline and then closed.
Donor Bone Marrow Transplantation (DBMT)
Bone marrow cells were obtained by processing the vertebral bodies after cardiac arrest. The marrow was filtered through a nylon mesh, red cells lysed with ammonium chloride solution (ACK; Thermo Fisher Scientific, Grand Island, NY, USA), and the preparation washed with Hank's balanced salt solution (HBSS; Thermo Fisher Scientific). The cells were then transfused into the recipient. A total of 3 × 108/kg of mononuclear cells processed from the bone marrow were administered intravenously.
Detection of Chimerism
After standard water shock treatment, peripheral blood cells were first stained with donor-specific mAbs chosen from a panel of mouse anti-human HLA class I mAbs that cross-react with cynomolgus monkeys. Cells were incubated for 30 min at 4°C and then washed twice. Cell-bound mAb was detected with fluorescein isothiothianate (FITC)-conjugated rat anti-mouse immunoglobulin IgG2a mAb (BD Pharmingen, San Diego, CA, USA), which was incubated for 30 min at 4°C, followed by two washes and analysis on FACScan (Becton Dickinson, Franklin Lakes, NJ, USA). In all experiments, the percentage of cells that stained with each mAb was determined from one color fluorescence histogram and compared with those obtained from donor and pretreatment frozen recipient cells, which were used as positive and negative controls. The percentage of cells considered positive was determined with a cutoff chosen as the fluorescence level at the beginning of the positive peak for the positive control stain and by subtracting the percentage of cells stained with an isotype control. By using forward and 90° light scatter (FSC and SSC, respectively) dot plots, lymphocyte (FSC- and SSC-low), granulocyte (SSC-high), and monocyte (FSC-high but SSC-low) populations were gated, and chimerism was determined separately for each population. Nonviable cells were excluded by propidium iodide (Thermo Fisher Scientific) staining.
Cytokine Measurement
Serum interleukin-1β (IL-1β), TNF-α, IL-6, IL-17, IL-12 (P40), and IL-10 levels at 1 week (CIBMT, n = 7; CKBMT, n = 3) and 4 weeks (CIBMT, n = 8; CKBMT, n = 7) after transplantation were determined by Luminex (Life Technologies, Carlsbad, CA, USA) using NHP cytokine PRCYTOMAG-40K (Merck Millipore, Billerica, MA, USA), following the manufacturer's instructions.
Statistical Analysis
All values are represented as mean ± standard deviation (SD). An intergroup statistical analysis was performed using Student's t-test or Welch's t-test. For chimerism, an intergroup (Islet A, Islet B, and Kidney A) statistical analysis was performed using the Bonferroni correction test. The differences were considered statistically significant with a value of p < 0.05. Graft survival was analyzed by Prism 4 (Graph Pad Software Inc., La Jolla, CA, USA).
Results
A Conditioning Regimen That Reliably Induced Mixed Chimerism and Renal Allograft Tolerance Failed to Induce Long-Term Islet Allograft Survival
Three monkeys (M4399, M2100, and M6201) were treated with the Islet A regimen, which reliably induced renal allograft tolerance in most CKBMT recipients (Kidney A) (Fig. 1 and Table 1). An average of approximately 50,000 islet equivalents (IEQs) of islets were isolated from a cynomolgus monkey pancreas with purity and viability typically exceeding 90%, as detailed in Table 2. The final islet preparation had a mean insulin and DNA content of approximately 400 and 900 μg, respectively (17). A separate study has shown that islet allograft survival was 4–5 days without any immunosuppressive treatment (13). With this regimen, all three Islet A recipients developed comparable levels of multilineage chimerism (Fig. 2). All recipients received a sufficient number of islets (> 11,000 IEQ/kg) with high purity and viability and transiently became insulin independent posttransplantation as shown in Figure 3A. Nevertheless, all recipients in this group exhibited unstable islet function and failed to achieve long-term islet allograft survival (18, 51, and 55 days, p = 0.0004 in Kidney A vs. Islet A) (Fig. 4).
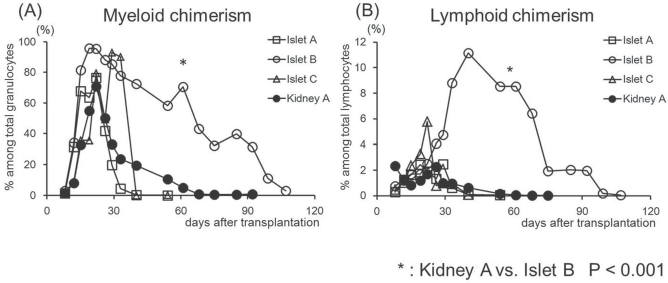
Multilineage mixed hematopoietic chimerism after CIBMT and CKBMT. Mean values of chimerism (%) detected in both myeloid (A) and lymphoid (B) lineages in Islets A, B, and C and Kidney A recipients. In Islet B, recipients developed significantly higher and longer duration multilineage chimerism than observed in the other groups (*p < 0.05).

Clinical courses after CIBMT. Solid lines represent serum glucose levels. Gray bars indicate insulin requirements (IU: international unit) per day. Black bars indicate the duration of CyA therapy. X indicates severe hypoglycemic episode within 72 h after islet transplantation.

Kidney and islet allograft survival. The kidney allograft survival was significantly longer than any islet allograft survival (p < 0.05). Islet allograft survival in Islet B was significantly longer than that in Islet A (p < 0.05).
A CyA-Free Regimen with Anti-CD8 mAb Significantly Improved Chimerism Induction and Prolonged Islet Allograft Survival
Since the loss of islet function may be attributed to CyA toxicity of the islet allograft, we tested a CyA-free regimen in three recipients. Since our previous studies showed improved chimerism induction with more aggressive CD8+ memory T-cell (TMEM) deletion (14), anti-CD8 mAb was added to the Kidney A regimen in place of CyA (Islet B). With this regimen, the levels and duration of chimerism were significantly improved in both lymphoid and myeloid lineages (Fig. 2). Islet allograft survival was also more stable and prolonged (p = 0.02) compared with the Islet A group (Fig. 4). However, these recipients eventually lost islet allograft function due to rejection by day 113 (Figs. 3B and 5A, B), and allograft tolerance was not achieved. In the Islet C group, in an attempt to develop a less invasive protocol, ATG was also removed from the Islet B regimen (Islet C). The level of chimerism induced with this regimen was comparable with those observed in Islet A (Fig. 2), but both recipients lost islet allograft function soon after discontinuation of immunosuppressive injection (Figs. 3C and 4).
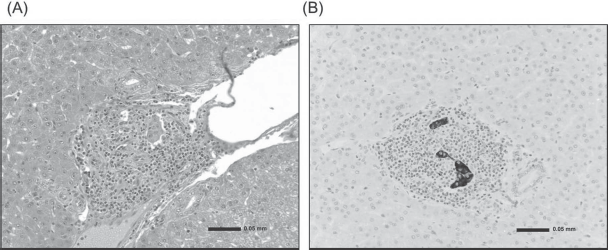
Histopathology of islet allograft. (A) The Islet allograft in the liver (day 113). The liver was examined at autopsy. There was marked mononuclear cell infiltration in the islet allograft transplanted in the liver. (B) Insulin staining of islets (day 113). There was limited islet tissue remaining at the transplant site.
Serum Cytokine Levels in Islet and Kidney Allograft Recipients
Our previous studies on induction of renal allograft tolerance demonstrated that higher inflammatory responses prevented allograft tolerance induction (24). Thus, we postulated that failure of tolerance induction in islet transplantation could have been the result of higher inflammatory responses in the CIBMT recipients. Therefore, we assessed various serum cytokine levels measured following CIBMT versus CKBMT. Significantly higher IL-6 levels (p < 0.05) were observed at 1 week after KTx, compared with those observed in islet transplantation. On the other hand, TNF-α and IL-17 levels tended to be higher, but not statistically significant in islet allograft recipients at 1 week. No significant difference was observed in any cytokines at 4 weeks after transplantation (Fig. 6).

Inflammatory cytokine levels and IL-10 in the sera. Black and white columns represent the serum cytokine levels in recipients of the islet allograft (CIBMT) and the kidney allograft (CKBMT), respectively, at 1 week and 4 weeks after transplantation. IL-6 level was significantly higher in recipients of the kidney allograft than those of islets at 1 week after transplantation (A). Although statistically not significant, TNF-α and IL-17 tended to be higher in islet recipients than those in kidney recipients at 1 week after transplantation (B, C), and IL-10 was higher in the CKBMT group at 4 weeks (not significant) (D).
Discussion
We have previously reported long-term renal allograft survival without ongoing immunosuppression administered in MHC-mismatched NHP recipients of CKBMT after treatment with a nonmyeloablative conditioning regimen (4,7,10). This approach has been successfully translated to HLA-mismatched clinical kidney transplant recipients with the longest immunosuppression-free survival now exceeding 12 years (5,8,9). In the NHP recipients, peripheral blood chimerism typically became undetectable by 30 to 60 days after transplantation except for chimerism observed in the Islet B regimen, which lasted longer than 100 days after DBMT (Fig. 2). Nevertheless, long-term survival of renal allografts was achieved without the need for chronic immunosuppression. In contrast to the renal allograft, our previous studies demonstrated that induction of heart allograft tolerance was not achievable after induction of transient chimerism (6). However, we recently observed that lung allograft tolerance is inducible even with transient chimerism (22). Therefore, tolerance induction via our approach with transient chimerism appears to be organ/tissue specific with kidney and lung allografts possibly having some mechanisms in common that maintain allograft tolerance after disappearance of chimerism. In a previous study, as an initial attempt to extend our approach, cellular transplantation was performed in a recipient already tolerant of a renal allograft. Two years after the CKBMT and withdrawal of immunosuppression, diabetes was induced with STZ and islets harvested from the original kidney/BM donor were transplanted into the portal circulation and beneath the kidney capsule (11). Euglycemia was achieved without additional immunosuppression. Although the recipient became diabetic 300 days after islet transplantation, viable transplanted islets were found in the liver and under the kidney capsule without any evidence of rejection. This study suggested that islet allograft tolerance could be achieved at least in a recipient already tolerant of a kidney allograft.
In the current study, we investigated whether tolerance of isolated islets, without the presence of a kidney allograft, could be similarly induced via the transient chimerism approach. Following conditioning with the same therapeutic regimen that consistently induces renal allograft tolerance, all three CIBMT recipients treated with the Islet A regimen developed comparable levels of hematopoietic chimerism to those observed after CKBMT (Kidney A). However, none of the CIBMT recipients achieved prolonged islet allograft survival. One potential control for this group (Islet A) would have been the use of autografts to rule out islet loss due to nonimmunological causes, such as the toxicity of the conditioning regimen or nonspecific inflammatory responses. However, this control is practically difficult to perform, as a recipient has to tolerate a strenuous conditioning regimen immediately after near total pancreatectomy. Therefore, to rule out the possibility of islet toxicity by CNI, rather than rejection, as the cause for these failures, we developed a CNI-free conditioning regimen by substituting anti-CD8 mAb for CyA used in the first three recipients. The rational for utilizing anti-CD8 mAb was based on our previous observations that more effective CD8+ TMEM depletion resulted in improved chimerism induction (14,24). As we expected, all anti-CD8 mAb-treated recipients developed significantly higher levels of multilineage chimerism than that observed after Islet A with CyA. A similar improvement of chimerism was not observed without ATG (Islet C), indicating that some intervention on CD4+ T cells by ATG may also be important for chimerism induction. Although the anti-CD8 mAb-treated recipients did achieve significantly longer allograft survival, tolerance was not induced with resumption of insulin administration being required in all recipients after several months.
The explanation for the contrasting results between CIBMT and CKBMT could be largely attributed to alloimmunity, but the graft loss due to CNI toxicity and nonspecific inflammatory responses should also be taken into consideration. For example, insulin requirements after transplantation were higher in Islet A than in CNI-free regimens (Islet B and Islet C), suggesting that the toxicity of CNI on islet allografts is indeed concerning in posttransplant islet function. On the other hand, two (M2100 and M1402) recipients experienced undetectable hypoglycemia within 72 h after CIBMT (Fig. 3, marked with X), which may indicate some islets of these recipients were destroyed by an instant blood-mediated inflammatory reaction (IBMIR) (16,25). Interestingly, recipients of the kidney allograft did not lose their allograft function despite significantly higher serum IL-6 levels (Fig. 6), indicating that the kidney allograft may be able to tolerate inflammatory responses more than the islets (3,19).
The loss of islet function in three recipients in the Islet B group may be attributable to the antidonor alloimmune response. As observed in our previous study with isolated heart allografts, islet allografts were rejected after the loss of chimerism. These results may indicate that additional mechanisms may be necessary to maintain tolerance after the loss of chimerism in islet or heart transplantation. In our most recent study, we found that stable heart allograft tolerance can be induced even with transient chimerism if a renal allograft from the same donor is simultaneously transplanted. The removal of the kidney allograft at 1 year after cotransplantation resulted in immediate rejection of the heart allograft, indicating a critical role of the kidney allograft in maintenance of tolerance after the loss of chimerism (21). Therefore, cotransplantation of a kidney allograft with islet transplantation may be an attractive strategy. Unlike heart transplantation, kidney and islet cotransplantation is more clinically applicable.
In conclusion, significant improvement of mixed chimerism induction and islet allograft survival were achieved without CyA by addition of anti-CD8 mAb. However, unlike the kidney allograft, islet allograft tolerance was not induced with transient chimerism. Induction of more durable mixed chimerism may be necessary for induction of islet allograft tolerance.
Footnotes
Acknowledgments
This work was supported in part by POI-HL18646, ROI A137692-05, U19 AI102405-01, National Institute of Allergy and Infectious Disease (NIAID). This manuscript was not prepared or funded by any commercial organization. The authors declare no conflicts of interest.