
Abstract
Different factors have been reported to influence islet isolation outcome, but their importance varies between studies and are hampered by the small sample sizes in most studies. The purpose of this study was to perform a systematic review to assess the impact of donor-, pancreas-, and isolation-related variables on successful human islet isolation outcome. PubMed, Embase, and Web of Science were searched electronically in April 2009. All studies reporting on donor-, pancreas-, and isolation-related factors relating to prepurification and postpurification islet isolation yield and proportion of successful islet isolations were selected. Seventy-four retrospective studies had sufficient data and were included in the analyses. Higher pre- and postpurification islet yields and a higher proportion of successful islet isolations were obtained when pancreata were preserved with the two-layer method rather than University of Wisconsin solution in donors with shorter cold ischemia times (CITs) [1 h longer CIT resulted in an average decline of prepurification and postpurification yields and proportion of successful isolations of 59 islet equivalents (IEQs)/g, 54 IEQs/g, and 21%, respectively]. Higher prepurification yields and higher percentage of successful islet isolations were found in younger donors with higher body mass index. Lower yields were found in donation after brain death donors compared to donation after cardiac death donors. Higher postpurification yields were found for isolation with Serva collagenase. This review identified donor-, pancreas-, and isolation-related factors that influence islet isolation yield. Standardized reports of these factors in all future studies may improve the power and identify additional factors and thereby contribute to improving islet isolation yield.
Introduction
Transplantation of islets of Langerhans can improve metabolic control and quality of life in patients with longstanding type 1 diabetes. Despite improvements and the standardization of isolation procedures, the outcome of human islet isolation remains unpredictable and highly variable. Furthermore, generally more than one islet preparation is required per recipient to achieve insulin independence after transplantation (18,22,46,68–70).
Previous studies have reported donor and other factors associated with higher success rates in terms of attaining adequate islet numbers for transplantation (1,5, 21,27,32,59,66). However, different factors have been identified, and large-scale trials in humans demonstrating the influence of a set of donor factors are lacking. Previous studies are relatively small, so factors could be missed. Therefore, different factors could be identified when studying larger numbers of donors, and the question remains which factors independently affect islet isolation outcome when corrected for the effect of other variables.
There is a shortage of donor pancreata relative to the needs of potential transplant recipients, and so optimal use of the available donor organs is vital. We carried out a systematic review of the literature on human studies reporting on donor-, pancreas-, and isolation-related factors and their influence on isolation outcome. In this way, we can identify factors that have an independent effect on islet isolation outcome.
Materials and Methods
Study Selection
PubMed (http://www.ncbi.nlm.nih.gov/pubmed/), Embase (http://www.elsevier.com/online-tools/embase), and Web of Science (http://wokinfo.com/) were searched to retrieve articles in English on human islet isolation from 1966 onward.
The following search string was used:
(“Islets of Langerhans Transplantation”[Mesh] OR ((“Islets of Langerhans”[Mesh] OR “islets”[all fields]) AND (“transplantation”[MeSH Terms] OR “transplantation”[All Fields])))
AND
(“isolation”[all fields] OR “Cell Separation”[Mesh] OR “Separation”[all fields] OR “Tissue and Organ Harvesting”[Mesh] OR “Harvesting”[all fields] OR “Tissue and Organ Procurement”[Mesh] OR “Organ Preservation Solutions”[Mesh] OR “Solution”[all fields] OR “Solutions”[all fields] OR “tissue donors”[MeSH Terms] OR “donor”[All Fields] OR “donors”[All Fields])
AND
(yield[All Fields] OR yields[All Fields] OR “isolation outcome”[All Fields] OR “isolation outcomes”[All Fields] OR “isolation result”[All Fields] OR “isolation results”[All Fields] OR harvest[All Fields] OR profit[All Fields] OR profits[All Fields] OR earnings[All Fields] OR earning[All Fields] OR output[All Fields] OR “success rate”[All Fields] OR “success rates”[All Fields] OR “recovery”[All Fields])
The search resulted (by April 2009) in 412 PubMed, 60 Embase, and 228 Web of Science titles, constituting a total of 700 titles. Two independent reviewers (D.E.H. and P.J.M.v.d.M.) examined titles and read relevant abstracts to decide if the full-text articles should be obtained. Cases of disagreement were resolved by discussing the title and abstract. Full-text articles (n = 141) were examined and selected on the basis of the following criteria: (1) reporting on either donor-, pancreas-, or isolation-related variables and their relation to islet isolation outcome; (2) reporting isolation outcome in islet equivalent (IEQ)/g pancreas pre- or postpurification; (3) sufficient specification of “successful” and “unsuccessful” islet isolation outcome as used in that study; (4) sufficient specification of donor organs used for islet isolation procedures with respect to selection characteristics.
Exclusion criteria were (1) histologically obtained pancreas variables and their relation to islet isolation outcome and (2) animal donor-, pancreas-, and isolation-related variables and their relation to islet isolation outcome.
Literature references were checked to minimize the risk of missing relevant studies. For duplicate papers reporting on the same study, we selected the article that reported the most complete and detailed data. This resulted in a total of 74 studies eligible for further analysis (2–17,19–21,23–38,40–45,47–49,51–67,71–83).
Data Extraction
Data were extracted independently by D.E.H. and P.J.M.v.d.M. by means of a predefined form. The following topics were included based on data availability in at least 50% of the studies:
– General variables: year of index admission, country of study, number of pancreata in the study
– Donor pancreas variables: age, body mass index (BMI), last serum glucose before procurement, donation after brain death (DBD) donors/donation after cardiac death (DCD) donors
– Pancreas variables: pancreas weight, cold ischemia time (CIT), method of preservation
– Isolation variables: method of purification (continuous vs. discontinuous and Ficoll vs. other), brand of collagenase
– Study results: islet isolation outcomes in terms of prepurification isolation yield, postpurification isolation yield, proportion of successful islet isolations (according to the definitions in the particular study).
Statistical Analysis
Because the number of pancreata varied considerably between studies, we weighted all isolation outcomes by the number of pancreata per study in all analyses. We studied the previously listed variables with respect to their relation with three outcomes: prepurification isolation yield, postpurification isolation yield, and proportion of successful islet isolations.
We first performed univariate analysis, relating each variable to each of the three outcomes. However, because the effect of some factors on isolation outcome may be confounded by others, a multivariate analysis was performed, including only the variables that had a significant effect on isolation outcome in the univariate analysis. In this way, the independent effect of each of the variables on the three outcomes was assessed. The analysis with the outcome proportion of successful islet isolations was adjusted for differences between studies in the criteria used to define successful islet isolation, varying between 100,000 and 350,000 IEQs, by including the criterion as a variable in the multivariate analysis.
Results
A total of 74 studies, all retrospective studies, met our inclusion criteria. When studies compared different groups in relation to isolation outcome [e.g., two-layer method (TLM) vs. University of Wisconsin solution (UW)], these were included as separate groups, giving a total of 132 groups that were finally compared in the analysis.
When studies addressed both pre- and postpurification isolation yield and/or proportion of successful isolations, we included the studies in the analyses of each outcome.
Prepurification Isolation Yield
Thirty-nine studies (2,5,9,10,16,23,24,26,27,30–38, 40,43–45,47–49,51–53,55,56,59–62,66,73,77,78,82), 70 groups in total, reported characteristics influencing prepurification isolation yield. Univariate analysis showed several factors to significantly affect prepurification isolation outcome (Table 1): higher yields were obtained in studies with younger donors, with higher BMI, without a last glucose or a low last glucose reported, with relatively few DBD donors, short CIT, and preservation with TLM rather than UW. These effects remained in multivariate analysis (Table 2), suggesting that each of these factors independently influenced prepurification yield. For example, from donors who are 1 year older, on average a 64 IEQ/g lower prepurification yield was obtained. Furthermore, when CIT was 1 h longer, on average a 59 IEQ/g lower prepurification yield was obtained, independently from other factors.
Factors Influencing Pre- and Postpurification Isolation Yield and Proportion of Successful Islet Isolations: Univariate Analysis

Data available in less than 50% of the studies. DBD, donation after brain death; TLM, two-layer method; UW, University of Wisconsin solution.
Factors Influencing Pre- and Postpurification Isolation Yield and Proportion of Successful Islet Isolations: Multivariate Analysis
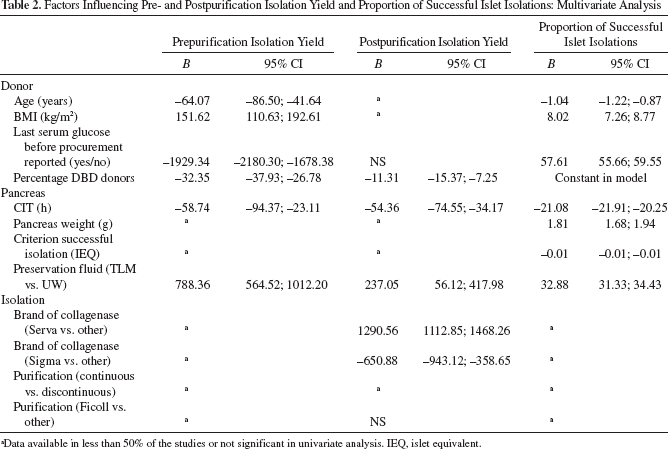
Data available in less than 50% of the studies or not significant in univariate analysis. IEQ, islet equivalent.
Less than 50% of the included studies reported data on pancreas weight and isolation-specific characteristics so these were excluded from the analysis.
Postpurification Isolation Yield
Sixty studies (2–9,12–16,20,23,25–30,32–38,40–42, 45,47–49,51–53,56–61,63–67,71,72,74–81,83), 106 groups in total, reported characteristics related to postpurification isolation yield. Univariate analysis showed several factors to significantly affect postpurification isolation outcome (Table 1): higher yields were obtained in studies without a last glucose or a low last glucose reported, with relatively few DBD donors, short CIT, preservation with TLM rather than UW, purification with Ficoll, and isolation with Serva collagenase. In multivariate analysis (Table 2), these effects remained as independent significant effects influencing postpurification isolation yield, except for last glucose before procurement and purification with Ficoll. For example, when CIT was 1 h longer, on average a 54 IEQ/g lower postpurification yield was obtained, independently from other factors.
In contrast with prepurification yield, age, BMI, and last glucose before procurement are not independent predictors of postpurification yield.
Less than 50% of the included studies reported data on pancreas weight and isolation-specific characteristics so these were excluded from the analysis.
Proportion of Successful Isolations
Thirty-one studies (5,11,12,17,19–21,24,26,27,29,31, 32,38,43,47,48,54,55,57,59,64,66,67,71,75–77,80–82), 57 groups in total, reported characteristics related to the proportion of successful isolations. In univariate analysis (Table 1) higher yields were obtained in studies with younger donors, with higher BMI, without a last glucose or a low last glucose reported, with relatively few DBD donors, short CIT, higher pancreas weight, and preservation with TLM rather than UW. In multivariate analysis (Table 2), these effects remained as independent predictors of a high percentage of successful isolations, except that higher percentage of successful isolations were found in studies that did report the last glucose before procurement. Furthermore, the percentage of DBD donors had no independent significant influence on the percentage of successful islet isolations.
For example, from donors who are 1 year older, on average a 1% lower percentage of successful isolations was obtained. Furthermore, when CIT was 1 h longer, on average a 21% percentage of successful isolations was obtained, independently from other factors.
In contrast with prepurification yield, the percentage of DBD donors is not, whereas pancreas weight is, an independent predictor as well as age, BMI, and last glucose before procurement in contrast with postpurification yield.
In total, data of 2,198, 4,122, and 2,769 pancreata were available for uni- and multivariate analysis of pre- and postpurification yield and proportion of successful islet isolations, respectively. However, in univariate analysis, 12.5% to 33.7% of the pancreata were excluded in at least one analysis due to missing data. In multivariate analysis, this was even higher (79.4–89.7%) because studies had to report on all of the variables included in the analysis to have their pancreata included.
Discussion
The present study has shown that donor-, pancreas-, and isolation-related factors have an influence on both pre- and postpurification islet isolation outcome as well as on the proportion of successful islet isolations.
Higher islet yields and a higher proportion of successful islet isolations were obtained when pancreata were preserved with TLM compared to UW. This is in accordance with Agrawal et al. (1). In their meta-analysis, significantly higher yields were found in pancreata preserved with TLM compared to UW. However, in their study, they found an equal rate of successful islet isolations in both groups. A possible explanation for this difference with our study could lie in the fact that in our multivariate analysis, the influence of TLM is corrected by other factors that have an influence on islet isolation yield.
Higher BMI and shorter CITs were also associated with higher islet isolation outcome pre- and postpurification as well as with a higher percentage of successful isolations when looking at CIT. Because larger islets are usually encountered in patients with higher BMI to obtain the higher insulin demand, and longer CITs result in more damage to the islets, these results seem to have face validity and have been well reported in previous studies (8,39,48,54,57,59,66).
Our study showed lower isolation yields and proportion of successful isolations in studies with a higher percentage of DBD donors. This is remarkable because in previous studies generally higher yields were found in DBD donors compared to DCD donors. However, successful islet isolations from DCD donors have also been reported previously (43,46,50,83). In our multivariate analysis, studies with a large percentage of DBD donors had significantly lower yields in pre- and postpurification isolation outcome and also a lower proportion of successful isolations when adjusted for the effects of other variables. Part of the explanation could be that in previous studies there was insufficient power to correct for other variables. In the studies that did correct for other factors, the results could be prone to the effect of the other, potentially underreported, factors in the models. This last explanation could also have an effect on our results. Furthermore, results of different studies cannot be easily compared without correcting for certain factors like age, as an age difference of 1 year has an influence on prepurification islet yield of 64 IEQ/g. Another explanation could be that the better outcomes of DCD donor might be center related. Most centers use DBD donors for islet isolation procedures. It could be that only centers with great experience in islet isolation would use DCD donors, leading to better results. Future studies should explore whether this explanation is valid, for example, by looking at DCD and DBD data for centers performing both procedures and by investigating whether centers performing more islet isolation procedures also have better outcomes.
This study is a first attempt to look at the effect of donor-, pancreas-, and isolation-related factors on isolation outcome. When reports of these variables in future studies would be standardized, we could possibly identify other factors and make a more accurate estimation of the independent effect of these factors. To illustrate the necessity of these standardized reports, we have looked at the missing variables in our analysis. In univariate analysis, 66.3–87.5% of the available pancreata were analyzed on the effect on pre- and postpurification yield or percentage of successful isolation. In multivariate analysis, this percentage was only 10.3–20.6% due to missing data on at least one of the variables included. This indicates that the studies differ to such a great extent in the variables that they report, even when we selected only those variables that were reported in most studies. This high percentage of missing data on different variables means that it was not possible to perform a meta-analysis.
Standardized reporting of the factors in all studies in the future on a minimal set of variables would also lead to a better fit of the model used in any meta-analysis. In the current analysis on postpurification yield, 19% of the variance in islet isolation outcome could be explained by the included variables. In prepurification islet yield and proportion of successful isolations, this percentage was better, but still only 50% of the variance could be explained. This suggests that besides the reported variables, other factors also influence isolation outcome.
In conclusion, this study identified donor-, pancreas-, and isolation-related factors that influence islet isolation yield. However, standardized reports of these factors are lacking and are needed to get more reliable evidence. To improve the power and provide better comparisons in future research, standardized reporting of these factors is recommended.
Footnotes
Acknowledgment
The authors declare no conflict of interest.