
Abstract
The selection of enzyme blend is critical for the success of human islet isolations. Liberase HI collagenase (Roche) was introduced in the 1990s and had been widely used for clinical islet transplantation. More recently, a blend collagenase NB1 has been rendered available. The aim of this study was to evaluate the isolation outcomes and islet quality comparing human islet cells processed using NB1 and Liberase HI. A total of 90 isolations processed using NB1 (n = 40) or Liberase HI (n = 50) was retrospectively analyzed. Islet yield, function in vitro and in vivo, cellular (including β-cell-specific) viability and content, as well as isolation-related factors were compared. No significant differences in donor-related factors were found between the groups. There were also no significant differences in islet yields (NB1 vs. Liberase: 263,389 ± 21,550 vs. 324,256 ± 27,192 IEQ; p = n.s., respectively). The pancreata processed with NB1 showed a significantly longer digestion time (18.6 ± 0.7 vs. 14.5 ± 0.5 min, p < 0.01), lower β-cell viability (54.3 ± 3.4% vs. 72.0 ± 2.1%, p < 0.01), β-cell mass (93,671 ± 11,150 vs. 148,961 ± 12,812 IEQ, p < 0.01), and viable β-cell mass (47,317 ± 6,486 vs. 106,631 ± 10,228 VβIEQ, p < 0.01) than Liberase HI. In addition, islets obtained with Liberase showed significantly better graft function in in vivo assessment of islet potency. The utilization of collagenase NB1 in human islet isolation was associated with significantly lower β-cell viability, mass, and islet potency in vivo in our series when compared to Liberase HI, even though there was no significant difference in islet yields between the groups. Evaluation of viable β-cell mass contained in human islet preparations will be useful for selecting enzyme blends.
Introduction
Despite the widespread use of glucose monitoring and new insulin formulations, many individuals with diabetes still develop devastating secondary complications such as retinopathy, nephropathy, neuropathy, and cardiovascular disease (12,21). The recent developments and improvements in islet transplantation-related technology and immunosuppressant medications allow restoring near normal glucose control in patients with brittle type 1 diabetes with minimal risk of serious hypoglycemic episodes that are associated with intensive insulin therapy (7,13,18,33,41,42).
The critical procedure of islet isolation is a mechanically enhanced enzymatic digestion of the pancreas, which allows dissociation and freeing of the islets from the surrounding acinar tissue (27,38). Collagenase plays a crucial role in dissociating the pancreas during enzymatic digestion phase. Liberase HI collagenase (Liberase; Boeringer-Mannheim/Roche) has been utilized as a standard blend for clinical islet transplantation since 1994 (28). More recently, the collagenase NB1 blend (SERVA) has been rendered available and utilized for clinical trials in human islet isolation.
Incidentally, concerns on the potential risks of contamination of the animal tissues utilized in the manufacturing of Liberase HI led to the decision to voluntarily suspend its use for clinical-grade human islet cell products worldwide. Thus, the only alternative option for clinical use became collagenase NB1. This conversion created substantial effects on islet transplant activity through the significant fluctuation of islet yield and quality.
In this study, we retrospectively analyzed and compared human islet isolations processed using Liberase HI and collagenase NB1 blends in terms of isolation outcomes, isolation-related factors, and islet quality. Our β-cell-specific islet assessment methods revealed significantly better quality of islets processed using Liberase HI, even though classic assessment methods such as fluorescein diacetate (FDA)/propidium iodide (PI) could not distinguish differences in islet yield.
Materials and Methods
Human pancreata from multiorgan donors with consent for research and/or clinical use were processed deceased at the Human Islet Cell Processing Facility of the Diabetes Research Institute at the University of Miami Leonard M. Miller School of Medicine (DRI-UM). Fifty-seven human pancreata were processed between March 2007 and December 2009 using collagenase NB1 (9 lots: 2,580 ± 162 Wunsch) with Neutral Protease NB (6 lots: 269 ± 105 U/vial) (SERVA Electrophoresis, Islandia, NY). Based on the donor selection criteria (Table 1), 17 out of 57 pancreata were excluded from this study. As control group, we used human pancreata that met the same criteria and were processed using Liberase HI (6 lots: 2,276 ± 187 Wunsch) (Roche, Indianapolis, IN) between February 2004 and August 2007.
Exclusion Criteria

Human Islet Isolation
All islet isolations were performed using a modified automated method with the same protocol, as described previously (38). Briefly, pancreata were immersed in an antibiotic solution prior to removing the surrounding vascular and adipose tissues. After cleaning, the pancreas was cut at the neck dividing the pancreas into two portions, the head and tail. Two 16-gauge catheters were then inserted into the main pancreatic duct of both pancreas portions. The dissociation buffer containing either collagenase NB1 or Liberase HI blend was perfused into the main pancreatic duct with a pump that automatically adjusts the flow rate to maintain constant pressure (38). After achievement of pancreas distension, seven to nine pieces were transferred into a digestion chamber with the same dissociation solution. The chamber was gently shaken to allow the pancreas to dissociate by both internal and external mechanical and enzymatic digestion. The digested pancreatic tissue was diluted, collected, and washed three times with chilled solutions. The islets were purified with either only continuous or continuous following discontinuous density gradients using a COBE 2991 Cell Processor (Gambro Laboratories, Denver, CO) at 4°C (17,32). Islet yield and purity were determined by dithizone (DTZ) staining (37). Islet counts were obtained before (pre) and after (post) purification as well as after culture by scoring islets with incremental diameter size ranges and data expressed in islet particulate number (IPN) and islet equivalent number (IEQ).
Fractional β-Cell Viability Assay
Fractional β-cell viability was determined using flow cytometry, as previously reported (15,19,20). Single cell suspensions were incubated for 30 min at 37°C in phosphate-buffered saline (PBS) without Ca2+ and Mg2+ and with Newport Green PDX acetoxymethylether (NG; 1 mM) and tetramethylrhodamineethylester (TMRE; 100 ng/ml; both from Molecular Probes). Cells were stained with 7-aminoactinomycin D (7-AAD; Molecular Probes), a marker of cell death. Cell suspensions were analyzed (minimum 3.0 times; 104 events) using a FACScan cytometer with the CellQuest-pro software (Becton Dickinson, Mountain View, CA, USA). After counting, the dead cells (7-AAD) were excluded from further analysis, live β-cells (NGbright) were analyzed for mitochondrial membrane potential (TMRE), which allows discriminating between viable (TMRE+) and apoptotic (TMRE) cells. Apoptosis was evaluated selectively in the NGbright cell population. The percentage of TMRE+ on live β-cells (NGbright) subset was determined based on the gate of TMRE unstained samples.
Cellular Composition Assay
The content of α-, β-, δ- and pancreatic polypeptide cells was determined by laser scanning cytometry (LSC/iCys; CompuCyte, Cambrige, MA), as previously described (15,16). Briefly, dispersed cells were fixed on glass slides with 2.5% paraformaldehyde (Electron Microscopy Sciences, Washington, PA). After incubation with Protein Block (BioGenex, San Ramon, CA) at room temperature (RT) for 30 min to reduce nonspecific binding, cells were incubated at RT for 2 h with the following primary antibodies: mouse monoclonal antibody to C-peptide (1:100 dilution, Abcam Inc., Cambridge, MA), mouse monoclonal antibody to glucagon (1:500; Sigma, St. Louis, MO), rabbit polyclonal antibody to somatostatin (1:500 dilution, Dako North America Inc., Carpinteria, CA), and rabbit polyclonal antibody to pancreatic polypeptide (PP; 1:1000 dilution, Dako). After washing in Optimax Wash Buffer (Bio-Genex, San Ramon, CA), cells were incubated at room temperature for 1 h with Alexa Fluor 488 goat anti-mouse IgG (1: 200 dilution, Molecular Probes, Eugene, OR), Alexa Fluor 647 goat anti-mouse IgG (1:200 dilution, Molecular Probes) antibodies, and 4′,6-diamidino-2-phenylindole (DAPI) (17 μl/ml, Molecular Probes). The percentage of α-, β-, δ-, and pancreatic polypeptide cells was automatically calculated with LSC/iCys software.
Calculation of β-Cell Content Within Islets and Absolute β-Cell Mass
Based on the analysis of immunostaining for endocrine cell markers by LSC/iCys, each parameter was calculated using the formulas:
F1: β-cell content within islets = β-cell/(α+β+δ+PP cell %) × 100 (%)
F2: β-cell mass (βIEQ) = β-cell content within islet (%)× total IEQ
F3: viable β-cell mass (VβIEQ) = β-cell mass × the percentage of TMRE+ on live β-cells (NGbright) (%)
Fluorescein Diacetate (FDA)/Propidium Iodide (PI) Viability Staining
After culture, 50–100 IEQ were transferred to a 5-ml centrifuge tube and settled for 2–3 min. After removal of the supernatant, the settled islets were collected and resuspended in phosphate-buffered saline (PBS) and placed into a 35 × 10-mm petri dish. The islets were stained, in the dark, with 0.46 JJM FDA and 14.34 μM PI. Fifty individual and consecutively stained islets were assessed for percent viability by estimating the ratio of viable (green fluorescence) versus nonviable (red fluorescence) cells using a fluorescent microscope, as described previously (30).
Glucose-Stimulated Insulin Release
To determine the in vitro potency of islets, a static glucose challenge was performed as previously described (15). Briefly, after overnight culture, islets (50–100 IEQ) were incubated in parallel with either 2.8 or 20 mM glucose in culture medium for 2 h at 37°C. At the end of the incubation period, the supernatant was collected for insulin assessment by ELISA (Alpco, Salem, NH). A glucose stimulated insulin index was calculated by dividing the insulin content in the supernatant of the islet aliquots exposed to high glucose to that of the high glucose.
In Vivo Assessment of Islet Potency
Animal procedures were approved by the Institutional Animal Care and Use Committee (IACUC), and performed in the DRI's Pre-clinical Cell Processing and Translational Models Core. Athymic nu/nu (nude) mice (Harlan Laboratories, Indianapolis, IN) were housed in virus/antibody-free rooms in microisolated cages, having free access to autoclaved chow and water. Animals were rendered diabetic via intravenous administration of 200 mg/kg of streptozotocin (Sigma). Nonfasting blood glucose was assessed with a glucometer (OneTouch Ultra2; Life Scan, Milpitas, CA). Mice with sustained hyperglycemia (>300 mg/dl) were used as islet graft recipients. Islet grafts of 2,000 IEQ each were implanted under the left kidney capsule, as previously described (15). Collectively, 41 mice received islet grafts from 33 human preparations processed using collagenase NB1 and 40 mice received islets from 26 human preparations isolated with Liberase enzyme blend. Average percentage of transplanted mice that reverted diabetes per human islet preparation and days required to reverse diabetes were assessed (17).
Statistical Analysis
Data were analyzed using Excel (Windows) and Prism 4.0 (GraphPad) software. Data are shown as mean + SEM. Statistical analyses were performed using methods appropriate to each specific analysis including Student's t-tests for two-sample comparisons of independent groups and Bonferroni correction followed by ANOVA for six-sample comparison. Statistical significance was considered for values of p < 0.05.
Results
Characteristics of Donors
The donor characteristics in each group are shown in Table 2. There was no significant difference in age, gender ratio (male/female), body height, body weight, body mass index (BMI), cold ischemia time (CIT), and pancreas weight between the two groups.
Pancreas Donor Variables

Liberase: Liberase HI collagenase (Roche); NB1: Collagenase blend (SERVA).
Isolation-Related Variables
The islet isolation-related variables in each group are summarized in Table 3. The digestion time in the collagenase NB1 group was significantly longer, when compared with the Liberase group (18.6 ± 0.7 vs. 14.5 ± 0.5 min, p < 0.01). There was no significant difference in the undigested pancreas weight and in the postpurification islet yields between the two groups. There was also no significant difference between the groups in terms of the transplant rate and successful isolation rate (postpurification islet yield: more than 250,000 IEQ) (Liberase vs. NB1: 54.5% vs. 36.8%, p = n.s., 52.9% vs. 41.2%, p = n.s., respectively). However, there were statistically significant differences between the two groups in the post- and prepurification islet particle number (prepurification: 405,965 ± 21,910 vs. 315,178 ± 27,609, p < 0.05; postpurification: 270,986 ± 19,870 vs. 188,731 ± 19,732, p < 0.05, in Liberase and NB1, respectively).
Isolation Variables

IEQ, islet equivalents; PN, particulate number.
The average size of the islets (IEQ/IPN) pre- and postpurification in the Liberase group was significantly smaller than those in NB1 group (prepurification: 1.13 ± 0.07 vs. 1.31 ± 0.10, p = 0.053; postpurification: 1.28 ± 0.10 vs. 1.53 ± 0.10, p < 0.05, in Liberase and NB1, respectively), even though the NB1 group had significantly longer digestion times. The results suggested that enzymatic activity of NB1 might be lower when compared to that of Liberase. However, there were no significant differences between the two groups in the percentage of embedded islets recovered (Liberase vs. NB1: 13.9 ± 1.9 vs. 13.8 ± 2.5, p = n.s.).
Islet Quality
Viability
To examine the effects of the two different collagenase blends on islet quality, islet preparations were assessed using FDA/PI, which has been currently used for clinical trials. There was no significant difference in islet cell viability assessed by FDA/PI between the two groups (Liberase vs. NB1: 87.7 ± 1.1% vs. 90.7 ± 2.1%, p = n.s.). However, fractional β-cell viability, which allows evaluating apoptotic cells as well as dead cells by flow cytometry (Table 4), showed that islets in the Liberase group had significantly higher β-cell viability (the percentage of TMRE+) when compared to the NB1 group (Liberase vs. NB1: 72.0 ± 2.0% vs. 54.5 ± 3.4%, p < 0.05), although both groups had similar percentages of dead cells (7AAD+).
Islet Cell Product Assessment
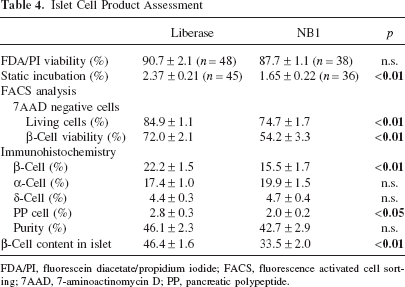
FDA/PI, fluorescein diacetate/propidium iodide; FACS, fluorescence activated cell sorting; 7AAD, 7-aminoactinomycin D; PP, pancreatic polypeptide.
β-Cell Content and Islet Mass
To assess the effects of the two enzyme blends on β-cell content/mass contained in each human islet preparation, we obtained single islet cell suspensions and stained them for pancreatic hormones (Table 4). The β-cell content and β-cell mass (βIEQ) for each islet preparation were calculated. The Liberase group showed significantly higher β-cell content within islets than the NB1 group (46.3 ± 1.6% vs. 33.4 ± 2.0%; p < 0.01). The β-cell mass in the Liberase group was also significantly higher than in the NB1 group (148,451 ± 12,812 vs. 91,351 ± 11,150 βIEQ, p < 0.01), even though there was no significant difference in total islet yield between the two groups. Moreover, there was significant difference between the groups in terms of the viable β-cell mass (VβIEQ), which was most associated with in vivo islet potency (Liberase vs. NB1: 106,274 ± 10,228 vs. 47,317 ± 6,486 VβIEQ, p < 0.01) Fig. 1A-C).

Isolation outcomes. (A) There was no significant difference in postpurification islet yields between the two groups [collagenase NB1, SERVA) versus Liberase: 263,389 ± 21550 versus 323,616 ± 27,192 IEQ (islet eqivalent; n.s.). (B, C) The NB1 group showed significantly lower β-cell mass (93,671 ± 11,150 vs. 148,451 ± 12,812 βIEQ, *p < 0.05) and viable β-cell mass (47,317 ± 6,486 vs. 106,274 ± 10,228 VβIEQ, **p < 0.01).
Islet Potency
In Vitro: Glucose Stimulation Insulin Index
The glucose stimulation insulin index in the NB1 group was significantly lower than in the Liberase group (1.65 ± 0.22 vs. 2.37 ± 0.21, p < 0.01) (Table 4).
In Vivo: Islet Potency in the Diabetic Nude Mouse Model
The average reversal rates of diabetes in transplanted mice in the Liberase and NB1 groups were 81% and 69%, respectively (p = n.s.) (Fig. 2A). Although there was no significant difference in the reversal rate, it took significantly more days to reverse diabetes in the NB1 group than in the Liberase group (p < 0.05) (Fig. 2B).
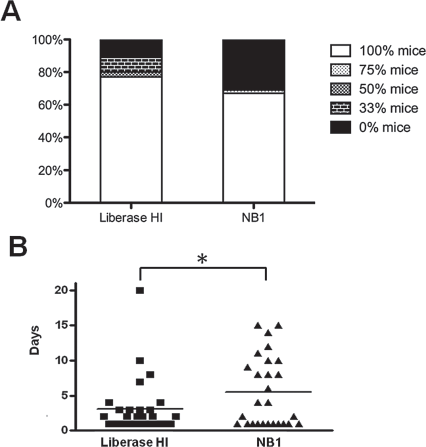
In vivo potency of human islet preparations. (A, B) Average percentage of transplanted mice that reversed diabetes per human islet preparation processed using collagenase NB1 or Liberase HI. The reversal rate in diabetic nude mice transplanted with human islet preparations showed no significant differences (A). The time required for the reversal of diabetes between the experimental groups was significantly longer in the NB1 group than in the Liberase group (B) (p < 0.05).
Discussion
In this study, we have compared the effects of two clinical-grade collagenase blends, Liberase and NB1, on islet yield and β-cell quality in human islet isolations. Although islet yields assessed by DTZ staining were comparable between the two groups, β-cell mass assessed by C-peptide staining in the Liberase group was significantly higher. Assessment of islet cell viability by FDA/PI, which has been the gold standard method used for ongoing clinical trials, did not detect any differences in the viability of islets between the two groups. However, the Liberase group showed significantly higher β-cell-specific viability than the NB1 group when viability was assessed by fluorescence-activated cell sorting (FACS), which allows evaluating both dead and apoptotic cells (15). Moreover, islets in the Liberase group demonstrated significantly better quality islet potency, both in vitro and in vivo. Our results consistently indicated that the quality of islets processed using the collagenase NB1 blend was not as good as that of islets processed using Liberase HI, even through islets yields were comparable. Evaluation of viable β-cell mass contained in human islet preparations will be of assistance for selecting enzyme blends.
Since C. histolyticum collagenase became commercially available in the early 1960s, it has been widely used as a tissue-dispersing enzyme (14,24,34). A variety of collagenases/proteases produced by this technology allows for degrading various types of collagen and gelatin. Therefore, enzyme derived from C. histolyticum is called “crude collagenase” (11). The Liberase HI was introduced in November 1994 as the first dissociation enzyme blend developed to isolate human islets (26,28,36). This product contained purified collagenase (both class I and II) from C. histolyticum and a purified bacterial neutral protease (thermolysin or Dispase®) (28). The development of Liberase HI has dramatically changed human islet isolation (28), contributing to obtaining reproducibly high numbers of islets from large animal pancreata, including human, and establishing human islet transplantation as an option of therapies for patients with type 1 diabetes (41). This has been attributed in part to the activity and purity of the enzyme blend, as well as to its low endotoxin contamination (5). Thus, Liberase HI had been used for clinical islet isolation until it was discontinued due to the potential, albeit low, risk of prion disease transmission. Since then, collagenase NB1 has been utilized as the only enzyme blend available for clinical purposes.
Several groups have reported the comparison between Liberase HI and collagenase NB1 blends in terms of the efficiency of islet isolations yield and islet quality (2,8–10,39). Recently Brandhorst et al. reported that collagenase NB1 is less efficient for pancreas dissociation than Liberase HI, describing that it may be less harmful to pancreatic tissues (8), and that the glucose-stimulated insulin release index and insulin content were significantly higher than in the Liberase group. In our study, we did not observe significant difference in terms of islet yields from human pancreata. In agreement with the previous report, we observed that both β-cell mass and VβIEQ in the NB1 group were significantly lower than in the Liberase group. Furthermore, both in vitro and in vivo islet function in the NB1 groups were significantly lower than in the Liberase group.
One possible explanation in the discrepancy between their report and our data may be related to lot-to-lot variability in the NB1 collagenase blend. In particular, a total of nine different lots of NB1 blend were used in our study and, among them, five were utilized more than four times. Although these data were not conclusive due to the small number of samples, there were significant differences observed in islet yield and β-cell mass (islet yield A: 491,625 ± 70,906, B: 269,765 ± 56,087, C: 257,603 ± 6,048, D: 259,622 ± 38,262, E: 241,012 ± 69,536 IEQ, ANOVA, p = 0.055; β-cell mass A: 193,913 ± 32,620, B: 49,349 ± 13,504, C: 75,779 ± 25,749, D: 103,953 ± 22,491, E: 101,659 ± 37,073 βIEQ, ANOVA, p < 0.01; Bonferroni correction A vs. C, D: p < 0.05). In fact, the highest β-cell mass in lot A was comparable to the one in the Liberase group (n.s.). As others reported (2), our data also showed significantly longer digestion times in the NB1 group. The longer exposure of pancreatic tissues to active enzyme at high temperature (37°C) results in lower islet viability through enzymatic toxicity and hypoxia (29,40). Even though NB1 blend might be less harmful to islet cells, some of the lots tested showed less potency in terms of pancreas dissociation, which exposed the tissue longer to a detrimental environment. Notably, Libease HI has also been reported to have lot-to-lot variability (4,35,43). A large-scale, multicenter study may be needed to assess the impact of lot-to-lot variability of the NB1 blend.
Anazawa et al. recently reported the comparison between Liberase HI and NB1 blends utilized for clinical auto-islet transplantation for patients with chronic pancreatitis (2). They demonstrated that total islet yields with no purification in both groups were similar, and that the percentage of embedded islets was significantly higher in the NB1 group compared to the Liberase group. The purification procedure is not always necessary for auto-islet transplantation unless the volume of whole islet preparation is high, which may increase the risk of intrahepatic thromboembolic events (31). However, in allogeneic islet transplantation, the purification process is a key for successful islet isolation and to reduce the volume of antigenic tissue implanted into the recipients. Even though the purification protocols have been improved in recent years, it still remains difficult to separate embedded islets from exocrine tissue when compared to non-embedded islets (3,17,32). This phenomenon might have contributed to the lower transplant rate registered in the islet isolation processed using NB1 blend. In human islet isolation, purifying islets from other pancreatic tissue had been challenging until the large-scale purification method using COBE 2991 cell processor was reported (1,25). The selection of the purification method or medium might be a possible explanation of the discrepancy among islet processing centers.
Neutral proteases have been recently reported to play an important role in enzymatic digestion (6,7,22,23). Kin et al. reported that the optimization of the neutral protease dosage based on pancreas weight rather than on class II/class I collagenase activity ratio was more crucial in successful islet isolation (23). Furthermore, they developed a pancreas digestion protocol optimized for NB1 enzyme, where only collagenase was injected into the pancreas through the duct, and then neutral protease was added to the circulating system during the digestion phase (22). Liberase HI and NB1 blends have different types of neutral proteases. Little data have been available to date in regards to the effects of neutral proteases on human islet quality and isolation yields. Although neutral protease will be useful for shortening the digestion time through helping the dissociation of pancreatic tissues, it may be toxic for islet cells. However, it may be beneficial for islet cells through the degradation of active collagenase I/II. Further study addressing these issues will be needed.
In conclusion, the present study demonstrated that the utilization of collagenase NB1 blend was associated with significantly decreased β-cell mass, viability, and function when compared to Liberase, even though islet yield was comparable. Collagenese NB1 might be less potent than Liberase in terms of the disintegration of the pancreas, which caused a longer digestion time and eventually exposed islet cells in harsh conditions for a long time. Further understanding of the lot-to-lot variability, of the role of neutral proteases and thermolysin, as well as the optimization and/or selection of isolation procedures based on the type of the utilized enzyme may be of assistance in improving islet isolation outcomes, leading to increased successful islet transplantation.
Footnotes
Acknowledgments
The authors are grateful to the members of the Human Cell Processing Facility, Pre-clinical Cell Processing and Translational Laboratory of the Cell Transplant Center, the Clinical Islet Transplant Program, the General Clinical Research Center, the Imaging Core, the Flow Cytometry Core, and the Administrative Core at the Diabetes Research Institute; and to the Organ Procurement Organizations for the continuous enthusiasm and support to our program. This work was supported in part by NIH-NCRR, GCRC MO1RR16587, NIDDK RO1-DK55347-IU42RR016603, 5R01 DK25802, ICR 5U42RR016603, JDRFI 4-200-946 and 4-2004-361, and the Diabetes Research Institute Foundation (www.DiabetesResearch.org). The authors declare no conflicts of interest.