
Abstract
The purpose of this study was to investigate the clinical efficacy of neural stem/progenitor cell (NS/PC) transplantation to treat severe cortical visual impairment (CVI), a sequela of neonatal brain injury. Fifty-two patients with cerebral injury and CVI were randomly divided into two groups: the treatment group (n = 25, with the median age of 18 months) and the control group (n = 27, with the median age of 19.5 months). The treatment group received intracerebroventricular transplantation of human NS/PCs and rehabilitation training. The control group received rehabilitation only. The visual function was assessed by Holt's method at various time points after transplantation. One in five patients with fundus abnormalities accompanied by blindness regained light perception. The visual functions of 75% of the patients with normal fundus were improved by one level or more in a 2-year follow-up. The median efficacy appeared 60 days posttransplantation. The total effective rate of cell transplantation on visual improvement was 64% (16 patients of 25), among which one blind patient regained light perception, five (31.2%) CVI patients improved by one level, and 10 (62.5%) improved by more than one level. Functional magnetic resonance imaging (fMRI) in a subpopulation of patients showed enhanced signals in the occipital lobe, visual pathway, and apical lobe after transplantation. In the control group, four patients with fundus abnormalities showed no improvement. Nine of 23 CVI patients with normal fundus improved visual function by more than one level. At the 2-year follow-up, no blind patients showed visual improvement. The total effective rate was 33.33% (9 of 27 patients). Among those showing visual improvement in the control group, six patients (66.67%) improved by one level, and three (33.33%) by more than one level. The median efficacy occurred in 365 days. Human NS/PC transplantation is effective to treat patients with severe CVI after neonatal brain injury. Compared with the traditional rehabilitation training, cell transplantation showed not only earlier visual improvement but also higher improvement rates and degrees. This article is published as part of the International Association of Neurorestoratology (IANR) supplement issue of Cell Transplantation.
Introduction
Brain injury ranks number three in causing cortical visual impairments (CVIs) in children (13). The incidence rate of CVI is approximately 2.4% (16) and is increasing alongside the number of critically ill newborns and premature infants. A survey from several hospitals, communities, and statutory blind registries, performed by Flanagan et al., revealed a total of 76 children with visual impairment, accounting for 1.61± of the newborns. Of these children with visual problems, 45% had CVI (8). Light stimulation is the only therapy currently available for CVI, but with poor efficacy. Therefore, it is necessary to explore new and effective treatments.
Stem cell research brings new hope for treating refractory central nervous system diseases. Various types of stem/progenitor cells have been shown to improve functionalities to some extent in patients and animal models of stroke, traumatic brain injury, Parkinson's disease, and Huntington's disease (1,7,9,20,28,39,45). In May 2005, we successfully treated the first case of neonatal hypoxic-ischemic encephalopathy (HIE) by transplanting human neural stem/progenitor cells (NS/PCs) (31). Later, we continued our clinical research on NS/PC transplantation to treat neonatal brain-injured patients and its sequela—cerebral palsy (29,31,40). One of the cases suffered from cerebral palsy together with severe CVI and had only faint light perception but was unable to gaze at or track objects. Interestingly, 11 days after receiving NS/PC transplantation, the baby started to gaze at objects such as dogs, bicycles, and cars as well as track their movements (30). On the basis of this initial success, we expanded our clinical research and report herein the outcome of human NS/PC transplantation in children suffering from CVI.
Materials and Methods
Patient Selection
We used a random number table to carry out the grouping of the outpatient department of the Navy General Hospital from May 2005 to February 2009. Sixty patients were divided into two groups with 30 cases in each group. Eight cases withdrew after grouping. Thus, 52 CVI patients were recruited into the study in two groups: the treatment group (n = 25, 18 males and 7 females, age 4–72 months) and the control group (n = 27, 19 males and 8 females, age 5–68 months). There were no statistically significant differences between the two groups with regard to age, sex, causes of CVI, brain injury types, or fundus structural changes (Table 1). All cases completed follow-up.
Comparison Between the Treatment and the Control Groups

p Values were derived by chi-square or Fisher's exact test. PVL, periventricular leukomalacia.
The inclusion criteria for subjects were as follows: (a) patients from May 2005 to February 2009; (b) patients aged 3 months to 6 years; (c) all patients who had a history of brain injury during their perinatal period; and (d) according to visual functional grading, all patients who had severe visual dysfunction, including blind patients and level I and level II visual function patients.
Exclusion criteria were as follows: (a) brain injuries caused by other diseases such as progressive inherited metabolic disease; (b) severe congenital heart disease, cardiac functional insufficiency; (c) severe pulmonary disease, respiratory failure; (d) complications with acute or chronic infection; and (e) frequent epileptic seizures in the last 3 months.
Treatment Group
Visual Function. Three cases were completely blind. The visual functions of the other patients were assessed using the Hoyt's method (15). Fourteen with merely light perception but no eye gazing and tracking were scored as having a level I visual function. The other eight could gaze at large objects occasionally and were scored with a level II visual function.
Fundus Examination. Fundus changes were found in five patients, three of whom had slightly pale optic discs bilaterally. The fourth one had white discs with no light reflection in the macular center, and the fifth was a premature infant with retinopathy. The fundi of the other 20 cases were normal (Table 1).
Functional Magnetic Resonance Imaging (fMRI). Detecting brain functions in a blood-oxygen-level-dependent (BOLD) manner, fMRI can be used as a reference for the visual function of visual centers above the suprachiasm. fMRI exhibits two types of active signals: red and blue. The red (positive) fMRI signal produced by oxidized hemoglobin in the capillaries indicates a normal visual function. The deoxyhemoglobin-produced blue (negative) signal, on the other hand, indicates a relatively weak visual function. A lack of any active fMRI signals suggests the absence of visual function.
fMRI examinations (3THDX; GE Company, Wauwatosa, WI, USA) were conducted in nine cases. Seven did not show any BOLD signals, neither positive nor negative, in the visual cortex and the visual pathways. One case exhibited a low level of negative signals only in the occipital lobe but not in other regions. The last case had a low level of positive signals in the right occipital cortex and basal ganglia.
Control Group
Visual Function. Three patients were completely blind. Fourteen patients had light perception without gazing and visual tracking reactions, and their visual functions were scored at level I. The other 10 could gaze at large objects occasionally and thus were scored as level II.
Fundus Examination. Fundus changes were found in four patients, two of whom had slightly pale optic discs bilaterally. The third one had white discs with no light reflection in the macular center, and the fourth was a premature infant with retinopathy. The fundi of the other 23 cases were normal.
fMRI. fMRI examinations were carried out in five cases. Four did not show any BOLD signals (positive or negative) in the visual cortex and the visual pathways. One case exhibited a low level of negative signals only in the visual pathways.
A flowchart regarding participant selection is shown in Figure 1.
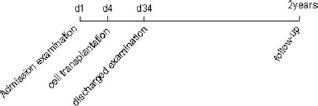
Flowchart of the trial. Magnetic resonance imaging (MRI), electroencephalography (EEG), cruor function, and immunofunction were included in the admission examination. MRI and EEG were included in the discharged examination. Visual function was determined during the follow-up period.
Routine Therapy
Before entering the clinical trial, the patients in both groups had already received light stimulation therapy and rehabilitative training for at least 3 months but had shown no visual improvements. The control group continued the light stimulus treatment for at least a further 6 months. Both groups continued physical therapy (PT) and occupational therapy (OT) throughout the trial.
Presurgical Procedure
The protocol of clinical studies was approved by the Scientific Council and Ethics Committee of the Navy General Hospital. The guardians of the patients in the treatment group were fully informed about the sources, separation, and cultivation of the cells; the methods of cell therapy; the risks of the surgery, possible adverse effects, and safety measures. The participant's guardian provided written informed consent for each participant. All treatment procedures were under the supervision of the Ethics Committee of the hospital. Before cell transplantation, coagulation and immune function tests were performed after peripheral blood was collected according to the routine protocols of the clinical laboratory of Navy General Hospital (Beijing, China).
Donor Selection
Fetus donors were selected from pregnant women who had requested artificial abortion during early pregnancy and consented to donate the fetus after being fully informed. Informed consent and agreement of voluntary donation was signed by all donors. Detailed family histories were obtained, and inherited metabolic, chromosomal, and infectious diseases were screened before donation. The protocols were approved by the hospital's Ethics Committee.
Cell Culture and Preparation
NS/PCs were isolated and cultured as previously described (29). Briefly, NS/PCs were isolated from an aborted human male fetal forebrain and resuspended in Dulbecco's modified Eagle's medium with F12 (DF12; Invitrogen, Carlsbad, CA, USA) supplemented with 1% N2 (Invitrogen), 2% B27 (Invitrogen), fibroblast growth factor-basic (20 ng/ml; PeproTech, Rocky Hill, NJ, USA), epidermal growth factor (20 ng/ml; PeproTech), leukemia inhibitory factor (4 μg/ml; PeproTech), and heparin (5 μg/ml; Sigma, St. Louis, MO, USA) and cultured under sterile conditions. Half of the medium was removed and replenished with fresh medium every 4 days. The cells were propagated for 2–3 weeks in vitro. Before transplantation, cells were strictly examined according to the technical guidelines for clinical research and quality control of human cells published by the State Food and Drug Administration (30,31,40). Cells were confirmed to be nestin positive by immunofluorescence staining using an anti-human nestin antibody (Millipore, Billerica, MA, USA). Cell viability was measured by trypan blue assay (Sigma), and the results showed a cell viability of over 95%. Cells have a normal karyotype and were microbe free. Endotoxin levels were less than 2 EU/ml in all cell populations.
Cell Transplantation
The patients were placed in a supine position and given general anesthesia before surgery. Under the guidance of color Doppler ultrasonography (AcusonSequia 512 Siemens; Acuson, Germany) with 4V1 probe and frequency of 2.0–4.0 MHz, 8 × 106–10 × 106 NS/PCs in normal saline [in the same volume as the outflow of cerebrospinal fluid (CSF)] were slowly injected into one of the lateral ventricles through the unclosed fontanel or through a hole drilled into the skull of patients with closed fontanels. The needle was slowly pulled out after the injection was finished, and the wound was sealed. Intraventricular cell transplantation was performed once for each patient.
Efficacy Evaluation of Transplantation
Each case received the visual function assessment 2 years after transplantation for the treatment group or enrollment for the control group.
Visual Function Evaluation
The visual function assessment based on Hoyt's method (below) (15) was co-performed by parents of the patients, ophthalmologists, and pediatricians.
Valid: The visual function improved at least by one level.
Invalid: The visual function had no changes in levels.
Regressive: The visual function decreased in levels.
Anopsia, amblyopia, and nystagmus were not included in the assessment of this clinical trial.
fMRI
The fMRI examination of the two groups was performed with informed consent when visual function showed changes.
Electroencephalogram (EEG)
EEG was performed using NicoletOne equipment (VIASYS Healthcare Inc., Chicago, IL, USA). Continuous EEG recordings, based on four electrodes and a reference electrode, were inspected at full length both in a two-electrode bipolar and a four-channel referential montage.
Statistical Analysis
Chi-square test or Fisher's exact test (unpaired) statistics were calculated using SPSS16.0 analysis software (IBM, Armonk, NY, USA). The data were represented as actual frequency. Differences between groups were considered statistically significant at p < 0.05.
Results
Visual Function (Table 2)
Treatment Group
One of the five patients with fundus abnormalities associated with blindness had light perception after transplantation. The visual functions of 15 of the remaining 20 patients with normal fundus were improved by at least one level. Among these 16 effective patients, six showed a rapid visual improvement at 5–13 days after transplantation. The other 10 exhibited a delayed improvement, five of which occurred at about 3 months, three around 6 months, and two between 6 and 12 months.
Visual Function Changes in the Treatment and the Control Groups

p values were derived by chi-square or Fisher's exact test.
A total of 22 patients completed the 2-year follow-up. One case improved from blindness to level I in visual function, three cases from level I to level II, four from level I to level III, one from level I to level I V, two from level II to level III, three from level II to level IV, and two from level II to level V. There was no retrogression in any of the patients. The total effective rate was 64% (16 of 25). Among the 16 effective cases, one with blindness obtained perception of light, five (31.25%) improved by one level, and 10 (62.5%) improved by two or more levels. The degree of improvement varied among the effective patients. Some children could gaze at big objects, small toy bricks, or glass beads and showed happiness when seeing their mothers or milk bottles. Others could recognize cards and distinguish different colors. Some could also track red balls, walking persons, or moving cars and liked to watch small pets.
Control Group
None of the four cases with fundus abnormalities (three with blindness) showed any improvement in visual function according to Hoyt's scale. Nine of the 24 cases with normal fundi showed various degrees of improvement. One case began to improve at 3 months, one at 6 months, three at 6–12 months, and four cases after a year.
Of the 27 control patients, 21 completed the 2-year follow-up. No blind patients improved to level I. Among the nine effective cases, two improved from level I to level II, one from level I to level III, four from level II to level III, one from level II to level IV, and one from level II to level V. No retrogression was found. The total effective rate is 33.33% (9 of 27). Among the effective cases, six (66.67%) obtained one level improvement in visual function and three (33.33%) improved by more than one level. The degree of improvement varied among patients. Some children could gaze at big objects occasionally; some gazed at small toy bricks or glass beads and distinguished small objects; still others tracked red balls and walking men and were able to name the objects.
fMRI
Treatment Group
Five cases with visual improvement received fMRI. In one patient, negative signals were detected in the front occipital lobe before treatment, with the right side significantly smaller than the left side (Fig. 2). After transplantation, in addition to the negative signals detected in bilateral occipital lobes, positive signals could also be identified in the right occipital lobe, the visual pathway, and the parietal lobe (Fig. 3). In another case, some negative signals were revealed in bilateral occipital lobes before treatment (Fig. 4), whereas positive signals could be detected in the right frontal lobe and the right occipitoparietal cortex after transplantation (Fig. 5). Furthermore, various degrees of positive and negative signals could also be detected in the other three cases after transplantation.

fMRI of case 1 before transplantation. Negative signals (blue) are detected in bilateral occipital lobes (visual cortices). The area of the signals on the right side is smaller than that on the left.

fMRI of case 1 after transplantation. In addition to negative signals (blue) in bilateral occipital lobes (visual cortices), positive (red) signals are now shown in the right occipital lobe, right visual pathway, and right parietal lobe.

fMRI of case 2 before transplantation. Negative signals (blue) are detected in bilateral occipital lobes (visual cortices).

fMRI of case 2 after transplantation. Positive (red) signals are detected in the right frontal cortex and parieto-occipital cortex.
Control Group
Three cases with improved visual function completed fMRI. Two showed some positive and negative signals in the visual pathway, whereas the other showed no changes (data not shown).
MRI (Table 2)
Treatment Group
Table 2 shows the MRI results of 16 effective patients before transplantation. There were no significant differences in terms of visual improvements among patients with one of the three most common types of brain abnormalities in this study, including decreased white matter and delayed myelination, periventricular leukomalacia (PVL), and cerebromalacia.
Control Group
The MRIs of nine effective cases are shown in Table 2. Among the three most common types of brain injury (decreased white matter with delayed myelination, PVL, and cerebromalacia), PVL patients showed the lowest rate of visual improvement.
Group comparison showed statistical significance only in PVL patients between the two groups. The effective rate of PVL patients in the treatment group was significantly higher than that in the control group.
Causes (Table 2)
The three main causes of CVI in this research were asphyxiation associated with preterm, preterm, and HIE. These patients showed no differences in the effective rates of visual improvement between the two groups.
Complications and Adverse Effects
Postoperative CSF leakage occurred in two cases and improved after use of a compression bandage and normal position recovery. Six cases got a fever (37.5–39.5°C) of 1–3 days' duration after transplantation, and one case got a fever for more than 5 days, with confirmation of no central nervous system infection after CSF examination. However, we observed bleeding in his head computed tomographic examination and his body temperature returned to normal spontaneously. No seizures appeared after transplantation. There were no serious adverse events related to transplantation in this study.
Discussion
Our results suggest that NS/PC transplantation is effective to treat severe CVI by significantly shortening the visual recovery time and increasing the rate of recovery. Severe neonatal brain injury, caused by perinatal hypoxia-ischemia and premature birth, is the main cause of neonatal cerebral palsy, which is frequently accompanied by CVI (28.2–69%) (5,10,14,16,22,24,38). CVI patients have a decreased visual acuity and a defective visual field. Some are completely blind. Previous studies suggest that CVI is mainly a result of injury of the visual pathway, PVL, or the injury of the calcarine fissure of the occipital lobe (25,26,42). Some children with CVI can improve their visual function through rehabilitative training by light stimuli and neural self-repair during development (4,15,16,22,35). However, for most CVI patients, especially the severe ones, there is no effective therapy to restore visual acuity (22,26).
NS/PCs can differentiate into multiple neural lineages, including neurons, astrocytes, and oligodendrocytes both in vivo and in vitro. Furthermore, they secrete multiple neurotrophic factors to promote the recovery of the injured neural tissue and neural functions. Here, we transplanted NS/PCs to treat patients with severe CVI. In the control group receiving just rehabilitative training, only 33.33% of children with CVI showed some degrees of visual improvement. Among these effective patients, 66.67% improved by one level, and 33.33%, by more than one level. In the treatment group receiving NS/PC transplantation in addition to rehabilitation, 64% of the patients had visual improvements after cell transplantation. Of these effective cases, 31.25% improved by one level, and 62.5% improved by more than one level. Furthermore, the median time of onset of visual function recovery was 60 days in the treatment group, significantly shorter than that of the control group (365 days). These results suggest that NS/PC transplantation is effective for treating severe CVI by greatly facilitating visual recovery. Such treatment may also be beneficial to the mental development of growing children and promote both mental and motor rehabilitation. The effect of the cell transplantation on the intellectual and motor function improvement has been reported in other articles (29–31,41).
Werth and Seelos reported that the fMRI of hemianopia patients showed active signals in the primary and secondary visual centers of the occipital lobe contralateral to the normal visual field; they also showed weak signals in areas contralateral to the blind visual field. Furthermore, they showed active signals in the primary and secondary visual centers of the occipital lobe after the visual recovery in bilateral CVI children (44). In our study, only a subpopulation of the patients in the treatment group received the fMRI examination. Their fMRIs showed few or no negative signals before transplantation, whereas after transplantation, there was the appearance of positive and more negative signals in the visual center and pathways. Two such cases, although they had positive and negative fMRI signals in their visual centers and pathways after transplantation, failed to show morphological changes in their MRIs. This suggests that the detected improvement of the visual function in these patients may not be a result of the structural repair of the visual center and pathways. Considering the relatively fast improvement rate of the visual function in most patients receiving transplantation, we suggest that the efficacy of NS/PC transplantation is probably due to the nutritional and trophic effects of the cytokines produced by transplanted cells onto residual neurons (such as luminance-sensitive cells) and/or silent synapses in the visual center, but not cell replacement per se (11,17,33,45). During early stages of neural development, there are a considerable number of synapses with normal anatomical structures that are kept in a silent state due to incapability of releasing neurotransmitters from presynaptic structures or absence of relevant receptors on postsynaptic membranes (18,34,43). The number of such silent synapses gradually reduced with development. Further studies showed that the silent synapses can be activated under certain circumstances. For example, neurotrophic factors such as nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF) can regulate the synaptic function and promote the release of neurotransmitters as well as play an important role in the conversion of synapses from silent to active during development (2,19,41). We hypothesize that neurotrophic factors secreted by the transplanted NS/PCs can also activate the silent synapse and “open” the unused visual pathways, thus improving visual function. The activation of the silent synapse may be one of the main mechanisms of the NS/PC treatment for CVI. Besides the paracrine effect, cell differentiation may be another mechanism partially accounting for the efficacy of NS/PCs. Evidence indicates that implanted NS/PCs could differentiate into multiple neural lineages in a region-specific manner. The differentiated neural cells could then reconstruct the neural circuits, receive excitatory and inhibitory signals from the adjacent host cells, and generate the action potentials (3,23,36). In rodents, the implanted NS/PCs did not seem to cause immune rejection and could survive for a long time in the brain (27,32). It is reported that the NS/PCs transplanted into the brain of patients with Huntington's and Parkinson's disease exhibit a robust survival at 4 weeks after transplantation (21,37). In our study, effective CVI patients showed no retrogression. Instead, their visual functions improved consistently along with development. Whether this phenomenon indicates a long-term effect of cell replacement remains to be determined.
Light stimulation, the traditional treatment for CVI, and the patient's own development both contribute to the visual function improvement in some CVI patients but not for the premature infant with PVL combined with CVI (6). In this study, PVL patients transplanted with NS/PCs showed a much greater improvement rate in visual function when compared with those with rehabilitation only. There were no obvious differences between the two groups because of limited patient numbers, but we still found relatively more cases with visual function improvement in the treatment group. This indicates that NS/PC transplantation may be a preferred treatment for PVL patients with CVI. However, larger-scale clinical studies are needed before making this conclusion. Previous animal experiments and other studies suggest that NS/PCs transplanted into the lateral cerebral ventricle can migrate throughout the whole brain and particularly toward the injury site (12,30). However, in this study, patients with fundus abnormality and retinopathy in both the treatment and the control groups did not improve their visual function, indicating a lack of efficacy of intracerebroventricular transplantation of NS/PCs in this type of patients. Further studies are required to determine whether the lack of efficacy is due to the ineffectiveness of NS/PCs per se for treating optic atrophy and retinopathy or the inability of intracerebroventricularly transplanted NS/PCs to migrate to the damaged optical nerve and retina.
This clinical trial was an open study; both the doctor in charge and the parents knew whether cell transplantation was performed, so subjective factors may exist in the judgment of the clinical symptoms. The oculist who participated was blinded to the treatments, and so their visual function rating was objective.
Minor adverse events occurred in some patients, and symptoms returned to normal in a very short time without neurologic sequelae.
In summary, human NS/PC-based cell therapy is effective to treat children with severe CVI. We recognize, however, that the number of the cases in this study is small, which precludes a correlation between the efficacy of cell transplantation and patients with different degrees of visual impairment, age, causes of disease, and brain injury types. Further studies are needed to determine the optimal transplantation route, time window, numbers of transplantation, and course of treatments.
Footnotes
Acknowledgments
The authors declare no conflicts of interest.