
Abstract
Bone marrow-derived mesenchymal stem cells (MSCs) are multipotent cells characterized by their self-renewal and differentiation potential. Accumulating clinical and preclinical evidence indicate MSCs are a promising cell source for regenerative medical therapies. However, undesirable immortalization, spontaneous transformation, and tumorigenic potential from long-term cultured MSCs have been reported in human and mouse. We report rat MSCs isolated from young donors could undergo transformation in early passage culture. We aimed to characterize the transformed population and determine their therapeutic effects after intracardiac transplantation in the infarcted myocardium. MSCs were isolated from bone marrow of Lewis rats according to standard protocols and cultured under standard conditions. Phenotype of growing cells was assessed by flow cytometry. Following acute myocardial infarction in rats, cells were delivered by intracardiac injection. Cardiac functions were assessed by pressure–volume loops. Infarction size and pathologic effects were evaluated after 6 weeks. The abnormal colonies were detected in culture as early at passage 3. They were noted to appear as distinctly different morphology from typical MSCs, which changed from a normal elongated spindle shape to a compact abnormal morphology. They exhibited rapid cell proliferation. Some subclones lost contact inhibition of cell division and formed multilayer aggregates. Chromosomal instability was detected. They were devoid of surface markers CD29, CD44, CD90, and CD117. Furthermore, there was no significant improvement on infarction size and cardiac function 6 weeks after cell transplantation. Our study highlights the need for establishment of biosafety criteria in regulating culture-expanded MSCs to achieve the full clinical therapeutic benefits.
Introduction
Mesenchymal stem cells (MSCs) are self-renewing, clonal precursors of nonhematopoietic stromal tissues (6,19). They can differentiate into osteoblasts, neurons, chondrocytes, skeletal myoblasts, and cardiomyocytes under appropriate conditions (5,7,10,14,22). They can be isolated from the bone marrow, adipose tissue, or umbilical cord blood and expanded in culture and proliferate in vitro (4,12,13,20,26). Their excellent proliferation capacity makes culture expansion of MSCs an attractive strategy to generate large number of cells for autologous stem cell therapy (9,19).
However, MSCs expansion may accumulate the deleterious mutations, resulting in spontaneous immortalization and malignant transformation. Indeed, spontaneous transformation of MSCs after expansion culture is reported in adipose tissue-derived human MSCs (16) and bone marrow-derived mouse MSCs (1,11,21,27). The transformed MSCs are associated with phenotypic and genotypic alterations, including rapid cell proliferation and loss of contact inhibition, accumulated chromosomal instability, gradual elevation of telomerase activity, and enhanced c-myc gene expression.
We report that rat bone marrow-derived MSCs in early passage underwent spontaneous transformation, and the therapeutic effects of transformed MSCs on the cardiac function were investigated in a rat left anterior descending (LAD) ligation model after intracardiac injections.
Materials and Methods
Isolation and Culturing of Rat MSCs
Rat MSCs were isolated from the bone marrow of the femurs and tibias of Lewis rats (Charles River laboratory). A 23-gauge needle was inserted into the shaft of the bone, which was flushed with 30 ml of complete Dulbecco's minimal essential medium (DMEM, PAN) containing 10% fetal bovine serum (FBS) (lot selected for promoting rapid expansion of MSCs, Hyclone), 2 mM L-glutamine (PAA), 100 U/ml penicillin (PAA), 100 μg/ml streptomycin (PAA), and 25 ng/ml amphotericin B (PAA). The harvested cells were filtered through a 100-μm nylon filter (Falcon) and plated into one 75-cm2 flask per rat. The cells were grown at 37°C and 5% CO2 for 3 days before the medium was replaced. The adherent cells were grown to 90% confluence to obtain samples here defined as passage zero (P0) cells. All animal work was approved by the local ethics committee and performed under guidelines determined by institutional committees for animal welfare.
Fluorescence-Activated Cell Sorter (FACS) Analysis
MSCs at passages 3, 6, and 9 were analyzed for purity and epitope expression using FACS analysis. The cells were blocked with Fc Block™ Blocking Reagent (BD Biosciences) and incubated for 10 min at 4°C with the following antibodies: anti-CD29 (BD Bioscience), anti-CD44 FITC (Chemicon), anti-CD90 (Thy1) FITC (Clone MRC OX-7, Abcam), anti-CD117 (Santa Cruz). For CD29 and CD117 staining following primary antibody incubation, a secondary antibody Alexa Fluor 488 conjugated (Molecular Probes) was applied for 10 min at 4°C. Isotype controls were purchased from BD Pharmingen. After incubation, the cells were washed with 2 mM phosphate-buffered saline (PBS)/EDTA and analyzed using a FACS Calibur flow cytometer (Becton Dickinson). Dead cells were excluded using propidium iodide (PI) staining. Data analysis was performed with BD CELL Quest software. Histograms of cell number versus logarithmic fluorescence intensity were recorded for 10,000 cells per sample.
Analysis of Chromosome Number
Twenty-four hours after medium change subconfluent cell cultures were prepared for the cytogenetic analysis. Colcimid (20 μl) were applied to the cultures for approximately 2 h in order to block microtubular formation. Following vortexing and centrifugation cells were incubated with 10 ml hypotonic potassium chloride for 8 min at 37°C for metaphases processing. Cell suspensions were subsequently fixed, dropped on precooled slides, air dried, and observed by phase contrast microscope in order to assess quality and quantity of mitoses. Chromosome number of metaphases was analyzed following Giemsa staining.
Metabolic Analysis
Representative parameters for cell metabolism were measured with the Bionas® 2500 analyzing system. Normal MSCs and abnormal MSCs were cultured on chips in DMEM with 10% FBS at the density of 3 × 104 cells/chip. Measurements were stably collected for 24 h using running medium (DMEM, 100 U/ml Pen/Strep, 0.1% FBS) and subsequently for 2 h in running medium with 0.2% Triton X-100. Acidification and respiration activity as well as cell impedance were assessed. All the experiments were run in duplicate.
Cell Labeling
To identify the transplanted MSCs in the implanted hearts, the cells were labeled with bromodeoxyuridine (BrdU) (Sigma Aldrich) 2 days before transplantation. The harvested cells were resuspended in cell culture medium at a density of 3 × 106 per 100 μl and kept on ice (less than 1 h) until transplantation into the myocardium. BrdU labeling efficiency was confirmed by immunostaining with anti BrdU monoclonal antibody (Sigma Aldrich).
In Vivo Tumorigenesis
MSCs actively growing in culture were isolated, washed, and resuspended in PBS and viable cells were counted. Cells (3 × 106) were injected intravenously into BALB/c athymic (nude) male mice (4–6 weeks, Charles River) (n = 6). After 1 month, mice were sacrificed by overdose of Ketamine. Organs including heart, lungs, liver, kidneys, and brain were harvested and embedded in Tissue-Tek O.C.T. compound. Frozen sections (5 μm in thickness) were prepared and stained with hematoxylin and eosin. Two professional pathologists were employed to investigate tumorigenesis.
Myocardial Infarction and MSCs Transplantation
All animals received humane care in compliance with the Guide for the Care and Use of Laboratory Animals (NIH Publication No.85–23, revised 1996). Male Lewis rats were obtained from Charles River. Myocardial infarction was induced at 8–12 weeks of age (approximately 280 g body weight) in 26 animals. Rats were anaesthetized by IP injection with pentobarbital (50 mg/kg body weight, Roche), endotracheally intubated, and mechanically ventilated. The heart was exposed via a left thoracotomy and the left anterior descending coronary artery was ligated permanently with a 6-0 silk suture (MI). In the sham group (n = 11), rats were sham operated (left thoracotomy without coronary artery ligation; SHAM). Successful infarction was determined by observing a pale discoloration of the left ventricular muscle and an ST elevation on electrocardiograms. Following the operation, 6 × 106 transformed MSCs were harvested by trypsin, resuspended in 200 μl PBS, and injected at six injection sites into anterior and lateral aspects of the viable myocardium bordering the infarction with a 31-gauge needle (BD Bioscience). Animals were sacrificed at 6 weeks after cell transplantation. Hearts were excised, rinsed, and embedded in paraffin blocks. Subsequently, sections of 5 μm thickness were prepared from the entire heart.
Histological Analysis
Paraffin sections (5 μm in thickness) were prepared and stained with Sirius red (Division Chroma, Muenster, Germany)/Fast green (Sigma-Aldrich) or hematoxylin and eosin. From every heart, three slices per level in eight different levels within the length of the whole organ were used for measurement of scar size.
Determination of Infarct Size
Heart tissue sections were stained with Fast green FCF and Sirius red. The infarct area with an increase in collagen content was shown as Sirius red positive and was measured using computerized planimetry (Axio Vision LE Rel. 4.5 software; Zeiss, Jena, Germany). The final infarct size was determined as percent of the whole area of the left ventricular section. Two investigators blinded to the experimental groups performed the analysis.
Immunostaining
For immunohistological detection of transplanted cells, paraffin sections were incubated with monoclonal mouse anti-BrdU (Sigma Aldrich). After blocking in Envision blocking buffer (Dako), sections were placed in primary antibody overnight at 4–8°C. On the following day, the sections were incubated with Alexa-488 (Molecular Probes) conjugated goat anti-mouse IgG. Nuclei were also counterstained with PI (Molecular Probes).
Left Ventricular Catheterization
Pressure–volume loops (P/V loop) were recorded under pentobarbital anesthesia (50 mg/kg body weight, Roche). Data were collected with the Millar Pressure–Volume System Ultra-Miniature Pressure–Volume Catheter (model SPR-838), Millar Pressure Conductance Unit (model MPCU-200), and Millar PowerLab data acquisition hardware (EMKA Technologies, Paris, France). Calibration of pressure and volume was performed by equating the minimal and maximal conductances with minimal (0 mmHg) and maximal (100 mmHg) pressures as well as minimal and maximal blood volumes received from venous circulation. After inserting the catheter into carotid artery retrograde access to the LV was achieved. Volume signal was corrected by measurement of wall conductance (parallel volume; Vp) via hypertonic saline (5%) injection. P/V loops of the LV were recorded under normal conditions (baseline) followed by stress conditions mediated by intravenous dobutamine administration (10 μg/kg/min, Sigma-Aldrich).
Statistical Analysis
All values are presented as mean ± SD. Statistical analyses were performed using Sigma Stat software version 3.0 (SPSS Inc., Chicago, USA). One-way ANOVA with Scheffe's post hoc test for unequal samples sizes was used to compare numeric data between the four experimental groups. A level of p < 0.05 was considered as significantly different.
Results
Surface Markers of Abnormal MSCs Is Different From Normal Mesenchymal Stem Cells
Cell isolation, expansion, and characterization of rat bone marrow MSCs have been established according to previous reports (17). Primary culture of the marrow cells was performed according to Dexter's method (3, 10). Due to the presence of very little extracellular matrix in the bone marrow, gentle mechanical disruption can readily dissociate the stroma and hematopoietic cells into a single cell suspension. When plating the cells at low density, the MSCs adhere and can be easily separated from the hematopoietic stem cells (HSCs) by repeated washing. Figure 1A shows the morphology of normal rat MSCs from bone marrow at day 10. The cells displayed a homogenous elongated spindle-shaped population and maintained a similar shape during the subsequent passages. Abnormal MSCs colonies were detected at passage 3. They had a compact morphology. Some subclones lost contact inhibition and formed multilayer aggregates (Fig. 1B, C). The surface molecule expression of two populations showed different phenotype. Both MSC cultures were devoid of CD34 and CD45 hematopoietic cells (data not shown). Normal MSCs were highly positive in CD29, CD44, and CD90 and moderate in CD117 (Fig. 2A). Abnormal MSCs were devoid of typical MSC markers (Fig. 2B).

Characterization of rat MSCs. (A) Morphology of normal MSCs cultured in primary culture at day 10. They display spindle shaped morphology. (B, C) Morphology of abnormal MSCs at passage 3. Scale bar: 200 μm.

Immunophenotypic profile of rat MSCs. (A) Normal rat MSCs. (B) Abnormal rat MSCs. Flow cytometry histograms show the expression of selected surface molecules CD29, CD44, CD90, and CD117. Control cells labeled without primary antibodies.
Chromosomal Aberration Was Detected From Abnormal MSCs
Abnormal MSCs were analyzed for chromosomal number. Alterations in the normal number of chromosomes were detected (Fig. 3A). The abnormal MSCs exhibited a very wide range of chromosome numbers, from 49 up to 221 with an average of 90 (Fig. 3B), which is considerably different from normal rat chromosomal number 42 (27).

Chromosome number analysis of abnormal rat MSCs. The number of chromosomes in each of 51 cells was counted. The normal rat karyotype has 42 chromosomes in each cell (original magnification 600×).
Abnormal MSCs Show Accelerated Metabolism Compared to Normal MSCs
Metabolic features were determined by culturing normal and abnormal MSCs on chips with Bionas® 2500 analyzing system (Fig. 4A–D). Abnormal MSCs showed distinctly higher acidification activities than normal MSCs (Fig. 5A). The increased acidification rate corresponded with their oxygen consumption behavior. In comparison with normal MSCs the respiration rate of abnormal MSCs was particularly elevated (Fig. 5B). More oxygen was metabolized by abnormal MSCs compared to normal MSCs. Abnormal MSCs showed lower impedance signal than normal MSCs. Therefore, cell adhesion or cell density in the abnormal MSCs seeded chip was higher than the normal MSCs seeded chip (Fig. 5C), indicating a rapid proliferation of abnormal MSCs. An increased cell density of abnormal MSCs is also visible from Figure 4C and D.
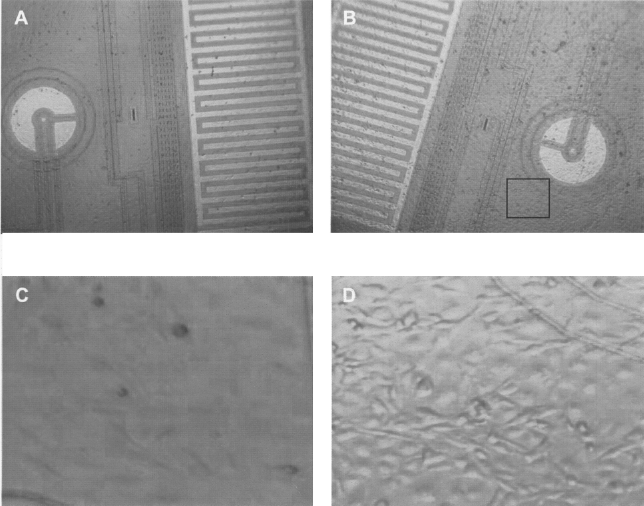
Representative images of cells on chips. Normal MSCs (A, C) and abnormal MSCs (B, D) on the chips 24 h after seeding. Original magnification (A, B): 50×; (C, D): 300×.

Detected signals of metabolic activities by Bionas® 2500 analyzing system. (A) Acidification activity. (B) Oxygen consumption. (C) Nonstandardized rates of cell impedance.
Cell Engraftment with Abnormal MSCs in the Infarcted Heart
Abnormal MSCs (6 × 106) were transplanted into the six sites of the viable LV myocardium bordering the infarction after LAD ligation (n = 6). The assessment of cell engraftment was carried out 6 weeks after cell transplantation. BrdU-labeled cells were detected in both the infarcted area and the border zone (Fig. 6A–C). There was no evidence for MSC differentiation into bone, adipose, and cartilage 6 weeks after cell transplantation (data not shown).

Immunohistological staining of infarcted rat myocardium following MSCs injection using monoclonal antibodies against BrdU. (A, B) Six weeks after transplantation, sections near the infarct zone were double-stained for nuclei (PI staining) and BrdU (A: Alexa-488 labelled). (C) Merged image of double staining of sections for BrdU and nuclei. Scale bars: 200 μm.
Infarct Size and Cardiac Function
LAD ligation consistently resulted in transmural myocardial infarction, exhibiting typical histological changes including thinning of the left ventricular free wall and extensive collagen deposition 6 weeks after myocardial infarction. Representative left ventricular sections 6 weeks following LAD ligation with PBS (n = 14) or transformed MSC injection (n = 6) are shown in Figure 7A and B. The average infarct size was 24.03 ± 1.58% in abnormal MSC-treated hearts and 23.89 ± 1.12% in MI hearts as determined by computerized color analysis of the Sirius red-stained sections. The difference was not statistically significant (p = 0.99) (Fig. 7C). Cardiac function, which was estimated by ejection fraction, cardiac output, stroke work, and stroke volume, was not improved significantly in the transformed MSC group compared to the MI group (p > 0.05) (Fig. 8), indicating that abnormal MSCs did not restore the performance of the infarcted hearts. On the contrary, normal MSCs ameliorated functionality after MI (Fig. 8).

Physiological effects of abnormal rat MSCs. Sirius red staining of transverse sections through rat hearts 6 weeks following ligation of the LAD coronary artery. (A, B) Representative left ventricular sections 6 weeks following LAD ligation with PBS, abnormal rat MSCs injection. Thinning of the left ventricular free wall and extensive collagen deposition (red) in scar tissue is noted. Scale bars: 2 mm. (C) On average, there is no significant difference between the scar size in hearts of abnormal MSCs-treated animals and in those of animals without cell treatment.

Functional effects of abnormal rat MSCs. Effects of abnormal rat MSCs transplantation on hemodynamic parameters. Values are means ± SEM (*p < 0.05).
There Was no Tumor Formation in Nude Mice After the Intravenous Injection of Abnormal MSCs
Four weeks after IV cell injection into the nude mice (n = 6), organs including heart, lungs, liver, kidneys, and brain were analyzed for tumorigenesis. No tumor was observed in all the analyzed slides (Fig. 9). A diffuse alveocyte desquamation was observed in all animals (Fig. 9A, B). All animals survived 4 weeks after abnormal MSCs injection.

Absence of tumor formation in nude mice. (A) Alveolar collapse following injection of abnormal MSCs. Scale bar: 200 μm. (B) Desquamation of alveoli. Scale bar: 100 μm. (C) Heart. (D) Liver. (E) Brain. (F) Kidney. Representative sections of organs harvested 1 month after injection (n = 6). Scales bars (C–F): 200 μm.
Discussion
We have demonstrated that under the described culture conditions, bone marrow-derived rat MSCs in early passage culture may undergo spontaneous transformation. Inheritable changes in cells were observed, as manifested by changes in chromosomes number and alterations in proliferative features and cell surface properties. These results were observed independently by three researchers working 2 years apart. Therefore, the idiosyncratic effects of a particular lot of serum in culture medium as the possible reason to induce the transformation can be excluded.
The resulting clones showed chromosomal instability by passage 3 and lost some characteristics of phenotype of MSCs. We observed the wide variation in chromosome number, which indicates chromosome instability and may contribute to cancer initiation. Consistently, the analysis of their metabolism detected an atypical increased rate of proliferation. It is still not clear whether the increase of chromosome number that occurred is due to cell fusion or chromosome replication. In fact, there is conflicting evidence: the fusion of mouse bone marrow-derived cells with host cells (2,23,24) and the fusion of human MSCs with cocultured epithelial cells (18) were reported; Zhou et al. (27) did not detect the fusion. This issue needs to be further addressed.
Zhou et al. (27), Tolar et al. (21), and Aguilar et al. (1) found bone marrow-derived mouse MSCs showed cytogenetic aberrations after several passages in in vitro culture. We also found that rat MSCs showed chromosomal instability after three passages. However, in our study, no sarcomas were detected 4 weeks after IV infusion of transformed rat MSCs into nude mice. This is different from the reports that 3 weeks after IV infusion transformed mouse MSCs induced malignant sarcomas in immunodeficient mice (1,11,21,27). Recent study from Li et al. (8) could be one of the explanations for this discrepancy, which suggested that transformed MSCs might restore a nonmalignant phenotype after fusion with host cells. It is important to further address how the cytogenetic aberrations acquired in culture correlate with tumor initiation and progression in vivo.
We also noted several recent reports indicating that spontaneous transformation of MSCs could occur on both bone marrow-derived mouse MSCs and adipose tissue-derived human MSCs (11,16,27). Hence, this phenomenon cannot be regarded as a casual phenomenon. Exploration of the genetic alterations and molecular mechanisms underlying the transformation may shed new light on regulating the process of ex vivo expansion of MSCs, which ensures their sustainable propagation without alterations in their genetic traits and functional degeneration.
The clinical importance of this study is related to the clinical trials that administrate human MSCs to patients with ischemic cardiovascular diseases for regenerating cardiac functions. The present study showed that transplantation of transformed MSCs into the infarcted hearts revealed no cardiac function improvement as characterized by infarct size, ejection fraction, cardiac output, stroke work, or stroke volume from left ventricles of the rats. Further, ex vivo expansion of human MSCs may induce the transformation and increase the risk of cancer formation after transplantation. The present study strengthens the established notion that standardized protocol for phenotypic and genotypic characterization of MSCs expanded ex vivo will be indispensable for the efficacy and safety considerations in clinical applications (15, 25). Hence, systematic characterization, standardized, rigorously tested protocol, and quality control are highly valued.
Conclusion
In summary, we have confirmed that expansion culture of bone marrow-derived rat MSCs may induce their immortalization and spontaneous transformation. The transplantation of transformed MSCs into infarcted hearts has no therapeutic effect on the cardiac functional improvement. Development of Good Manufacturing Practice (GMP) compliant culture conditions for MSCs will be of primary importance.
Footnotes
Acknowledgments
This work was supported by the German Helmholtz Association, Mecklenburg-Vorpommern (Nachwuchsgruppe Regenerative Medizin Regulation der Stammzellmigration 0402710), German Federal Ministry of Education and Research (BMBF), BioChancePlus program (0313191), German Research Foundation, Sonderforschungsbereich/Transregio 37, B5, B2, and A4, START-MSC (project 6: Kardiovaskuläre Differenzierung und Applikation definierter mesenchymaler Stammzellpopulationen), Miltenyi Biotec and Steinbeis Transfer Zentrum fuer Herz-Kreislaufforschung, Rostock, Germany. This study was part of the thesis of D. Furlani submitted in fulfillment of the requirements for the degree of Doctor of Philosophy at the University of Rostock (Germany). Authors wish to thank Professor Horst Nizze and Dr. Ulf Titze for their histological analysis, Ms. Sabine Drechsler and Ms. Miriam Nickel for the metabolic assays, and Ms. Saskia Hühns and Ms. Margit Fritsche for technical assistance.