
Abstract
Cell encapsulation is a method of encasing cells in a semipermeable matrix that provides a permeable gradient for the passage of oxygen and nutrients, but effectively blocks immune-regulating cells from reaching the graft, preventing rejection. This concept has been described as early as the 1930s, but it has exhibited substantial achievements over the last decade. Several advances in encapsulation engineering, chemical purification, applications, and cell viability promise to make this a revolutionary technology. Several obstacles still need to be overcome before this process becomes a reality, including developing a reliable source of islets or insulin-producing cells, determining the ideal biomaterial to promote graft function, reducing the host response to the encapsulation device, and ultimately a streamlined, scaled-up process for industry to be able to efficiently and safely produce encapsulated cells for clinical use. This article provides a comprehensive review of cell encapsulation of islets for the treatment of type 1 diabetes, including a historical perspective, current research findings, and future studies.
Introduction
Cell encapsulation involves enveloping living cells in a semipermeable, biocompatible membrane that allows for a bidirectional flow through the membrane, with nutrients and oxygen diffusing into the membrane and waste products and therapeutic proteins diffusing out. Moreover, this membrane acts as a barrier by providing cells with protection against large molecules, such as immune effector cells, to consequently provide a method to circumvent graft rejection. The ultimate goal of encapsulation is to prolong graft function without the use of systemically toxic antirejection medications.
Although encapsulation has been around for almost a century, it has found renewed enthusiasm in the last decade given the advances in cell transplantation research and the connection between the two technologies. The first publication regarding cell encapsulation was performed in the 1930s, by Bisceglie et al., which revealed that mouse tumor cells encased in a polymer structure can survive in the abdomen of a guinea pig without being rejected by the body (10). In the last decade, there has been a surge of research in the field of cell encapsulation, and within the US alone there are currently over 36,000 patents for cell encapsulation technology. The most extensively studied model using encapsulation technology has been performed on isolated pancreatic islets for the treatment of type 1 diabetes mellitus (T1DM). The purpose of this article is to provide a comprehensive review on the topic of islet encapsulation, with particular focus on current research efforts, and give a prospective on the future direction of this technology.
Biomaterials for Encapsulation
Choice of Materials
Many considerations must be taken into account when selecting materials for an implantable, cell-containing device. These include the configuration of the device, site of implant, response of the host, loading of cells, preservation of cellular function, longevity of implant, purity of materials, and process reproducibility (26). In general, cellular encapsulation devices fall into two categories: fairly rigid preformed or flexible. Fairly rigid preformed devices are made of synthetic polymer membranes, which are then loaded with cells after fabrication, while flexible polymer hydrogel devices are formed around the cells. The firmer design is often designed to elicit a specific response from the host, such as development of neovasculature in the vicinity of the device. The more flexible approach often strives to minimize the host response, evading detection by the inflammatory and immune processes of the host. An example of a prefabricated, rigid device is the “Encaptra” (113), fabricated primarily from polytetrafluroethylene (PTFE), which has a long history of transplant studies using both primary tissue and cell lines, while “Diabecell” (134) is an example of a more flexible device containing microcapsules and made primarily of alginate. The Diabecell device is currently in clinical trials using xenogeneic tissue, primary neonatal porcine islets. Intravascular devices, in which the host blood supply flows through the device, have been largely abandoned due to risks of thrombus formation and bleeding risks (140).
A number of synthetic and biologic polymers have been explored over several decades for encapsulation. Naturally occurring hydrogels include collagen, gelatin, hyaluronate, fibrin, alginate, agarose, and chitosan. Synthetic agents include poly acrylic acid, polyethylene oxide, poly vinyl alcohol, polyphosphazene, polypeptides, and their derivatives (74,91,102,133). Poly lactic acid and poly glycolic acid form synthetic hydrogels that have been used for years in medical devices and continue to be the most popular synthetic materials for engineering, but have not seen widespread use in cellular encapsulation because they are designed to erode. A theoretical detriment to the erodable approach is that the encapsulated tissue will ultimately sensitize the host immune system, making retransplantation with “booster” grafts face a more aggressive host environment. Most investigators seek long-term or permanent devices.
Fabricating Devices
In selecting an appropriate material for encapsulation, the constituents need to be nontoxic materials, which are characterized by robust methods. However, purity and the identity of the starting materials is challenging with polymers, particularly when derived from natural materials, as in the case of alginates (69). Fabrication of the devices, whether preformed membranes or hydrogels cast in situ, needs to be controlled, reproducible, and characterizable. Next, one must decide whether an active response from the host is desired. Any encapsulation strategy introduces a diffusional barrier to oxygen flux that limits the metabolic potential of the encapsulated tissue. High oxygen flux is needed in the proximity of the encapsulated tissue, and many investigators strive to increase capillary density in nearby host tissue by using materials that invoke neovascularization, sometimes by molecular signals, such as platelet-derived growth factor (PDGF) (89), but more commonly by the physicochemistry of the polymers themselves. Rough surfaces have been shown to induce neovascularization, which is often in concert with fibrosis (76).
Frequently, materials are used that provoke a fibrotic response in the host. Because early stages of fibrosis include neovascularization, these agents seem to provide an early boost to cellular viability of the encapsulated tissue. However, given sufficient time, collagen deposition will follow, which over time will lead to vascular involution and insufficient oxygen supply. The rate of this process is highly dependent on the materials as well as the animal model, resulting in a wide range of reported graft duration.
The alternative is a “bioneutral” or “bioinvisible” approach, where the material used for encapsulation produces little or no response from the host's inflammatory and immune systems. Several materials qualify in this regard, including alginates, polyurethanes, and PTFE (Teflon). Some investigators favor hydrophilic hydrogels because the interfacial surface tension is minimized, resulting in decreased protein adsorption and cell adhesion. Of these, alginate has received the most attention in the field largely because alginate gels are stable to oxidative damage in vivo (152). Alginates are polyanionic carbohydrates that form gels under relatively mild conditions in the presence of polyvalent cations, such as calcium. These gels are frequently stabilized by treatment with polycationic polymers like polylysine, although these copolymers have demonstrated negative effects on graft function in rodents (109). Alginate gels are quite versatile materials. This variation of polymer's molecular weight, nature, sequence of the constituent sugar acids, and identity of cross-linking polycation allow for gels with a relatively broad range of physical properties, with the most important being mechanical stability and molecular permselectivity (Fig. 1). These advantages must be balanced against the challenges of consistently isolating and purifying alginates from natural sources.
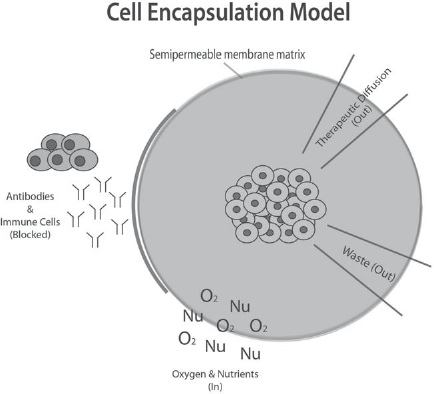
Cell encapsulation mechanism. Model displays the method in which cell encapsulation works. Cells are encapsulated in a semipermeable membrane, which allows communication with the host environment by means of a pore gradient. Small molecules such as oxygen (O2) and nutrients (Nu) can readily diffuse across, and therapeutic proteins can diffuse out, while large molecules, such as antibodies, are blocked from entering the graft and causing failure (95).
Alginate gels have been applied to cell encapsulation in several physical formats. The most common form of alginate used currently is small droplets containing cells ranging from 100 nm to 1 mm in size (38,136). These devices are formed by various means of droplet generation, resulting in some variation in overall size and placement of the cellular component within the droplets. Large, two-dimensional flat alginate sheets have also been investigated, where more control can be exerted on the dimensions of the devices and placement of the cells within (33,124). In all cases, the devices are formed from viscous polymer suspensions of cells and gelled in situ. Care must be taken when executing these processes to maintain vitality of the encapsulated tissue. In practice, the hydrogel barrier to oxygen flux must be less than a few hundred microns to support metabolic activity of the encapsulated tissue (23).
In contrast, preformed polymer membrane devices can be fabricated, sterilized, and subjected to quality control before loading with tissue. However, loading these devices to high density can present challenges. Furthermore, the relative distances between the immunoisolating membranes must be maintained during the life of the implant so as to maintain sufficient oxygen flux by passive diffusion from the adjacent host tissue. As a practical matter, this limits the overall size of these devices, with currently the largest device “Encaptra” holding just 250 μl of tissue (131). Transplantation of any encapsulated cell depends on many factors. In general, in choosing the appropriate encapsulation method and material, one must look at not only cell type being encapsulated, but also the transplantation site.
Historical Perspective
The US Center for Disease Control and Prevention (CDC) estimates that 25.8 million people (8.3% of the population) in the US have diabetes. The total medical costs of diabetes, direct and indirect, are estimated at $174 billion. This disease is progressive and over time results in irreversible damage to multiple organ systems, leading to devastating morbidity and mortality. Overall, the risk of death for patients with diabetes is approximately twice as high compared to same age nondiabetics (18). Currently there is no cure, but active and aggressive research has accomplished noteworthy breakthroughs. For instance, it has long been established that islets isolated from human cadaveric donor pancreata can be transplanted into patients to achieve insulin independence (50,116). This was a significant advance in the treatment of T1DM; however, these results were not sustainable.
In the 1990s, successes with islet transplantation were inadequate. Starting in 1990, data were collected for 8 years and showed only 12% of islet transplant recipients were able to achieve insulin independence for greater than a week (13). This changed in 2000, when the Edmonton group reported 100% success with achieving insulin independence in seven patients. The Edmonton protocol included transplanting at least 10,000 islet equivalents (IEQs) per kilogram (kg) body weight, which was usually obtained from two islet donors and the exclusion of glucocorticoids (115). This sparked a wave of enthusiasm for islet transplants with many centers adopting the Edmonton protocol for their islet isolations. Recently, however, the Edmonton protocol has encountered problems in reproducibility, and the clinical durability has been recently called into question (14); likewise, outcomes vary highly between centers. A paper in Diabetes Care published in 2012 reports that primary efficacy has improved in the years between 2007 and 2010 compared to patients that received islet transplants between 1999 and 2006. The rate of insulin independence at year 3 for those transplanted between 2007 and 2010 was 44% compared to only 27% between 1999 and 2002 (6).
The collaborative islet transplant registry (CITR) accumulates the most comprehensive collection of data regarding allogeneic islet transplants in North America, Europe, and Australia. As of 2008, there have been 325 adult recipients of islet transplants, and CITR reports that the number of severe hypoglycemic events and the glycated hemoglobin levels have significantly improved in those patients who underwent transplantation (3). Despite a standardized protocol among the centers performing allogeneic transplantations and the substantial decline in transplant recipients between 2007 and 2008, the CITR authors continue to support islet transplantations and report a positive impact in metabolic control for the recipients (3).
Based on data from CITR, islet transplant protocols that include the use of immunosuppressive medications had higher rates of insulin independence and lower rates of functional loss, as expected. This has resulted in many centers adopting the use of immunosuppressive medications either during induction, for maintenance, or both (3). The use of immunosuppression to promote graft function carries with it an immense degree of potential morbidity. In an international clinical trial in 2003, 36 patients received islet transplants with a reported 38 adverse and serious events, which can be attributed to immune suppression regimens. The transplanted patients suffered from infections, mouth sores, osteoporosis, gastrointestinal (GI) illness, and impaired renal function, to name a few (116). These side effects promote research into cell encapsulation because of its potential to avoid the use of systemically toxic drugs while enhancing graft function. This is perhaps why cell encapsulation research has been aggressively conducted on islets for the treatment of T1DM. A comprehensive review of the most relevant in vivo studies related to islet encapsulation research is given in Tables 1-3.
Small Animal Models of Islet Cell Encapsulation: The Most Relevant Small Animal Studies Performed on Islet Encapsulation

The author, the year of publication, the islet donor and recipient source, the islet equivalent (IEQ), the implant site, and the outcome of the study are provided.
Large Animal Models of Islet Cell Encapsulation: The Most Relevant Large Animal Studies Performed on Islet Encapsulation

The author, the year of publication, the islet donor and recipient source, the islet equivalent (IEQ), the implant site, and the outcome of the study are provided.
Human Clinical Trials: The Most Relevant Human Clinical Trials Related to Islet Encapsulation

The author, the year of publication, the islet donor and recipient source, the islet equivalent (IEQ), the implant site, and the outcome of the study are provided.
Small Animal Encapsulation Studies
Lim and Sun are widely recognized as the first group to produce the pivotal studies involving the encapsulation of islets for transplantation. In their groundbreaking work, islets were isolated from adult rats and encapsulated in alginate microcapsules for intraperitoneal (IP) transplantation into recipient rats (78). Compared to naked islets implanted underneath the kidney capsule, which only survived an average of 6–8 days (as was evident by the return of hyperglycemia), encapsulated islets survived up to 3 weeks posttransplant. Owing to the success of the Lim and Sun studies, several groups have expanded on the encapsulation model and experienced a spectrum of achievement. Souza et al. performed a retrospective review from 2000 to 2010 and found 56 articles that discussed islet transplantation in a rodent model (123). Thirty-four percent of the articles discussed encapsulated islets, while 37 articles (66%) discussed nonencapsulated islets. The best islet survival rate was found in the IP transplants of encapsulated islets, lasting an average of 100 days with the longest survival being greater than 365 days. In contrast, nonencapsulated islets survived best with direct injection into the liver with an average survival of 164 days with the use of immunosuppression. Studies performed by Suzuki et al., using a chamber-type device to encapsulate islets for transplants into mice, also showed positive results (129). Islets were isolated from male B6AF1 mice and encapsulated in alginate for syngeneic islet transplant into mice. The alginate solution was added to a variety of islet concentrations (250, 500, 750, 1,000) and then loaded into a prefabricated macroscaled diffusion chamber. The chamber consisted of two laminar membranes separated by a silicone rubber washer. Each device was implanted into the epididymal fat pad of the mice, which were previously rendered diabetic through a streptozotocin (STZ) injection. Results revealed that the greatest success with restoration of normoglycemia was achieved after 4 weeks posttransplant and continued up to 12 weeks in mice implanted with two devices containing 500 islets. Those with a higher islet load showed no significant improvement compared to the 500 isletloading group. The authors went further to characterize the amount of fibrosis surrounding the devices as fibrosis volume. In groups that were unsuccessful in achieving glucose control, the fibrosis volume was always substantially greater than the viable islet volume. The authors did not discuss in detail why some devices contained more fibrosis than others, but infection was believed to be the possible culprit in some devices that were unsuccessful.
Duvivier-Kali and colleagues performed studies on syngeneic and allogeneic islet transplants, using alginate microcapsules (36). Islets were isolated from male nonobese diabetic (NOD) and B6AF1 mice, and islet transplants were carried out in STZ-induced diabetic nude mice as well as spontaneous diabetic NOD mice. Control groups received nonencapsulated islets under the kidney capsule. High mannuronic acid alginate microcapsules, cross-linked with BaCl2 and without the traditional permselective component, were used to encapsulate 900–1,000 IEQs into the abdominal cavity of diabetic mice. Compared to naked islet transplantation under the kidney capsule of NOD mice, which resulted in normoglycemia for 4 ± 1 days, encapsulated islets maintained normoglycemia for >340 days in diabetic NOD mice, and islets from B6AF1 resulted in normoglycemia for >350 days in both diabetic mouse groups. After removal of the capsules after 49, 105, and 210 days posttransplant, reappearance of hyperglycemia occurred immediately. Interestingly, this group performed studies using blank capsules and discovered at explant 1 month after implantation that the capsules made of high glucuronic acid alginate resulted in a lower retrieval rate. Likewise, capsules with poly-l-lysine (PLL) coating resulted in an increased number of fibroblast overgrowth and broken capsules. Capsules that were cross-linked with BaCl2 resulted in a reduced fibrotic reaction compared to that done using CaCl2. These preliminary studies are highly beneficial in expressing the importance of biomaterial selection.
As was highlighted in these two studies, fibrosis discovered on the capsules posttransplant was likely related to the source material used for encapsulation. The choice of material used for encapsulation is likely the most important aspect in promoting the success of islet encapsulation. There are a number of other small animal studies using encapsulated islets that have shared in the success of these two authors. It has clearly been shown that this is a feasible technology in small animal studies; however, large animal models and human clinical trials have not displayed the same efficacy.
Large Animal Models of Encapsulated Islets
Unlike small animal models, there is a limited number of encapsulated islet transplant studies using large animals with the same success. These studies suggest that there have been many successes with this treatment; however, the small number of studies and the inconsistent results render the results inconclusive.
In one of the first large animal studies, Soon-Shiong et al. used alginate-coated islets transplanted into the peritoneum of diabetic dogs and showed islet function and improved glucose homeostasis up to 2 years after transplantation (120). The authors were meticulous in capsule selection and ultimately achieved an impressive graft survival of 726 days, as documented by the presence of C-peptide in one transplanted canine (119). The strength of these canine studies includes the documented absence of C-peptide prior to undergoing transplants, which is a fundamental aspect of islet transplants, as some researchers using large animal studies perform total pancreatectomy and concomitant islet transplants that improved glucose function cannot be accurately associated with the islets rather than the residual presence of pancreatic tissue from incomplete pancreatectomies. Interestingly, these studies performed in the early 1990s revealed excellent results; however, subsequent studies have been unable to significantly improve upon the graft survival achieved by Soon-Shiong and colleges. In primate studies performed by Dufrane et al., adult porcine islets were encapsulated in alginate and transplanted into primates with the purpose of showing that encapsulation quality improves outcomes (34). Primates that received high-quality alginate capsules were normoglycemic for 6 months without immunosuppression, and the majority of the grafts (86%) were free of fibrotic overgrowth at explantation, whereas naked porcine islets, or poor quality encapsulated islets, were rapidly destroyed after transplants.
A follow-up study by Dufrane et al. attempts to clarify the difference between micro- and macroencapsulation. This study uses adult porcine islets encapsulated in alginate microcapsules or in a macroscale device containing a double-sided collagen matrix with two layers of alginate for transplant. Encapsulated islets were either transplanted naked underneath the kidney capsule, in the peritoneum, (microcapsules) or subcutaneous (macrodevice) into diabetic primates (33). Compared to unencapsulated islet controls, which were rejected within 7 days, islets encapsulated in a macrocapsule device resulted in normoglycemia for up to 6 months in five animals. After implantation of a second macrocapsule device, normoglycemia was maintained for an additional 18 weeks. The results of their microencapsulated islets, however, improved capillary glucose levels for only 2 weeks. These results indicate that macroencapsulation of islets may provide additional advantage to islets' long-term survival and function.
As a further study that supports the idea of the limits of microencapsulation, Elliot et al. performed a study using microencapsulated neonatal porcine islets at a dose of 10,000 IEQ/kg, transplanted into the peritoneum of eight diabetic cynomologus monkeys (37). After 12 weeks posttransplant, there was a 36% mean drop in exogenous insulin need and a further drop of 43% at 24 weeks, compared to control animals. However, insulin independence did not occur in any of the transplant recipients. No adverse effects were noted apart from two animal deaths determined to be unrelated to the transplants. This study became the impetus for this group to proceed into their clinical trials.
Human Clinical Trials
Unlike the documented achievements seen in both rodent and large animal studies over the years, very few researchers have been able to proceed to clinical trials. Table 3 provides a comprehensive outline of the clinical trials performed on encapsulated islet transplants.
After the success of multiple transplantations in dogs, Soon-Shiong et al. were granted approval for the first encapsulated islet clinical trial. The subject was a 38-year-old male with long-standing T1DM and a previous renal transplant, due to end-stage renal disease. The patient had an average insulin requirement of 45–50 units per day and was maintained on low-dose cyclosporine and azathioprine for the renal transplant. A total of eight cadaveric pancreases were used for isolation and encapsulated in alginate. Encapsulated islets were then transplanted into the peritoneum at an initial dose of 10,000 IEQ/kg and, 6 months later, a supplemental dose of 5,000 IEQ/kg (121). The patient's insulin requirements reduced to 1–2 units per day, and in the ninth month he was able to discontinue all exogenous insulin. At the conclusion of the study, researchers discussed future plans, including transplanting patients that were not maintained on immune suppression as well as establishing the optimal dose of islets to be transplanted.
Basta et al. isolated human islets, according to the Edmonton protocol, and encapsulated them in ultrapurified alginate for implantation in four patients who were diagnosed with long-standing T1DM (8). Three out of four patients received an IP injection under ultrasound guidance and local anesthesia. The fourth patient underwent a laparotomy, and capsules were injected evenly beneath the liver and spleen. Islet dosing varied between recipients, ranging from 540,000 to 1,600,000 IEQs per patient. Transplant results showed that the transplant procedure was ultimately safe, with no significant postoperative side effects. One patient, in particular, revealed a significant reduction in hypoglycemic episodes compared to pretransplantation. Notably, at the 7-year follow-up, all patients were in good health; however, they were back on their original exogenous insulin regimens.
In a publication in Diabetes Care, Califiore et al. reported on their first two cases of encapsulated islet transplants. Human islets were isolated from cadaveric donors and encapsulated in microdroplets generated from highly purified alginate beads and transplanted into the peritoneum under sonographic guidance using a 14-gauge needle. Both patients showed improvements in their mean daily blood glucose levels and a decline in the need for exogenous insulin intake. Moreover, one patient had a disappearance in weekly hypoglycemic episodes and a biphasic C-peptide response during the oral glucose tolerance test (OGTT), and serum C-peptide was detected at 1 year and 6 months in patients 1 and 2, respectively. However, neither patient was able to achieve insulin independence (17).
In 2009, Tuch et al. reported the results from their human clinical trials where multiple islet infusions were performed. Islets were isolated from human cadaveric pancreases and microencapsulated in barium alginate capsules (136). A mean of 178,000 IEQs encapsulated islets per infusion were transplanted into four diabetic recipients. One patient received four islet infusions over 7 months; another received two infusions 10 months apart, and the remaining two received one infusion each. No immunosuppression was used; however, the group employed the use of an anti-inflammatory agent and antioxidants. In one patient, C-peptide was only detected on day 1 and became undetectable at 1–4 weeks. In the patient receiving four infusions, C-peptide was detected at 6 weeks and remained present for 2.5 years; however, the small amount of insulin produced did not alter his insulin requirements or glycemic control. Laparoscopy was performed at 16 months in the patient receiving four infusions, and capsules were noted to be surrounded by fibrous tissue, and encapsulated islets were noted to be necrotic. This, along with previous results, indicates the possibility that alginate encapsulation quality may be an important factor in predicting encapsulation islet transplant success, with less pure preparations causing higher degree of fibrosis surrounding the capsules, leading to islet necrosis and eventual transplant failure.
In a controversial trial performed in Mexico by Valdes-Gonzalez et al., porcine islets were transplanted into 12 T1DM patients with a mean age of 14.7 years (142). Porcine islets were encapsulated in a collagen device consisting of two stainless steel mesh tubes and a PTFE rod interior. These devices were implanted subcutaneously in the patients' abdominal wall. The devices were implanted and allowed to vascularize for a period of 2 months before the PTFE rod was removed, and 13,927–20,833 IEQs/kg were infused into the device. All patients except one received a second device 6–9 months later and a third device. No complications arose, and no evidence of infection with porcine viruses was detected after a 4-year follow-up. Half of the patients experienced a significant reduction in insulin requirements that continued for 4 years. Two patients became insulin independent for several months. Three years posttransplant, one of four devices was removed from four patients, and insulinpositive cells were present in the device. In a follow-up article in 2010, Valdes-Gonzalez reported on 23 patients transplanted between 2000 and 2004; all patients had the presence of urinary C-peptide, and approximately 50% of patients experienced a reduction of exogenous insulin dosing of more than 33% (141). Moreover, only 2 of 23 patients reported mild chronic complications associated with diabetes after transplant compared to 14 out of 23 patients prior to transplant. This level of chronic diabetic complications, per the author, is appreciably lower than same age T1DM without a transplant. Unfortunately, this group did not include a diabetic control undergoing extensive medical treatment to validate the statement.
Living Cell Technologies (LCT) has the most experience in developing and executing xenoislet transplants for human clinical trials. At the International Pancreas and Islet Transplant Association meeting in Prague in 2011, LCT reported on the outcomes of their current clinical trial (40). Neonatal porcine islets at a dose range of 5,000 to 20,000 IEQs/kg were microencapsulated in an alginate hydrogel and implanted into the peritoneal cavity of 14 adult recipients (Fig. 2). The most notable result of the transplants included a significant reduction in hypoglycemia (20 episodes pretransplant compared to 8 episodes at week 12–52 posttransplant) and a reduction in unaware hypoglycemia. Minor reductions in exogenous insulin dosing were achieved but not at a significant rate. Interestingly, this factor did not change despite islet dose received (5,000 IEQs/kg and 20,000 IEQs/kg). In 2004, Elliot's group reported on their long-term outcomes in a T1DM patient following alginate-encapsulated porcine islet transplantation (37,46). A 41-year-old male with insulin-dependent diabetes, for 18 years, received an IP transplant of 15,000 IEQs/kg porcine encapsulated islets. Glycated hemoglobin improved from 9.3 prior to transplant to 7.8 after 14 months. Moreover, C-peptide levels peaked at 4 months and remained detectable at 11 months. At 12 weeks, the patient's insulin dose was reduced to approximately 30%; however, his dose returned to baseline levels after follow-up at 49 weeks. There was an absence of a porcine viral infection in patient serum and biopsies of capsules taken up to 9.5 years after transplant. The patient continued to express an overall positive outcome from the procedure (38).

Microencapsulated islets. Islets were isolated from young pigs (26 days), matured for 8 days and then encapsulated in ultrapure low-viscosity mannuronate (UPLVM) alginate microcapsules, using an electrostatic encapsulator. Encapsulated islets were then stained with dithizone. Sample image is an isolated islet, approximately 150 μm in diameter, encapsulated in a 500-μm microcapsule. Scale: 100 μm. Picture is provided by Dr. Jonathan RT Lakey, UCI.
Xenotransplantation for clinical trials has gained considerable criticisms. For example, LCT data were debated by the International Xenotransplantation Association in 2007, as many believed their animal data were immature, and none of their publications documented long-term production of insulin in their primate studies (49). Likewise, the trials in Mexico were criticized in a paper published in Nature regarding the complete lack of animal studies and the young age of the recipients (19). Despite these ongoing concerns, however, the clinical trials continued.
In several press releases, LCT revealed the beneficial outcomes of their porcine islet transplants, where in four out of seven diabetic recipients, the number of hypoglycemic episodes was reduced on average by 44% and their glycosylated hemoglobin level improved from a mean of 8% before implantation to 6.8% after. Two of the patients have been able to completely stop exogenous insulin injection after their 4-month follow-up (39).
There have been significant triumphs in clinical trials; however, the progress has been slow, and the lack of reproducibility threatens to dampen enthusiasm. The studies have been extremely varied, including the devices used, the islet source, the dose of islets infused, and more importantly the outcomes. There is no standardization and no consensus among researchers what the ideal conditions are for these encapsulated transplants. This is a risky undertaking considering more devices continue to be studied, yet improvements on existing therapies have been sparse. Further proof of encapsulated islet transplant success in large animal studies and improvements on existing therapies needs to continue before the medical world can decide that this is a technology worthy of the excitement it is receiving.
Improving Encapsulated Graft Function
Graft Fibrosis and Rejection
Although, in theory, encapsulation prevents rejection by allowing the coated cells to evade immune molecules, it is not clear whether this hypothesis translates into clinical applications. As was revealed in studies from Suzuki and Duvivier-Kali as well as the human trial by Tuch et al., fibrosis was a significant problem encountered in their studies (36,129,136). In fact, Suzuki et al. went on to conclude that the success of the transplant was directly related to the volume of fibrosis encountered (129). Despite the avoidance of antibody recognition, fibrosis continues to plague many encapsulation devices for reasons that are not completely elucidated. Encapsulation effectively protects against large molecules such as antibodies and T-cells; however, proinflammatory cytokines such as interleukin-1 (IL-1) and anti-tumor necrosis factor-α (TNF-α) and other inflammatory molecules can freely diffuse across most hydrogel structures because of their lower molecular weight. These cytokines have been implicated in graft injury and failure in islet transplants (20,23,45).
Despite the tremendous advances in developing biocompatible encapsulation methods, many researchers have also begun to experiment with coencapsulating molecules or pretreating islets to further improve the viability of these transplanted cells and avoid graft injury (7,15, 27,57,108). Coencapsulated antirejection molecules will theoretically provide immune suppression at a local level, yet avoid systemic toxicity. In vitro studies done on coencapsulation showed promising results. Su et al. showed that islet cells encapsulated with an IL-1 inhibitor maintained a 60% greater viability than controls when placed in solution with proinflammatory cytokines (126). Likewise, Leung et al. found that in vitro alginate microcapsules encapsulated with anti-TNF-α were able to bind and remove active TNF-α from solution. TNF-α is one of the main cytokines responsible for promoting the inflammatory response; thus, its binding and removal would, in theory, promote greater graft survival (77). In a novel in vivo study, Bunger et al. showed that islets coencapsulated with dexamethasone implanted into mice peritoneum exhibited less local tissue fibrosis compared to the capsules, which did not contain dexamethasone (15). Others have mirrored this idea and coencapsulated nonsteroidal anti-inflammatory drugs implanted into a mouse model and witnessed superior graft survival and a decreased inflammatory response compared to controls (7,108).
Oxygen and Nutrient-Rich Environment
Although fibrosis is implicated in graft failure, ideal oxygen conditions are equally essential for graft survival (31,66). In studies performed by Dionne et al., islet secretion was determined to be 100% with a partial pressure of oxygen (PO2) of 60 mmHg, 50% at a PO2 of 27 mmHg, and only 2% at a PO2 of 5 mmHg (31). This theory was emulated in studies performed by De Vos et al., where in the absence of fibrotic overgrowth in their transplanted islet microcapsules, the presence of graft functional loss was attributed to necrosis in the center of the islet indicating poor nutrition, including oxygen, to the grafted cell. The authors proposed that the transplant site with a close blood supply to the grafts could alleviate this problem (28). Likewise, Pedraza et al. aimed to alleviate graft hypoxia by engineering an oxygen-generating biomaterial. The material made of polydimethylsiloxane-encapsulated solid calcium peroxide was found to generate oxygen for a period of 6 weeks. In vitro studies revealed that enhanced islet survival was observed with the addition of this device, as well as improved cell metabolic activity, decreased lactate dehydrogenase (LDH) and caspase activity, and improved glucose responsiveness and insulin release (101). With the substantial importance of oxygen and nutrient delivery to promote graft survival, researchers have studied the coencapsulation of factors such as vascular endothelial growth factor (VEGF) or other angiogenic factors such as fibroblast growth factor 1 and 2 (FGF1 and 2) (57,76,118). FGF 1 was examined in vitro and determined to have a slow release from the capsules for over 30 days in one study (57). Other researchers have discovered that pretreating islets prior to encapsulation can also promote longevity. In an in vivo study performed by Ludwig et al., STZ-treated rats were implanted subcutaneously with a macrochamber, made of an alginate slab, containing islets pretreated with a growth hormone-releasing hormone (GHRH) agonist and placed adjacent to an oxygen-permeable membrane. Chamber transplants resulted in normalization of glucose for up to 3 months, and when GHRH was introduced, normoglycemia was achieved earlier and more consistently and displayed a better response to the glucose tolerance test compared to untreated islets (81). A similar study was performed with pretreatment of islets with desferrioxamine by Vaithilingam et al., which showed increased expression of VEGF and reduced hypoxic stress (139). Research efforts are actively aiming to improve the islet encapsulation process, in hopes of improving transplant outcomes, which thus far have failed to show long-term insulin independence. Many aspects need to be considered in promoting effective encapsulated islet grafts including enhancing oxygen and nutrient diffusion, as well as avoiding cytokines and proinflammatory mediators from destroying the graft.
Sources of Islets: Xenotransplantation and Stem Cells
Ultimately, the extreme lack of available tissue sources is a large setback for the continued progression of this treatment. Currently, there are over 115,000 people waiting for an organ, and 18 people will die each day on the waiting list (138). Xenogeneic islets and stem cells are two avenues of addressing this shortage.
Xenotransplantation
With the increasing success of cell encapsulation and the ability to protect cells from being identified by the body's immune system, the possibility of transplanting cells from other species becomes an attractive possibility. Although highly controversial, the process of encapsulating cells from animals would be a solution to our distressing shortage of donated organs. Despite the ethical dilemma, animal tissues have been used in humans for decades. Animal advocates endorse that it is morally unacceptable to sacrifice animals for the benefit of humans. Although this is a legitimate debate, it should not be overlooked that the US uses more than 90 million pigs a year for food alone.
A major concern in xenotransplantation is xenozoonosis, which is the risk of developing new infections that are transmitted from animal to human, leading to a manmade pandemic (95). Porcine endogenous retroviruses (PERVs) are present in all swine and transferred through inheritance from multiple mutations in the swine genome over time. Most swine breeds contain 50 PERV genomes in their DNA, and although it does not cause infection in the pigs, it has the potential to cause infection in other species (100,114). Other such viruses are present in the swine genome that can potentially cause infections in humans as well. Despite this theoretical risk, Paradis et al. performed a retrospective collection of serum and cells on 160 patients that had been treated with pig tissue over 12 years prior and found no evidence of PERV infection (99). Currently, all xenotransplantation efforts have been halted in the US due to these concerns, but have continued elsewhere. As was discussed in the human clinical trials, LCT, a company out of Australia, has been conducting several trials with encapsulated porcine islets into diabetic human patients in one arm of their human clinical trials. The encapsulated porcine cells used are called “Diabecell,” which originated from a pathogen-free pig farm in New Zealand (79,80). New Zealand's strict animal quarantine practices, strenuous security measures, and geographic isolation have made it an attractive location for the development of these pathogen-free herds. Spring Point facilities, headquartered out of Minnesota, hopes to make the US a global contender in xenotransplantation research. Their pathogen-free, medical-grade porcine facilities have received the highest level of accreditation as a first time applicant (29). Although a significant triumph for researchers, it is yet to be determined whether clinical xenotransplantation will ever progress in the US as it has abroad.
Stem Cells
The latest forefront for encapsulation technology involves the use of stem cells as an infinite and renewable source of donor islets. Encapsulating stem cells is a relatively new area of research, and both adult stem cells and embryonic stem (ES) cells have been researched in the hopes of providing islets for cell replacement therapy. The use of stem cells for cell replacement continues to provoke legal and ethical debates, which is beyond the scope of this review; however, these issues are discussed in detail in a review by Street et al. (125). Beyond these concerns, researchers have discovered that ES cells can differentiate into insulin-producing cells either through gene manipulation or under culture conditions. However, attempts at differentiation usually resulted in cells with a weak response to glucose stimulation, poor insulin production, and uncontrolled cell growth (64).
Differentiation of ES cells into pancreatic-like structures was first published by Lumelsky et al. in 2001. In a procedure involving expansion and differentiation of nestin-positive cells from ES cell cultures in in vitro and in vivo studies suggested these ES cells were functionally and structurally similar to β-cells (83). While the insulin-positive cells generated contained 50 times less insulin per cell compared to a normal islet cells, studies revealed that insulin secretion occurred in response to varying glucose concentrations. These islet-like cell clusters were then grafted subcutaneously into STZ-treated mice and were found to remain immunoreactive to insulin upon graft harvest. Although grafted mice did not have sustained improvement of hyperglycemia, body weight and survival was significantly improved compared to control diabetic mice.
In an attempt to improve upon the protocol by Lumelsky et al., work by Blyszczuk et al. showed improved insulin secretion can be obtained from these islet-like cell clusters by expressing transcription factors that are important in pancreas development (12). The authors noted that the consecutive expression of paired box 4 (PAX4) combined with selection of nestin-positive cells and specific culture conditions resulted in the differentiation of ES cells that gave rise to insulin-positive cells that appeared similar to adult and embryonic β-cells. Between 1 × 106 and 2 × 106 cells were transplanted into STZ-induced diabetic mice under the left kidney and spleen, resulting in normalization of blood glucose levels.
In another study, this time using induced pluripotent stem (iPS) cells derived from skin fibroblasts, insulinsecreting cells were differentiated into cells that behaved like β-cells (4). In vitro, the cells responded to glucose in a dose-dependent manner, as would be expected with a peak insulin production seen with a 20-mM glucose stimulus. The insulin-secreting β-like cells were introduced via intraportal vein injection into the livers of mice modeling type 1 and 2 diabetes. STZ-treated mice served as a model for type 1 diabetes. These mice received the β-like cells, and normoglycemia was achieved after day 2 and continued up to 16 weeks posttransplantation.
Publications from these and many other authors encourage others to pursue stem cells as a potential infinite islet source, and future studies are looking into using cell encapsulation to encase stem cells for transplantation (4,12,65, 83,86).
Researchers have found that encapsulated stem cells continue to differentiate while encapsulated and ingeniously have a tendency to survive longer (1,2,60). Addae et al. used a mouse model to study the differentiation of ES cells into a neuronal phenotype and observed a twofold increase in neuronal differentiation, an increase in the specificity for interneuron differentiation, and a prolonged survival in the encapsulated stem cells versus nonencapsulated cells (2).
Very few studies have been performed using encapsulated islet-like stem cells for the correction of diabetes. Kadam and colleagues were able to produce functional pancreatic-like cells from the long-term culture of mesenchymal stem cells (MSCs) from full-term human amniotic membranes (55). Cells exhibited a basal insulin secretion around 20 pmol/ml and approximately 90 pmol/ml after glucose stimulation. These islet-like clusters were encapsulated in polyurethane–polyvinyl pyrrolidone microcapsules prior to transplantation into the peritoneum of diabetic mice. This resulted in normalization of glucose levels in the mice that were transplanted and IP glucose tolerance test that was similar to nondiabetic controls.
Novacell (now ViaCyte) is a company based in San Diego that has been working on an encapsulation device called TheraCyte. The TheraCyte device is made of a double membrane of PTFE. An inner membrane contains a selective membrane to prevent the diffusion of immune mediator to the cells, while the outer layer is composed of a less selective membrane to facilitate angiogenesis. In one study, researchers transplanted stem cells, which had been directed down the pancreatic lining into diabetic mice (65). After 2 months, these cells developed into structures that behaved like pancreatic islets and resulted in normalization of blood glucose levels in diabetic mice. However, one complication of the study was the incidence of teratoma formation in 5% of the rodents transplanted. Lee et al. reported their results using the TheraCyte device and stem cells developed from 18- to 22-week-old human fetal pancreata (75). Grafted cells were retrieved after 10 weeks of transplantation and were found not only to stain positive for insulin, but glucagon and somatostatin were positive as well. Although C-peptide levels were low after 12 weeks of transplantation, after 5 months mice exhibited increased C-peptide levels and glucose responsiveness. Other studies using the same device in nude mice revealed dismal results including undetectable human C-peptide and insulin levels; even after a glucose challenge, C-peptide levels rose only slightly above the detection assay in one rodent (86). Furthermore, at explantation, the device was noted to be encased in fibrotic tissue, and there were no histologically positive endocrine cells found in the device. These studies portrayed relatively poor results; however, researchers continue to improve and differentiate cells that behave increasingly like human β-cells from both adult and ES cells, which will potentially improve upon this treatment.
Conclusion
The improvement and advancement of encapsulated cell technologies would transform the medical field and our current approaches to a multitude of diseases. Although there have been vast accomplishments over the years, in both animal models and early phase human clinical trials, the field is far from seeing this application clinically. The success has been difficult to replicate, and there is yet to be an established protocol for the engineering, processing, or implantation of these coated cells. There's a need for a consensus among researchers performing encapsulated islet transplants to improve upon the current technology. Likewise, a streamlined scale-up process for industry needs to occur in order to efficiently produce biomaterials for encapsulation in order to promote safety, standardization, and affordability for its use clinically.
Footnotes
Acknowledgment
The authors declare no conflicts of interest.