
Abstract
Treatment of central nervous system (CNS) malignancies typically involves radiotherapy to forestall tumor growth and recurrence following surgical resection. Despite the many benefits of cranial radiotherapy, survivors often suffer from a wide range of debilitating and progressive cognitive deficits. Thus, while patients afflicted with primary and secondary malignancies of the CNS now experience longer local regional control and progression-free survival, there remains no clinical recourse for the unintended neurocognitive sequelae associated with their cancer treatments. Multiple mechanisms contribute to disrupted cognition following irradiation, including the depletion of radiosensitive populations of stem and progenitor cells in the hippocampus. We have explored the potential of using intrahippocampal transplantation of human stem cells to ameliorate radiation-induced cognitive dysfunction. Past studies demonstrated the capability of cranially transplanted human embryonic (hESCs) and neural (hNSCs) stem cells to functionally restore cognition in rats 1 and 4 months after cranial irradiation. The present study employed an FDA-approved fetal-derived hNSC line capable of large scale-up under good manufacturing practice (GMP). Animals receiving cranial transplantation of these cells 1 month following irradiation showed improved hippocampal spatial memory and contextual fear conditioning performance compared to irradiated, sham surgery controls. Significant newly born (doublecortin positive) neurons and a smaller fraction of glial subtypes were observed within and nearby the transplantation core. Engrafted cells migrated and differentiated into neuronal and glial subtypes throughout the CA1 and CA3 subfields of the host hippocampus. These studies expand our prior findings to demonstrate that transplantation of fetal-derived hNSCs improves cognitive deficits in irradiated animals, as assessed by two separate cognitive tasks.
Keywords
Introduction
Cranial radiotherapy remains the most effective way to treat a range of central nervous system (CNS) malignancies, from pediatric patients afflicted with medulloblastoma to adults stricken with glioblastoma multiforme. In the former case, radiotherapy can be curative (29), while in the latter case, irradiation improves progression-free survival (27,54). These survival benefits, however, come at the cost of debilitating cognitive decrements that adversely impact quality of life (15,21,39,40,50,55). Treatment-associated cognitive dysfunction is particularly problematic for pediatric patients in its severity, long-term nature, and socioeconomic impact (37,43,52). At present, no long-term, satisfactory solutions exist for the treatment of cognitive impairments caused by both radio- and chemotherapy (24).
While improvements in radiotherapy treatment strategies have limited radiographically visible morphologic injury to the brain parenchyma, such as radionecrosis and edema, a progressive onset of cognitive dysfunction invariably occurs (1,2,35,45). The cognitive decrements are multifaceted and manifest as impaired hippocampal-dependent (and independent) learning and memory and frequently include altered attention, concentration, and executive functions, such as planning and multitasking (41). Interventions to combat the long-term neurocognitive sequelae resulting from such cytotoxic cancer therapies have yet to be developed (21).
Considerable evidence points to the depletion of neural stem and progenitor cells as one of the contributory mechanisms underlying radiation-induced cognitive dysfunction. Irradiation has a profound impact on the small but neurogenically active population of stem cells in the subgranular zone (SGZ) of the hippocampal dentate gyrus (3,19,49,53,58). Many studies have now shown that ionizing radiation depletes radiosensitive populations of multipotent neural stem and progenitor cells in the hippocampus and elicits a persistent oxidative stress that fundamentally compromises the neurogenic niche, thereby leading to long-term impairments of neurogenesis (23,24). While the convergence of multiple mechanisms is certain to impact cognitive health, it is the temporal coincidence linking the loss of multipotent neural cells to the inhibition of neurogenesis and onset of hippocampal-dependent spatial learning and memory deficits that point to the importance of preserving neural stem cell pools (4,23,24).
The foregoing provides the backdrop for much of our work aimed at replacing those cells lost or damaged by irradiation. Our past work using an athymic nude rat model has demonstrated the efficacy of pluripotent human embryonic stem cells (hESCs) and multipotent human neural stem cells (hNSCs) in preserving cognitive function when transplanted intrahippocampally following cranial irradiation (3–5). Cells transplanted 2 days following irradiation were found to restore spatial memory performance on a novel place recognition task that relies on hippocampal function and is sensitive to radiation-induced deficits (3–5). Beneficial effects of cognition were found to persist out to 4 months following a single round of transplantations (3–5). Further analysis revealed significant survival of engrafted cells that migrated throughout the septotemporal axis of the hippocampus and differentiated along both glial and neuronal lineages (3–5).
This evidence suggests that stem cell-based strategies designed to preserve and/or replenish radiation-damaged and/or depleted stem cell pools in the brain may be capable of forestalling the development of cognitive impairments. In the present study, we have tested an FDA-approved, good manufacturing practice (GMP) human fetal-derived neural stem cell line to investigate its therapeutic potential in our established immunocompromised athymic nude (ATN) rat model. Here we report that transplantation of fetal-derived hNSCs reverses irradiation-induced cognitive dysfunction using two cognitive tasks and further show that engrafted cells exhibit robust survival and neuronal differentiation 1 month following cranial irradiation.
Materials and Methods
Animals and Irradiation Procedure
All animal procedures described were approved by the Institutional Animal Care and Use Committee (IACUC) and comply with NIH guidelines. The immunocompromised ATN rat model (strain 0N01, Cr:NIH-rnu) was used here, as in our previous studies (3–5). A total of 29 male ATN rats (2 months old, purchased from Frederick National Laboratory, NCI, Frederick, MD, USA) were maintained in sterile housing conditions (20°C ± 1°C; 70 ± 10% humidity; 12 h each light and dark cycle) and had free access to sterilized diet and water. Animals were divided into three groups: 0 Gy (no irradiation) sham surgery controls (CON, n = 12), 10 Gy irradiated sham surgery (IRR, n = 9), and 10 Gy irradiated with engrafted neural stem cells (IRR + NSI, n = 8). Rats were anesthetized, eyes and body were shielded, and the head was exposed to cranial γ-irradiation (10 Gy) using a 137Cs irradiator (J.L. Shepard, Mark I, San Fernando, CA, USA) at a dose rate of 2.07 Gy/min, as described previously (3).
Transplantation Surgery
The use of human stem cells in this study was approved by the Institutional Human Stem Cell Research Oversight Committee (hSCRO) under a material transfer agreement (MTA) with Neuralstem, Inc. (Germantown, MD, USA). The NSI566RSC cells (henceforth termed NSI) are human, fetal-derived NSCs developed by Neuralstem, Inc. NSIs were prepared and isolated from the cervical– upper thoracic region of the spinal cord obtained from a single 8-week human fetus after an elective abortion (30,34,63). The development and propagation of NSI cultures has been described in detail previously (30,34,63). The NSI cell line displayed abundant expression of Sox2 (sex-determining region Y box 2)/nestin and cells retained their capability to differentiate (neuronal and astroglial phenotypes), as described previously (33, 57,63). Immunocytochemical analysis was performed to confirm the characteristics of the cells (see text for details).
A day prior to each surgery, cryopreserved vials derived from a well-characterized GMP cell bank were thawed, washed, prepared in a hibernation buffer, and shipped overnight from Neuralstem to the University of California, Irvine (UCI). The following day, the cells were checked for viability and used directly for transplantation without further manipulation. On an average, the viability of NSI used in the present study was 80–85%.
The NSI cultures were transplanted into irradiated rats (Fig. 1A). At 2 days postirradiation, each rat received bilateral, intrahippocampal transplantation of 70,000 live NSI (IRR + NSI) in 1 μl of cell suspension using a 33-gauge microsyringe at an injection rate of 0.25 μl/ min. Both hippocampi received four distinct injections (total 2.8 × 105 live NSIs per hemisphere) using precise stereotaxic coordinates, as described previously (3). Sham-operated control (CON) and irradiated (IRR) rats received sterile vehicle (hibernation buffer) at the same stereotaxic coordinates.

Schematic of research design and immunocytochemical analysis of NSI566. (A) Two-month-old ATN rats received 10 Gy head-only γ-irradiation and were transplanted 2 days later with human-fetal derived neural stem cells (NSI566; NSIs). At 1 month posttransplantation surgery, animals were administered NPR and FC tasks. Three weeks later, after cognitive testing, animals were euthanized for immunohistochemical analysis. Nonirradiated control and irradiated animals receiving sterile hibernation buffer served as sham surgery groups. (B) Immunocytochemical analysis of NSI566 stained with 4′,6-diamidino-2-phenylindole (DAPI) shows strong expression and colocalization of the multipotent marker (nestin, red). In vitro differentiated NSIs express both neuronal (green, neurofilament proteins MAP2 and SMI312) and astrocytic (red, GFAP) markers. Scale bars: nestin, 10 μm; MAP2, SMI312, and GFAP, 50 μm.
Measurement of Cognitive Function
To evaluate the outcome of NSI transplantation on cognitive function, at 1 month posttransplantation, rats from CON, IRR, and IRR + NSI groups were tested on novel place recognition (NPR), contextual and cued fear conditioning (FC) tasks as described previously (3,4,19). The NPR task assesses spatial recognition memory and relies on intact hippocampal function (3,4,19). The FC task was administered in three phases over 3 days: a training phase, a context test, and a cued test. Cued FC memory has been shown to rely on intact amygdala function, while contextual FC memory additionally engages the hippocampus (19). For all phases, rats were placed in a PhenoTyper 3000 (Noldus Information Technology, Leesburg, VA, USA) comprised of a video camera for observation and live tracking during FC trials. The animals were tested on NPR followed by FC. For both tasks, video recording and automated tracking of the animals was carried out using a Noldus Ethovision XT system (version 7.0). The detailed procedures for the NPR and FC tasks have been previously described (3,4,18,19).
Immunohistochemistry and Confocal Microscopy
After completion of cognitive testing, animals were deeply anesthetized with isoflurane and euthanized by intracardiac perfusion with 4% paraformaldehyde (Acros Organics, NJ, USA). Tissues were processed in a sucrose gradient (10% to 30%; Sigma-Aldrich, St. Louis, MO, USA) and 30-μm-thick sections cut coronally through the hippocampus using a cryostat (Leica Microsystems, Wetzlar, Germany). Sections were then stored in phosphate-buffered saline (PBS) with 0.02% sodium azide (both Sigma-Aldrich).
Immunohistochemical and immunocytochemical studies employed both monoclonal and polyclonal antibodies. Primary antibodies were as follows: anti-Ku80 (human-specific DNA telomere-binding nuclear protein, mouse, 1:100, Stem101, StemCell, Inc., Cambridge, UK), anti-DCX (doublecortin, goat, Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA), anti-NeuN (neuron-specific nuclear antigen, rabbit, 1:250, Millipore, Billerica, MA, USA), anti-GFAP (glial fibrillary acidic protein, rabbit, 1:500, Millipore), anti-S100 (S100β protein, rabbit, 1:200, Millipore), anti-MAP2 (microtubule-associated protein 2; neuronal filament protein, monoclonal AP20, mouse, 1:200, Sigma-Aldrich), anti-SMI312 (pan-axonal neurofilament, mouse, 1:200, EMD Millipore), and antinestin (rabbit, 1:200, EMD Millipore). The secondary antibodies and detection reagents included biotinylated horse anti-goat IgG (1:200, Vector Labs, Burlingame, CA, USA), donkey anti-mouse and anti-rabbit conjugated with Alexa Fluor 488 or 594 (1:200, Invitrogen, Carlsbad, CA, USA), and TOTO-3 iodide (infrared nuclear counterstain, Invitrogen) as a nuclear counterstain for sections, while cells in culture were counterstained with 4′,6-diamidino-2-phenylindole (DAPI) blue nuclear stain (Sigma-Aldrich).
To identify and track the differentiated fate of transplanted human cells, representative sections were processed using dual immunoflourescence staining for human-specific nuclear antigen (Ku80) and various mature and immature neuronal (DCX, NeuN) and astroglial (GFAP, S100) markers, as described (7). Serial sections taken through the middle of the hippocampus were selected for staining and stored in Tris-buffered saline (TBS, 100 mM, pH 7.4, Sigma-Aldrich) overnight. Free-floating sections were first rinsed in TBS followed by Tris-A (TBS with 0.1% Triton-X-100, Sigma-Aldrich), blocked with 10% normal donkey serum [NDS (Sigma-Aldrich) with Tris-A], and incubated overnight in a mouse anti-Ku80 solution (1:100) prepared in 3% NDS and Tris-A. The next day, the sections were treated with donkey anti-mouse IgG conjugated with Alexa Fluor 594 (1:200) made with Tris-A and 3% NDS for 1 h. The sections were light protected, washed with Tris-A, and blocked in serum and primary antibodies for neuronal or glial markers. Color development was facilitated by Alexa Fluor-conjugated secondary antibodies, as described above, and counterstained with TOTO-3 nuclear dye for visualization of hippocampal morphology. Immunostained sections were rinsed in TBS and mounted on clean Vectabond (Vector Labs)-coated slides using SlowFade antifade mounting medium (Invitrogen). Ku80-positive cells were visualized under fluorescence as red, and DCX, NeuN, GFAP, or S100-positive cells were visualized as green. For quantification of differentiated phenotypes, dual-labeled sections from representative hippocampal sections were analyzed from distinct transplants derived from four animals in each group.
Laser scanning confocal analyses to identify phenotypic fate of graft-derived cells were performed using a Nikon Eclipse microscope (TE2000-U, EZ-C1 interface; Nikon, Tokyo, Japan), as described previously (3,4). Z-stack analyses (1-μm intervals) and orthogonal image reconstruction were done using Nikon Elements AR software (v3.22, Nikon Instech Co. Ltd., Tokyo, Japan).
Statistical Analyses
Statistical analyses were carried out using PASW Statistics 18 (SPSS, IBM Corporation, Somers, NY, USA). All analyses were two tailed, and a value of p ≤ 0.05 was considered statistically significant. In all cases, normal distribution of the data (Kolmogorov–Smirnov test) and homogeneity of variance (Levene's test of equality of error variances) were confirmed. When a statistically significant overall group effect was found, multiple comparisons were made using Fisher's protected least significant difference (FPLSD) post hoc tests to compare the individual groups.
For the NPR tasks, exploration ratio, or the proportion of total time spent exploring the novel spatial location (Tnovel/Tnovel + Tfamiliar) was used as the main dependent measure. The behavior of the animals during minute 1 of the 5-min and 24-h test phases was analyzed [for details, see Acharya et al. (3) and Christie et al. (19)]. The number of animals included for NPR task analyses were CON (n = 12), IRR (n = 9), and IRR + NSI (n = 8).
For the FC task, percentage of time spent freezing was used as the main dependent measure. Freezing was assessed during the final minute of the baseline (i.e., before tone–shock pairings were administered) and posttraining (i.e., after tone–shock pairings) phases. For the context test, freezing was assessed over the entire 5-min trial. For the precue test, freezing was assessed during the first minute, in which no tone was sounded, and for the cue test, freezing was assessed across the 3-min interval that the tone was sounded and for the final minute of the trial in which no tone was sounded. Repeated measures ANOVA was used to assess group (between-subjects factor) and phase (within-subjects factor) effects on freezing behavior [for details, see Christie et al. (19)]. A separate cohort of animals for each group (CON, IRR, and IRR + NSI, n = 8 animals) was analyzed for the FC task analyses.
Results
NSI Express Stem Cells and Neural Markers In Vitro
Prior to transplantation, NSI cells were tested in vitro for the expression of multipotent and neural markers. Robust expression of the neural stem cell marker nestin (red) validated the undifferentiated state of NSIs (Fig. 1B). Additional in vitro differentiation analysis demonstrated the capability of NSIs to generate cell types positive for the neuronal neurofilament proteins MAP2 and SMI312 (green) and astrocytic GFAP (red) following growth factor deprivation for 7 days (Fig. 1B).
Transplanted Human NSIs Improves Cognition
Novel Place Recognition Task
One month posttransplantation, animals were habituated and tested on the NPR task (Fig. 2A–C). Analysis of total time spent exploring both objects during the initial familiarization phase revealed an overall group difference (p < 0.0001) (Fig. 2A). IRR + NSI animals explored more than CON and IRR groups (p < 0.0001). Following a 5-min retention interval, IRR animals spent a significantly lower proportion of time exploring the novel place compared to CON and IRR + NSI groups (p < 0.0001) (Fig. 2B). On the other hand, after the 5-min retention interval, IRR + NSI animals did not differ from CON animals. Moreover, one-sample t tests comparing the exploration ratios of individual groups to chance (0.5, dashed line, Fig. 2B) revealed that CON (p < 0.001) and IRR + NSI (p < 0.0001) animals spent significantly more time exploring the novel place than expected by chance (dashed line, Fig. 2B), while IRR animals explored the novel spatial location less than expected by chance. Following an additional 24-h retention interval (Fig. 2C), the overall group difference was not significant (p = 0.09). One-sample t tests showed that none of the groups explored the novel spatial location significantly more or less than expected by chance following the 24-h delay. However, there was still a trend for the IRR animals to explore less (Fig. 2C).
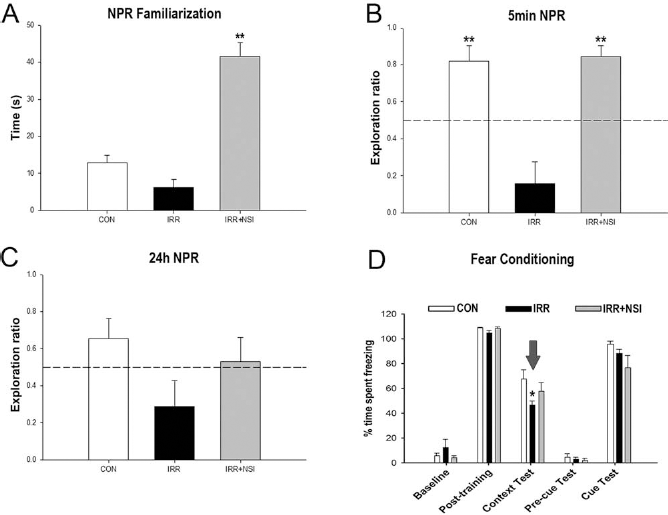
Human fetal-derived neural stem cell transplantation improved radiation-induced cognitive impairments at 1 month posttransplantation. For the NPR task, animals were first familiarized with two identical objects in specific spatial locations in an open field arena, and total time spent exploring both identical objects was assessed. Following a 5-min retention interval, animals were placed in the same arena with one object moved to a novel spatial location. (A) Analysis of total time spent exploring both objects during the initial familiarization phase of the NPR task revealed NSI-transplanted (IRR + NSI) animals explore more than controls (CON) and irradiatedsham (IRR) groups (p < 0.001, post hoc). Exploration ratios were calculated (Tnovel/Tnovel + Tfamiliar) for the first minute of 5-min (B) and 24-h (C) test sessions in the NPR task. (B) In the 5-min test phase, IRR animals spent a significantly lower proportion of time exploring the novel place (p < 0.001 vs. CON, and vs. IRR + NSI, post hoc), while CON and IRR + NSI animals did not differ. IRR animals did not spend more time exploring the novel place than expected by chance (dashed line at 50%). (C) Twenty-four hours after the initial familiarization phase, animals were presented with the same two objects, with one moved to a new spatial location. None of the groups spent more time exploring the novel place than expected by chance. For the context and cued FC task (D), baseline freezing levels were established using a series of five tone–shock pairings (posttraining bars, D), and all groups showed increased posttraining freezing behavior. Twenty-four hours later, a context test was administered, and the IRR group spent significantly less time freezing compared to CON, while CON and IRR + NSI did not differ (p = 0.014, post hoc comparisons, indicated by arrow). Forty-eight hours after the initial training phase, the context was changed, which resulted in a substantial reduction in freezing behavior in all groups (precue bars, D). Further, freezing levels were restored in all groups following the tone sound (cue test bars, D), indicating intact amygdala function in all groups. Data are presented as means + 1 SEM. p Values were derived from FPLSD post hoc comparisons. *p = 0.014 indicates significant difference versus CON and IRR + NSI, and **p = 0.001 indicates significant difference versus IRR animals.
Fear Conditioning Task
The three phases of the FC task (training, cue, and context tests) were administered over 3 days. A significant overall group × phase interaction effect (p = 0.03) was found by repeated measures ANOVA for the percentage time spent freezing during the FC task (Fig. 2D). Subsequent individual one-way ANOVAs conducted for each phase of the task revealed a significant group effect (p = 0.046) for the context test phase of the FC task (context text bars, Fig. 2D). Post hoc FPLSD tests showed that IRR animals spent significantly decreased percentages of time freezing compared to the CON group (p = 0.014), while CON and IRR + NSI groups did not differ. No significant group difference was observed in freezing behavior across baseline, posttraining, precue test, and cue test phases (Fig. 2D), indicating a selective deficit on the hippocampal-dependent contextual memory phase of the task. Furthermore, since all groups demonstrated significant increases in freezing behavior after the ton–shock pairings (posttraining phase), this suggests that irradiation did not impair motor or sensory function. The fact that cued memory was intact demonstrates that the acquisition of the tone– shock pairing was not impaired and that the deficit was specific to the memory of the context in which the pairing was learned.
Survival and Location of NSI in Irradiated Rat Hippocampus
At ~2 months posttransplantation, following cognitive testing, eight animals in each group were euthanized for immunohistochemical analysis to determine the pattern of integration of transplanted NSIs (Fig. 3). Examination of Ku80 (green) immunofluorescence-stained sections from IRR + NSI group demonstrated the presence of grafts along the entire septotemporal axis of the hippocampus (Fig. 3). Visualization with Ku80 marker (green) revealed that transplanted cells remained in clusters at the transplant site, and very few Ku80+ cells were observed migrating away from the transplant core in the irradiated host hippocampus (Fig. 3C–D). As shown in our previous studies (3–5), we aimed placement of transplants above the CA1 region, without disturbing the hippocampal milieu. With the exception of two animals (wherein transplant was found above DG), transplant-derived cells were located above the CA1 subfield with projections into the corpus callosum (CC), and they formed a transplant core (Tc, Fig. 3A–C). As shown in Figure 3, the location of transplant did not distort the host hippocampal cytoarchitecture (pink, TOTO-3 nuclear counterstain, Fig. 3).

Survival and location of transplanted NSIs. At ~2 months posttransplantation, NSI are located near the injection site [dual-labeled cells displayed as white, Nt, needle track; Tc, transplant core, (A–E) 5× to 60× magnification] and CA1 and CC areas. Transplanted NSI (green) did not show extensive migration patterns in the host hippocampus [dentate gyrus (DG), dentate hilus (DH), CA3 subfields]. Transplanted NSIs were detected by Ku80 (green) and counterstained with nuclear dye (TOTO-3, pink). Inset (E) represents orthogonal reconstruction of confocal Z-stacks. Scale bars: (A,B) 100 μm; (C) 50 μm; (D) 20 μm; (E) 10 μm; and (E, insert) 5 μm.
Differentiation of Transplanted NSI
To determine the phenotypic fate of transplant-derived cells in the irradiated animals following NSI transplantation, dual immunofluorescence and confocal Z-stack analyses were carried out in representative sections of the IRR + NSI group. Examination of dual immunofluorescence-stained Ku80+ and various neuronal and astrocytic markers demonstrated the presence of both phenotypes in the irradiated host hippocampus (Fig. 4). Transplant-derived cells expressed immature (DCX+, Fig. 4A) and mature (NeuN+, Fig. 4B) neuronal markers. Moreover, assessment of astrocytic differentiation using Ku80 revealed the presence of double-labeled immature (GFAP+, Fig. 4C) and mature (S100+, Fig. 4D) phenotypes. Orthogonal reconstructions of confocal Z-stacks are shown for each marker (Fig. 4a–d). Qualitative examination of all animals indicated that the majority of transplanted cells differentiated into neurons that were still in the developmental stage (DCX+, Fig. 4A) and located primarily in the transplant core, whereas a minority of transplant-derived cells expressed astrocytic markers (Fig. 4C–D).

Differentiation of transplanted NSIs in the irradiated hippocampus. At ~2 months posttransplantation, Ku80-positive (human-specific nuclear antigen, red) NSIs differentiated into immature [doublecortin (DCX) (A, a) green] and mature neurons [neuron-specific nuclear antigen (NeuN) (B, b) green] as visualized by dual labeling of neuron-specific markers with Ku80 (red). A similar pattern of differentiation was observed for immature [glial fibrillary acidic protein (GFAP) (C, c) green] and mature [S100 protein (D, d) green] astrocytes. Arrows indicate representative dual-labeled NSI transplant-derived cells (A–D). Confocal Z-stack orthogonal reconstructions of dual-labeled cells are shown for each neuronal (NeuN, a; DCX, b) and astrocytic (GFAP, c; S100, d) phenotype. DG, dentate gyrus; CC, corpus callosum. Scale bars: (A–D) 50 μm and (a–d) 10 μm.
Quantification of differentiated phenotypes revealed that the majority of engrafted cells expressed the immature neuronal marker DCX (24.5 ± 2.2%, Fig. 5) with a smaller percentage going on to express the mature neuronal marker NeuN (3.65 ± 1.0%, Fig. 5). Engrafted cells developing astrocytic fates were much smaller as the percentage of GFAP-positive (2.21 ± 0.2%, Fig. 5) and S100β-positive (2.29 ± 0.09%, Fig. 5) cells were lower in comparison. Thus, engrafted NSIs were found to preferentially commit to neuronal, rather than astrocytic, fates.

Engrafted NSIs differentiated into neuronal and astrocytic phenotypes 2 months after irradiation and transplantation. The majority of NSI graft-derived cells (Ku80+) differentiated into immature neurons [doublecortin (DCX)]. Transplanted NSI also differentiated into mature (S100β+) and immature (GFAP+) astrocytes, though minimal oligodendrocytic differentiation was observed at this time point (not shown). The data are represented as the mean ± SEM of four independent observations for each marker.
Discussion
The progressive and debilitating cognitive decrements associated with radiotherapeutic management of brain cancer have a significant and adverse impact on quality of life. While advancements in cancer treatment have improved the survival rate and life span of cancer survivors, many still suffer from neurocognitive sequelae with no satisfactory, long-term clinical recourse for their condition. Our past and present findings showing that cranially engrafted stem cells can either reverse or prevent the development of radiation-induced cognitive impairments suggest that stem cell replacement strategies might one day provide a much needed intervention for forestalling this serious side effect.
Our past data analyzed at 1 and 4 months posttransplantation indicated that hNSCs provided slightly better cognitive benefits than hESCs (25). There was also no evidence of teratoma formation at these posttransplantation times. Despite these positive results, translating such findings to the clinic invariably leads to important decisions regarding the best choice of stem cells, with safety and efficacy of chief concern. With this in mind, we decided to initiate the present studies using an FDA-approved, GMP hNSC from Neuralstem, Inc., referred to as NSI566RSC (i.e., NSI). The behavior of these cells and their differentiation into motor neurons in the rodent spinal cord has been characterized over the years (30,34,63). NSI cells have been successfully engrafted into the lumbar spinal cord of superoxide dismutase 1 (SOD1) transgenic rodent models of motor neuron disease (59,60,62). Engrafted cells underwent extensive neuronal differentiation, formed new synaptic contacts, released neurotrophic factors, and showed an advanced degree of structural integration into the motor circuitry, effects that likely contributed to the delayed onset and progression of disease in these models. More recent studies have found that engraftment of NSI cells in rats subjected to complete spinal cord resection stimulated functional recovery (36). Data show that grafted neurons were capable of overcoming the inhibitory microenvironment of the injured spinal cord, where they underwent extensive axonal growth and synapse formation to form new neuronal relays capable of restoring electrophysiological activity and behavior (36). These promising findings led the FDA to approve the first phase 1 safety trial of direct intraspinal transplantation of NSI cells into patients with amyotrophic lateral sclerosis (ALS). All 12 patients enrolled in this ongoing trial that received stem cell injections have tolerated the surgical procedures and transplants in the absence of any accelerated disease progression (12,25,48). Thus, current data demonstrate safety and may well lead to efficacy studies aimed at protecting motor neuron pools in ALS patients.
These findings were instrumental in our decision to promote the translation of our findings to the clinic and analyze the capability of the FDA-approved NSI cells to ameliorate radiation-induced cognitive dysfunction. Engraftment of NSIs was found to elicit significant improvements in cognition 1 month posttransplantation in rats receiving head-only irradiation, as assessed by two well-characterized and widely used cognitive tasks (Fig. 2). In contrast to irradiated animals that underwent sham transplantation surgery, the performance of NSI-engrafted animals was indistinguishable from unirradiated controls on the 5-min NPR task (Fig. 2B), with both controls and transplanted animals showing significant preference for exploring the novel place. Differences in exploration ratios between cohorts retested 24 h later on the NPR task were not found to be significant, as animals only showed a trend for exploring the novel location at this time (Fig. 2C). While we and other independent laboratories have shown that the NPR task is sensitive to radiation-induced deficits as well as cognitive improvements following transplantation surgery, group differences in locomotor activity and/or anxiety levels could confound this behavioral paradigm that relies on spontaneous exploration. However, group differences in anxiety levels assessed using an elevated plus maze were not observed (data not shown). Locomotor activity (distance traveled and velocity of movement) assessed during the initial familiarization phase of the NPR task revealed that irradiated animals, regardless of surgery, showed reduced locomotion and velocity compared to nonirradiated controls (data not shown). Thus, this prompted additional behavioral testing using a contextual FC task that does not rely on spontaneous exploration but is known to engage the hippocampus.
Using the FC task, a specific impairment was detected (Fig. 2D). Animals subjected to cranial irradiation spent significantly less time engaged in freezing behavior than controls during the context phase of the task. This finding suggests that irradiation disrupted 24-h memory for the shock–context association, which has been shown to rely on intact hippocampal function (46). Interestingly, animals engrafted with NSI cells demonstrated intact freezing behavior and were statistically indistinguishable from controls in their contextual fear memory. This finding suggests that stem cell transplants ameliorated a radiation-induced deficit in hippocampal function. The amount of posttraining freezing observed was comparable between all experimental cohorts, indicating that irradiation, sham surgery, and/or transplantation of NSI cells did not affect initial acquisition of the conditioned freezing response. Similarly, the experimental conditions imposed on animal cohorts did not affect freezing behavior during the cue test phase, indicating intact acquisition and memory for the conditioned tone stimulus, which has been shown to rely on intact amygdala function (46). The specific deficits in contextual fear memory observed in the present study suggest that irradiation selectively disrupts hippocampal function, which is consistent with the NPR deficits and disruptions in hippocampal neurogenesis that we observed in the present and many past studies (46,58). Similarly, the capability of engrafted NSI cells to reverse or prevent radiation-induced cognitive dysfunction corroborates our past data and points to the potential utility of these cells in another injury model of the CNS.
To date, the only routine application for stem cell therapy involves hematopoietic stem cell transplantation for the treatment of leukemia and lymphomas (28), which reconstitutes the immune system after whole-body irradiation (28), but can also facilitate the repair of brain injury in rodent models (44). Stem cell-based approaches have been used successfully in animal models to ameliorate neurodegenerative conditions such as Alzheimer's disease (10,61), as well as other disorders such as epilepsy (6,11,38) and traumatic brain injury (47). Importantly, we have now demonstrated that intrahippocampal transplantation of hNSCs can rescue cognition following exposure to cranial irradiation using three sources of stem cells (3,4). Our present findings demonstrate the utility of a GMP-derived stem cell line that has been granted FDA approval. Engrafted NSI cells survived and differentiated throughout the septotemporal axis of the hippocampus in sufficient yield to significantly ameliorate cognitive dysfunction at 1 month follow-up in animals receiving 1 Gy head-only irradiation.
In past studies, we have used a well-characterized immunohistochemical technique that capitalizes on the rapid and predictable expression of activity-related cytoskeletal protein (Arc) to address some of the possible mechanisms by which transplanted stem cells improve cognitive function. Arc is an activity-induced gene that correlates both temporally and spatially with the stimulus that induced its transcription (13,31,51). Our findings that transplanted cells express Arc suggest that engrafted cells can functionally integrate into neuronal circuits to ameliorate cognitive decline. This, however, is unlikely to account for all the potentially beneficial effects of transplanted stem cells, and trophic support derived from engrafted cells is likely important (10). In support of this idea is the observation that the transplant core has an extremely high yield of doublecortin-positive cells. These enriched areas of engrafted cells may promote the secretion of beneficial factors throughout the hippocampus.
In the present study, the majority of grafted cells developed neuronal phenotypes as validated by dual immunofluorescence staining of Ku80 with DCX or NeuN (Fig. 4). This result corroborates previous observations in which rodent models of ischemic paraplegia and ALS (SOD1 G93A) were transplanted with the same NSI cells (20,62). The microtubule-associated protein, DCX, is exclusively expressed (with some exception) by immature neurons from embryonic day 10 to ~2–3 weeks postmitosis (14,26,42). At the transplant core, there was marked differentiation of grafted cells into DCX-positive cells (Fig. 4), suggesting that the majority of NSI graft-derived cells developed neuronal phenotypes by 3 to 4 weeks postgrafting. Careful examination of the morphologic phenotypes of engrafted cells positive for either immature or mature neuronal or astrocytic markers did not reveal any overt aberrant features. Furthermore, there were no apparent disruptions to hippocampal architecture caused by the presence of the engrafted cells. Quantification of differentiated phenotypes (Fig. 5) confirmed that engrafted NSIs preferentially committed to neuronal rather than astrocytic cell fates. While a further time course study is needed to quantify the fate of individual cells, current results indicate robust survival of grafted cells ~2 months following transplantation in the irradiated CNS. Further, while evidence suggests that NSI graft-derived cells undergo extensive proliferation within the transplant core, this does not appear to translate into teratoma formation over the duration of our study.
Collectively, our data point to the importance of preserving the pool of multipotent cells in the brain. Similar concepts have been considered by the radiotherapy community, as improved treatments for brain cancer now routinely implement more sophisticated technologies and treatment planning designed to maximize dose to the tumor bed while minimizing radiation injury to the normal tissues of the brain (8). Stereotactic radiosurgical approaches [e.g., intensity-modulated radiation therapy (IMRT) and image-guided radiation therapy (IGRT)] provide the capability to design hippocampal sparing treatment plans in efforts to reduce adverse neurocognitive sequelae (8). The clinical benefit of protecting neurogenesis during the radiotherapeutic management of pediatric medulloblastoma has recently been estimated (9). When a variety of treatment plans designed to minimize the dose to the hippocampus were evaluated, the estimated risk for developing memory impairment was reduced by 33–47% (9). Confounding this potential beneficial strategy, however, is a recent study retrospectively analyzing patients that were treated for malignant glioma (22). Patients receiving larger doses to the stem cell niches did better, suggesting that stem cell niches in the brain harbor glioma stem cells (22). Therefore, while sparing the hippocampus may lead to improved cognitive outcomes at the risk of compromising progression-free survival, targeting the hippocampus may improve progression-free survival at the expense of debilitating cognitive decrements. A plausible, but unconfirmed, resolution to this dilemma may involve an intentional boost of irradiation to the neurogenic regions of the brain. This may enhance killing of migrant and resident cancer stem cells in efforts to prolong progression-free survival, which could be followed by cranial stem cell transplantation to restore cognition.
While stem cell transplantation may one day provide relief to the many cancer survivors trying to manage their neurocognitive sequelae, it is premature at this point to presume efficacy in the absence of any human data. With this in mind, the present efforts to initiate preclinical testing of an FDA-approved, GMP-derived NSI stem cell line moves these findings closer to the clinical arena. We are cognizant that additional mechanisms, involving disruptions to the blood–brain barrier and/or enhanced permeability of the specialized vascular niche in which stem cells reside (56), altered cerebral blood flow (16,32), and perturbations to neuronal anatomy (17,64), may contribute to the onset and progression of radiation-induced dementia. Nonetheless, lack of suitable and efficacious treatment options for the devastating side effects of cranial radiotherapy underscore the urgency for developing satisfactory interventions for this long-term mental health problem. Our efforts to thwart cognitive dysfunction by cell replacement therapy employing a GMP-derived cell line may provide the experimental backdrop for a potential solution.
Footnotes
Acknowledgment
This work was supported by the National Institutes of Health NINDS grant R01 NS074388 (CLL) and by Neuralstem, Inc. We thank katherine Tran, Nicole Chmielewski, and Lara Riparip for excellent technical assistance. The authors declare no conflicts of interest.