
Abstract
The aim of the study was to analyze the clinical efficacy and safety of olfactory ensheathing cell (OEC) transplantation for treating patients with chronic, complete spinal cord injury (SCI). Six patients with six chronic complete spinal cord injuries were recruited and treated with autologous OEC transplantation and followed for 24 months. The scores from before and after transplantation were analyzed. This was a self-control experiment. There was significant amelioration in the scores of the standard neurological classification of spinal cord injury made by the America Spinal Cord Injury Association (ASIA) and the International Association of Neurorestoratology–Spinal Cord Injury Functional Rating Scale (IANR-SCIFRS) following OEC transplantation with 24 months of follow-up. No clinical complications were observed. OEC transplantation would appear to be clinically safe and may promote the neurofunctional recovery of SCI based on data from six patients. This manuscript is published as part of the International Association of Neurorestoratology (IANR) supplement issue of Cell Transplantation.
Keywords
Introduction
Olfactory ensheathing cells (OECs) are a type of ensheathing cell that possesses the characteristics of both astrocytes and Schwann cells; they originate from the olfactory substrate located at the first and second layer of the olfactory epithelium in the olfactory nerve and bulb. OECs, as the major component of olfactory mucosa, possess the ability of continually renewing throughout life. They can guide growing axons from the neurons of the nasal cavity olfactory mucosa to the olfactory bulb to form synapses in the brain (2). Accumulating evidence has proven that OECs can significantly promote the axonal growth in chronic complete spinal cord injury (SCI). Nonetheless, there is still some doubt about OECs' therapeutic effect and safety (5,6,18). In the present study, six chronic complete SCI patients were treated with implantation of OECs, and the clinical efficacy and safety of OEC transplantation were studied by evaluating their functional recovery in follow-up.
Materials and Methods
Patients
In this study, six chronic complete spinal cord injury patients were enrolled and treated with transplantation of fetal OECs from January 2008 to December 2009. After transplantation, the patients were requested to perform regular neurofunctional evaluation tests during the 2-year follow-up. There were four males and two females in the study, with an average age of 39.67 ± 9.81years. The patients were diagnosed with SCI for a mean period of 18.83 ± 5.78 months. Two cases of damaged cord were located at cervical segments, and the other four cases were located at thoracic segments. All the patients were chosen by the following inclusion criteria: [1] MRI showed no compression of injured spinal cord and the pathogenetic condition was stabilized, [2] neurotrophic drugs or nerve growth factor had been administered before operation, [3] the spinal injury lasted at least half a year, [4] presence of complete case data, and [5] neurofunctional evaluation of SCI was America Spinal Cord Injury Association category A (ASIA A). All eligible patients and/or families were fully informed about the nature of the study and provided written informed consents before participating in the study. This study was approved by the ethics committee of the hospital.
Cell Culture
The olfactory bulb of fetuses aborted over 4 months old was digested with collagenase IA (Gibco, Gaithersburg, MD, USA) for 10 min at 37°C to produce a single cell suspension in phosphate-buffered saline (PBS). Cells were then cultured in Dulbecco's modified Eagle's medium + F12 supplement (DMEM/F12; Gibco) with 10% fetal bovine serum (FBS; Gibco) for 3–4 days, and the medium was then changed every 2–3 days. When confluency was reached about 2 weeks later, cells were subcultured for subsequent propagation to attain the required number of cells for the patient. Appropriate tests including phenotype and sterility test had been performed before transplantation. To carry out transplantation, cells were dissociated with 0.25% trypsin/0.53 mM ethylenediaminetetraacetic acid (EDTA; Invitrogen, Carlsbad, CA, USA), and the enzymatic activity was stopped by culture medium. The cell suspension was centrifuged, and the cell pellet was washed thrice with saline. The entire cell pellet was suspended in 1 ml saline and then was delivered to the operating room. Cells were then resuspended in 1 ml saline before being loaded into a syringe for transplantation. The cell viability was assessed using trypan blue (Gibco) exclusion. Cell viability was 95% or greater for them to be used for transplantation. The cell density was about 107/ml for transplantation.
Operation and Implantation of Olfactory Ensheathing Cells
Under general anesthesia, the postcenter longitudinal incision of the corresponding part of the spinal injury was chosen, the meninx fibrosa was sliced, and the spinal cord was exposed. Two million OECs at the final volume of 200 μl were injected into multiple corresponding points (~4–5) located at the borderline between the normal and abnormal spinal cord using a 0.45-mm infusion needle (Cook Critical Care, Bloomington, IN, USA) as determined by combining the result of the MRI with the hyper-plastic capillary and tissue damage observed through a microscope. Total number of OECs for each patient was about 2 × 106. After injection, the meninx fibrosa was tightly sutured with absorbable sutures (Vicryl, Ethicon Johnson and Johnson, San Angelo, TX, USA). Routine hemostasis and anti-infection were given after operation, and drainage tubes (Hemovac, Davol, Cranston, RI, USA) were kept in for 2–3 days.
Evaluation of Spinal Function
All six patients were evaluated at 1 week preoperatively and reevaluated at 3, 6, 12, and 24 months postoperatively. The curative effect was determined by comparing pre- and postoperative scores, based on the ASIA Impairment Scale (3) and International Association of Neurorestoratology Spinal Cord Injury Functional Rating Scale (IANR-SCIFRS) (10). An ASIA score was acquired based on the following factors: 1) Sensory function: Pinprick and touch sensations were tested at each dermatomal key point (28 points on each side of the body), and a 0–3 grade was then assigned (0, no sensation, in which blunt and sharp stimulations could not be differentiated; 1, sensory disorders; and 2, normal sensations); the pinprick and touch grades on each side were summed up to get a total sensory grade, which was used to indicate a possible change in sensory function. 2) Motor function: Ten key muscles on each side of the body were tested from top to bottom, and a 0–5 grade was then assigned according to strength; the grades on each side were summed up to get a total motor grade, which was used to indicate a possible change in motor function. 3) Anal sphincter was tested using finger testing. Sensory function was classified into presence and absence, and any sensation in the saddle area indicated an incomplete spinal cord injury. IANR-SCIFRS established a functional rating score, which includes nine categories with 16 items in total (plus one optional category). The maximum possible score is 48; the lowest possible score is 0; a functional rating scale score of 48 indicated normal functioning across all categories, 35–47 indicated a slight degree of functional handicap (mostly independent), 18–34 indicated a medium degree of functional handicap (some dependency indicated), and 0–17 indicated a severe degree of functional handicap (significant impact on daily life).
Statistical Analysis
The data were expressed as means ± SEM. Using SPSS16.0 for Windows (Chicago, IL, USA), paired sample t tests were performed for the comparisons of ASIA scores and IANR-SCIFRS before and after transplantation (24 months). A value of p < 0.05 was considered statistically significant.
Results
Spinal cord function showed significant improvement in all the six patients. Scores of ASIA and IANR-SCIFRS were significantly increased after operation and OEC transplantation (Tables 1 and 2). Sensory function, motor function, and autonomic nerve function, such as diaphoresis, had increased. Two patients experienced a urinary tract infection caused by the long-term indwelling catheter and had no influence on OEC transplantation effect. There were no long-term fever or other complications related with transplantation.
Standard Neurological Classification of Spinal Cord Injury (SCI) (ASIA)

ASIA, America Spinal Cord Injury Association.
International Association of Neurorestoratology–Spinal Cord Injury Functional Rating Scale (IANR-SCIFRS)
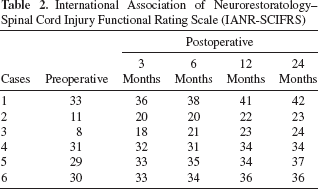
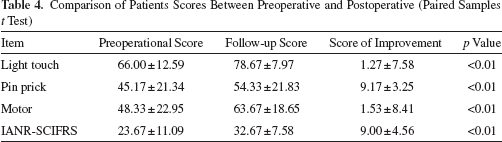
In all six cases, the mean increase in score was 12.7 for light touch, 9.1 for pin prick, and 15.4 for motor. The mean increased IANR-SCIFRS score was 9.0 (Table 3), while significant differences between pretreatment and posttreatment were observed (Table 4).
Characteristics of Six Patients

Comparison of Patients Scores Between Preoperative and Postoperative (Paired Samples t Test)
Discussion
Review of Spinal Cord Injury Research
Traditionally, the outcome of spinal cord injury by surgical methods is quite poor due to the absence of spontaneous regeneration functions in the neurons (16). Dimitrijevic proposed first in 1983 that there were healthy white matter fibers with electrophysiological transfer function in injured spinal cord tissue (4). Scholars in China confirmed that the independent limb motor function would remain 2/5 to 3/5 if the numbers of surviving axons in the injured corticospinal tract are over 10% (20). Other studies have proven that the regeneration capability of damaged axons could be restored, and partial neurological function recovery would be attained with the improvement of neurological function in an injured central nervous system. The dysfunction of neurons in injured segments can be compensated for by adjacent segments; however, attempts to date to restore function after spinal cord injury have remained essentially ineffective. In recent years, OEC transplantation has demonstrated promising therapeutic effects for SCI, which could promote neurofunctional restoration by remyelinating axons (1,15,17). In a preclinical study in a SCI rat model, treatment with OEC transplantation led to improved motor scores as well as sensory function. The OECs were found to bridge the affected area, manage axon myelinization, form functional connection, and accelerate electrophysiological velocity of conduction (7). It was also shown that OECs can secrete all kinds of neuronal growth factors necessary for neural development, differentiation, and maturation (19). Moreover, OECs can suppress the production of harmful factors such as gliotic tissues, thereby improving the microenvironment and promoting spinal cord regeneration (14).
Clinical Study on Olfactory Ensheathing Cell Transplantation for the Treatment of Spinal Cord Injury
Olfactory mucosa transplants were first used in human trials by Lima et al., who demonstrated the efficacy of whole olfactory lamina propria for promoting functional recovery in chronic, severe SCI patients (12). Raisman's group further isolated and purified OECs and found that injection of such cells into the lesion site of adult rats with complete transections resulted in improved motor scores and sensory function (11). Huang et al. (9) infused an OEC suspension into the damaged segment of the spinal cord of patients with SCI and showed the regeneration of spinal cord and improved neurological function. Other researchers injected OECs into 15 patients at Frankel grade A at different time intervals, which resulted in promoting neurological status at Frankel grade from A to C in six patients, as well as from A to B in five patients. No serious adverse reactions were observed (13).
In the present study, six cases of chronic complete SCI were treated with decompression surgery and/or conventional therapies such as neurotrophic drugs, acupuncture, and rehabilitation for longer than 6 months posttrauma. There were no other oppressive factors in addition to primary spinal cord injury and stable neurological function for more than 6 months. Thus, the possibility of spinal cord self-cure can be ruled out in clinical observation after OEC transplantation. We found that some patients' sensory and motor function showed improvement in 2 weeks after operation, which is difficult to explain by nerve axon growth or OEC reparation. It may be related with signal modulation or neural plasticity (8). OECs may change the local microenvironment of the injured spinal cord lesions and stimulate the short-term potentiation of neural plasticity, such as activating undifferentiated neurons and reducing denervation hypersensitivity, which could result in functional recovery with nonstructural or anatomical restoration.
The continuous functional improvement after OEC transplantation in this study can be attributed to the short-and long-term potentiation of neural plasticity, the neural pathways repairing, and reconstruction. Through 24 months of clinical follow-up, continued improvement tendency was also presented in the observation. Six cases of postoperative patients in 2 years experienced improvements of sensory and motor functions compared with preoperative symptoms, as well as the obvious improvement in skin nutrition. Therefore, OEC transplantation is feasible and safe, as well as helpful in repairing the spinal cord function of chronic SCI.
Conclusions
The postoperative effect indicated that OEC transplantation is a safe method to promote the neurofunctional recovery of SCI patients. Moreover, there were no severe complications with OEC transplantation.
Footnotes
Acknowledgment
The authors declare no conflicts of interest.