
Abstract
BACKGROUND:
Return-to-work (RTW) is often viewed as an important outcome following acquired brain injury (ABI) and spinal cord injury (SCI), although not all individuals have vocational goals and many experience barriers to RTW.
OBJECTIVE:
This study investigated the relationship between RTW and psychosocial functioning at 12-months post-discharge after ABI and SCI and examined patterns of RTW according to perceived need for and receipt of vocational support.
METHODS:
A file audit was conducted for 69 participants with ABI (n = 44) and SCI (n = 25). Data on employment status and perceived vocational support at 3- and 12-months post-discharge, home and community participation, psychological distress, and health-related quality of life were extracted.
RESULTS:
Individuals in paid employment at 12-months post-discharge (22%, n = 15) reported significantly better psychosocial functioning at this timepoint compared to those not employed (78%; n = 54). For those not employed, three subgroups were identified: 1) Did not perceive the need for or receive vocational support (50%; n = 27); 2) Perceived vocational support needs were unmet (19%; n = 10); and 3) Perceived and received vocational support (31%; n = 17). Psychological distress was highest for those who perceived and received vocational support but were not employed.
CONCLUSION:
RTW was associated with better psychosocial functioning after acquired neurological injury. The findings highlight the need for clinicians to explore and revisit individuals’ perceived need for and preferences for vocational support and monitor the psychological well-being of those with RTW goals that are not yet successful.
Keywords
Introduction
Returning to work is a priority for many individuals after an acquired neurological injury such as acquired brain injury (ABI) or spinal cord injury (SCI). Resuming employment or education can represent a major milestone for community reintegration, promoting a renewed sense of belonging, self-worth, and identity [1–3]. Yet, rates of unemployment for people with ABI and SCI are typically high (i.e., 40–60%) [4–6], and many barriers to work re-integration have been identified [7–11].
Biopsychosocial frameworks highlight that a complex interplay of factors is likely to influence return-to-work (RTW) after neurological injury, including injury-related characteristics, pre-injury, psychological, and socio-environmental factors [12, 13]. The influence of medical and injury-related factors on post-injury employment outcomes has been extensively investigated after ABI [14–18] and SCI [18–20]. In general, longer inpatient length of stay and more severe and global disability are associated with poorer RTW outcomes [6, 21–23]. The presence of multiple impairments or comorbid medical and psychiatric complications are also associated with reduced likelihood of post-injury employment [6, 25]. Demographic factors such as age, ethnicity, and education have been found to influence RTW outcomes following neurological injury in some studies, with higher educational attainment [6, 26–29], younger age at injury onset [7, 28–30], and non-minority ethnicity [7, 30] associated with greater likelihood of RTW. Further, individuals in partnered relationships prior to injury [18, 32], and males [7, 33] have been found to have better RTW outcomes in some studies. However, the findings are generally mixed for demographic characteristics [11, 34].
The influence of pre-injury employment on RTW is well-documented, with studies indicating that individuals employed at the time of injury typically have better RTW outcomes than those not employed [7, 32]. This may particularly be the case for those previously employed at a full-time capacity and returning to the same employer [18]. More variable findings are evident for pre-injury occupation level, regarding the RTW outcomes of individuals engaged in managerial versus non-managerial working roles [14, 35]. The findings of some ABI studies suggest that individuals engaged in managerial and professional roles take longer to RTW and face greater barriers, potentially due to the greater cognitive, language, and interpersonal skills required in these professions and the need for retraining [24, 36]. However, a recent review identified that individuals with ABI with higher professional qualifications, or those returning to professional, managerial, or skilled work roles, typically had better job retention than manual workers [35]. In the SCI population, individuals with higher levels of education or professional qualifications have been found to experience better RTW outcomes, which may be related in part to fewer physical demands associated with administrative and clerical work [37, 38].
In comparison to pre-injury and injury-related characteristics, a smaller body of literature has evaluated the influence of socio-environmental factors, including access to vocational rehabilitation, on RTW outcomes following neurological injury. Vocational rehabilitation refers to a managed process aimed at supporting people to obtain, return to, or maintain, meaningful vocational activity after injury or illness. This process often entails assessment of a person’s vocational needs, readiness and goals and the provision of individualised assistance to enable vocational goal achievement [39, 40]. Other services within vocational rehabilitation include assessment of functional capacity and aptitude, work-related education, vocational guidance or counselling, work preparation (e.g., work experience and retraining, or RTW planning and worksite assessment), job seeking assistance, and supported placement. Such support may not be limited to focusing on paid work, but also include other meaningful vocations such as education or study and volunteering [41]. Support to RTW may be provided by specialist vocational rehabilitation services for ABI or SCI, and/or from disability employment services or general employment services. Although often commencing early post-injury through specialist rehabilitation services, vocational rehabilitation is often viewed as a complex, multi-step process that may entail a range of professionals (e.g., job coaches) and employment support services provided over a long-term timeframe after injury [39, 41].
In general, early engagement in vocational rehabilitation has been found to be associated with better employment outcomes [28], irrespective of the injury type (e.g., ABI or SCI) [21], and several studies have highlighted the benefits of vocational interventions for improving RTW outcomes [19, 42–44]. Yet, a longitudinal study of RTW outcomes following ABI (n = 137) found that more intensive, or extensive engagement with vocational support services was associated with delays in RTW, after controlling for comorbidity and degree of cognitive impairment [24]. Hence, there is a need to better understand the role of vocational support in the RTW process.
Few studies to date have examined individuals’ perceptions of their vocational support needs following acquired neurological injury, which may influence their motivation and engagement, and subsequent RTW outcomes. In a recent study on factors influencing employment outcomes after SCI, Borg [20] identified that perceptions of unmet need and workplace challenges following RTW negatively impacted work re-integration, job satisfaction, and ultimately, employment sustainability. Thus, personal expectations about returning to work and attitudes towards employment may influence post-injury employment outcomes. Reviews have similarly identified the impact of attitudinal factors such as optimism, hope, positive expectations, motivation, and achievement orientation on RTW outcomes after ABI [3, 46] and SCI [3, 47–49]. The importance and personal meaning attached to work roles also appears to have a significant impact on post-injury employment outcomes [3, 46]. Similar psychological factors have been linked to employment sustainability [50], suggesting that these are potentially modifiable targets for intervention in vocational rehabilitation after acquired neurological injury [3, 46].
The focus on vocation-related goals often begins in the inpatient environment in the weeks and months following injury [21, 52]. Advocating for early vocational intervention, McLennan [53] emphasised the importance of maintaining the pre-injury occupational bond between individuals and their employers for enhancing positive expectations of successful and timely RTW. However, for individuals unable to resume their former employment positions soon after discharge, ongoing access to vocational rehabilitation and support to explore and pursue alternative roles and re-training may be necessary. Importantly, such support should match individuals’ perceived need for, and goals related to employment [50, 53].
Returning to work may signal broader community reintegration success and have multiple benefits for people’s health-related quality of life (HRQOL) and well-being [53, 54]. A meta-synthesis by Stergiou-Kita [45] identified that RTW after brain injury provided a sense of normality, structure, purpose, and contribution, in addition to supporting economic independence. Work also represented a valued social outlet, social status, and avenue for reconciling a new identity. Accordingly, several studies have identified links between employment status, psychological well-being [3, 55], and HRQOL [55, 56] following acquired neurological injury. Although the direction of these relationships is often unclear, it seems likely that RTW within the first 12-months post-discharge would be associated with better psychosocial functioning, such as greater independence in the home and community, lower psychological distress, and better HRQOL. However, RTW is not always a feasible or current goal for all individuals and can have detrimental effects on psychosocial functioning if the work is perceived to be highly stressful, lacking in personal meaning, or incompatible with one’s interests and capabilities [3, 57]. Therefore, the match between perceived vocational support needs and support received and relationship to psychosocial functioning is important to understand.
Study aims and hypotheses
Despite early intervention models highlighting the importance of timely access to vocational rehabilitation, relatively few studies have examined individuals’ perceived need for and receipt of vocational supports during the community re-integration process [25, 58]. Greater understanding of unmet vocational support needs for people with acquired neurological injury would help to tailor early vocational support services. The focus of the current study was on vocational rehabilitation or support to return to paid employment or study/education. The first aim was to identify the rates of RTW after ABI and SCI at 3-months and 12-months post-discharge. The second aim was to examine associations between employment outcome and psychological distress (depression, anxiety, and stress), HRQOL, and home and community participation at 12-month post-discharge. It was hypothesised that individuals who had returned to work by 12-months post-discharge would report lower levels of psychological distress, and greater HRQOL and home and community participation. The third aim was to examine patterns of RTW according to the perceived need for and receipt of vocational support at 12-months post-discharge. It was hypothesised that individuals employed at 12-months post-discharge would be more likely to report having their vocational rehabilitation and support needs met (i.e., perceived support needs matched support received) than those not employed.
Methods
Participants and setting
A file audit was conducted on data previously collected as part of a broader project examining transitions of care, service access, and rehabilitation outcomes (Trajectories of Rehabilitation across Complex Environments [TRaCE] 2.0) [59, 60]. Adults with an acquired neurological injury were recruited from the inpatient Brain Injury Rehabilitation Unit (BIRU) and Spinal Injuries Unit (SIU) at the Princess Alexandra Hospital, a tertiary referral and trauma centre in Queensland, Australia, between July 2019 and March 2020. BIRU and SIU are components of the respective specialist ABI and SCI rehabilitation services continua of care, which provide integrated services across inpatient rehabilitation, day rehabilitation and/or specialist outpatient clinics, and community-based transitional rehabilitation and outreach services [61, 62]. Common to all services is specialist clinical expertise in SCI or ABI rehabilitation and a person-centred approach focused on aligning rehabilitation with personal values and goals. All services have the capability to address a range of RTW issues identified by people with ABI and SCI within their programs. Dedicated specialist vocational rehabilitation services are provided for people with SCI through the Back2Work [53] early intervention vocational rehabilitation (EIVR) program during inpatient rehabilitation in the SIU and in the community following discharge and, for people with ABI who identify RTW as a current goal, through the Acquired Brain Injury Transitional Rehabilitation Service (ABITRS) [41]. However, post-discharge pathways typically vary, with some clients receiving post-hospital rehabilitation through their local health-based service provider or a private provider (e.g., via insurance funding); the timing, nature and intensity of this service provision is variable.
Participants in the current study were recruited just prior to discharge from BIRU (inpatient) or SIU and were administered a baseline survey (conducted in-person) and follow-up surveys via telephone, at 3- and 12-months after discharge from inpatient rehabilitation. At each timepoint, the typical follow-up procedure entailed up to three attempts at contact, primarily by telephone with messages left, as well as via email or postal mail. If the participant or a caregiver were not contactable, or responded to indicate that the participant was unwell or deceased, no further contact was made. Inclusion criteria were: (1) a new medically confirmed diagnosis of ABI or SCI; (2) capacity to provide informed consent as determined by a medical practitioner, or consent provided by a guardian / substitute decision maker on behalf of the individual; (3) were aged 18–65 years at the time of study consent and not retired at time of injury. The exclusion criteria comprised: (1) patients readmitted to BIRU or SIU for reasons other than rehabilitation for a newly diagnosed ABI or SCI; (2) patients did not complete relevant survey measures at 3- and/or 12-months; (3) patients were older than 65 years at the time of discharge or were retired at the time of their injury.
Ethical considerations
Ethics approval was obtained from the Metro South Hospital and Health Service (MSHHS) Human Research Ethics Committee (HREC) (HREC/2019/QMS/50271) and Griffith University Human Research Ethics Committees (2019/456). Informed consent was obtained from all participants or their substitute decision-makers.
Measures and outcomes
Demographic and injury-related data were obtained from hospital administrative records. During the discharge assessment, participants completed the Depression Anxiety Stress Scales-21 (see 2.3.5) and provided information on their pre-injury employment. The following measures were administered at 3-months and 12-months post-discharge in the context of a larger assessment battery.
Vocational outcomes survey
A brief vocational outcome survey was purposively designed by the TRaCE project steering committee, comprised of senior rehabilitation clinicians and researchers, to represent the needs of both target populations. This survey initially asked participants about paid employment since discharge from inpatient rehabilitation (survey given at 3-months follow-up) or since the last assessment at 3-months post-discharge (survey given at 12-months follow-up). If participants had worked in paid employment, they were asked to indicate the nature of their employment in terms of status (e.g., full-time/part-time/casual), employer (e.g., same or different from pre-injury), hours worked (e.g., same, more, or less than pre-injury), and duties (e.g., same, slightly different, completely different from pre-injury). If participants had not been in paid employment, they were asked to indicate the primary reason they were not working (e.g., the injury, other illness, decided to retire, redundancy, no suitable job available, lack of assistance in returning to work, etc). Participants were also given the opportunity to provide additional reasons or clarify reasons for not working, which were recorded in note form by the researchers.
Needs and Provision Complexity Scales (NPCS)
The NPCS is a 15-item self-report measure developed to assess perceptions of met and unmet support need amongst individuals with complex neurological disabilities, such as ABI and SCI [63]. Perceptions of required support needs and receipt of support are evaluated across six domains: healthcare, personal care, rehabilitation, social and family support, equipment, and accommodation. The NPCS is administered in two parts, Part A assesses participants’ perceived level of need and Part B assesses participants’ corresponding level of perceived support received. For the current analysis, only the vocational support data were analysed as part of the rehabilitation domain. For vocational support needs, participants were asked whether they required any vocational support to return to part-time or full-time work or education (Yes/No). If yes, they were asked to indicate the type of support based on the following response options: 1) work-related/education assessment/advice; 2) ongoing work-related education and support; and 3) formal vocational programme, e.g., work preparation, work retraining, supported placements. For vocational support received, participants were asked whether they received support (Yes/No) to return to part-time or full-time work or education, and to indicate the type of support received (response options 1–3, as above).
Mayo-Portland Adaptability Inventory (MPAI-4) –Participation index
The MPAI-4 is a 29-item measure developed to assess functioning across a range of physical, cognitive, emotional, behavioural, and social domains [64]. Although developed for people with ABI, the 8-item Participation Index was deemed suitable for people with SCI due to its broad focus on home and community participation in the post-acute period after hospital discharge. The items include: initiation (getting started on activities without prompting), social contact (friends, work associates, and other people who are not family, significant others, or professionals), leisure/recreational activities, self-care (eating, dressing, bathing, hygiene), residence (responsibilities of independent living and homemaking), transportation, employment (paid employment or other employment), and money management (e.g., shopping, banking, personal income and asset management). As part of the employment item, individuals were asked if paid employment or other “constructive, role appropriate activity” (e.g., caregiving, volunteering) was their primary desired social role [56]. Using the self-report version, participants rated items on a five-point rating scale ranging from 0 to 4, where 0 represents completely independent functioning (e.g., Independent; living without supervision or concern from others) and 4 represents very impaired (e.g., No or rare participation or requires extensive assistance or supervision from others [more than 75% of the time]). Accordingly, lower MPAI participation scores signify better home and community participation. Internal reliability of the MPAI was good (α= 0.85).
EQ Visual Analogue Scales (VAS)
The EQ VAS is a self-report scale assessing HRQOL [65]. Using the telephone-administered version, participants were asked to picture in their mind a vertical scale that looks like a thermometer and to indicate the point on the scale that best reflects their current health status, by providing a rating of 0 (indicating ‘worst health you can imagine’) to 100 (indicating ‘best health you can imagine’). The EQ VAS has previously been utilised as a measure of global HRQOL in individuals with ABI [66] and SCI [67].
Depression Anxiety Stress Scales (DASS-21)
The DASS-21 is a self-report measure used to assess psychological distress [68]. The 21 items comprise three subscales: Depression (e.g., “I felt that I had nothing to look forward to”), Anxiety (e.g., “I was aware of dryness of my mouth”) and Stress (e.g., “I found myself getting agitated”). Participants responded to each item via a 4-point rating scale ranging from 0 (Did not apply to me at all) to 3 (Applied to me very much or most of the time). Scores were summed for each subscale and multiplied by two to produce a total score for each subscale, with higher scores indicating greater depression, anxiety, and stress. The DASS-21 has been validated for use in ABI [69] and SCI populations [70]. The DASS-21 showed adequate internal reliability (Depression α= 0.93; Anxiety α= 0.74; Stress α= 0.88).
Statistical analyses
An initial comparison of demographic and injury-related factors associated with employment outcomes at 12-months post-discharge was conducted using independent-samples t-tests and chi-square tests. To investigate the first hypothesis, analyses of covariance (ANCOVAs) were conducted to compare levels of psychological distress, HRQOL, and home and community participation between participants who were employed and those not employed at 12-months post-discharge, after controlling for relevant covariates. Effect sizes are reported based on Cohen [71]. For t-tests, Cohen’s d was interpreted using the following criteria: small effect = 0.20; medium effect = 0.50; large effect = 0.80. For ANOVA, partial eta squared (ηp2) was interpreted using the following criteria: small effect = 0.01; medium effect = 0.06; large effect = 0.14. For the second hypothesis, perceived vocational support needs and receipt of support based on the NPCS data were summarised and tabulated for the employed and unemployed cohorts at the 3- and 12-month timepoints. Participants were classified as having their vocational needs met if their overall perceived need for vocational support (Yes/No) aligned with support received (Yes/No). A chi-square test was used to examine whether the proportion of individuals with vocational needs met varied according to employment status (employed vs not employed at 12-months post-discharge).
Results
Sample characteristics
As shown in Fig. 1, a total of 261 individuals with ABI and SCI were screened for eligibility over the 9-month period (July 2019 –March 2020), and 102 were not eligible. Of those eligible (n = 159), 31 declined and 30 were missed or not able to be recruited or assessed in time prior to discharge. Ninety-eight participants (ABI n = 56; SCI n = 42) provided informed consent and completed the discharge assessment. Thirteen of these participants were lost to follow-up at 3-months post-discharge, and a further seven were excluded due to lack of data on the NPCS. Nine additional participants were lost to follow-up at 12-months post-discharge. A comparison of participants retained at 12-months (n = 69) and those either lost to follow-up or lacking NPCS data (n = 29) identified no significant differences in demographic or injury characteristics, functional independence at discharge, or levels of home and community participation, HRQOL and psychological distress at discharge (p > 0.05).
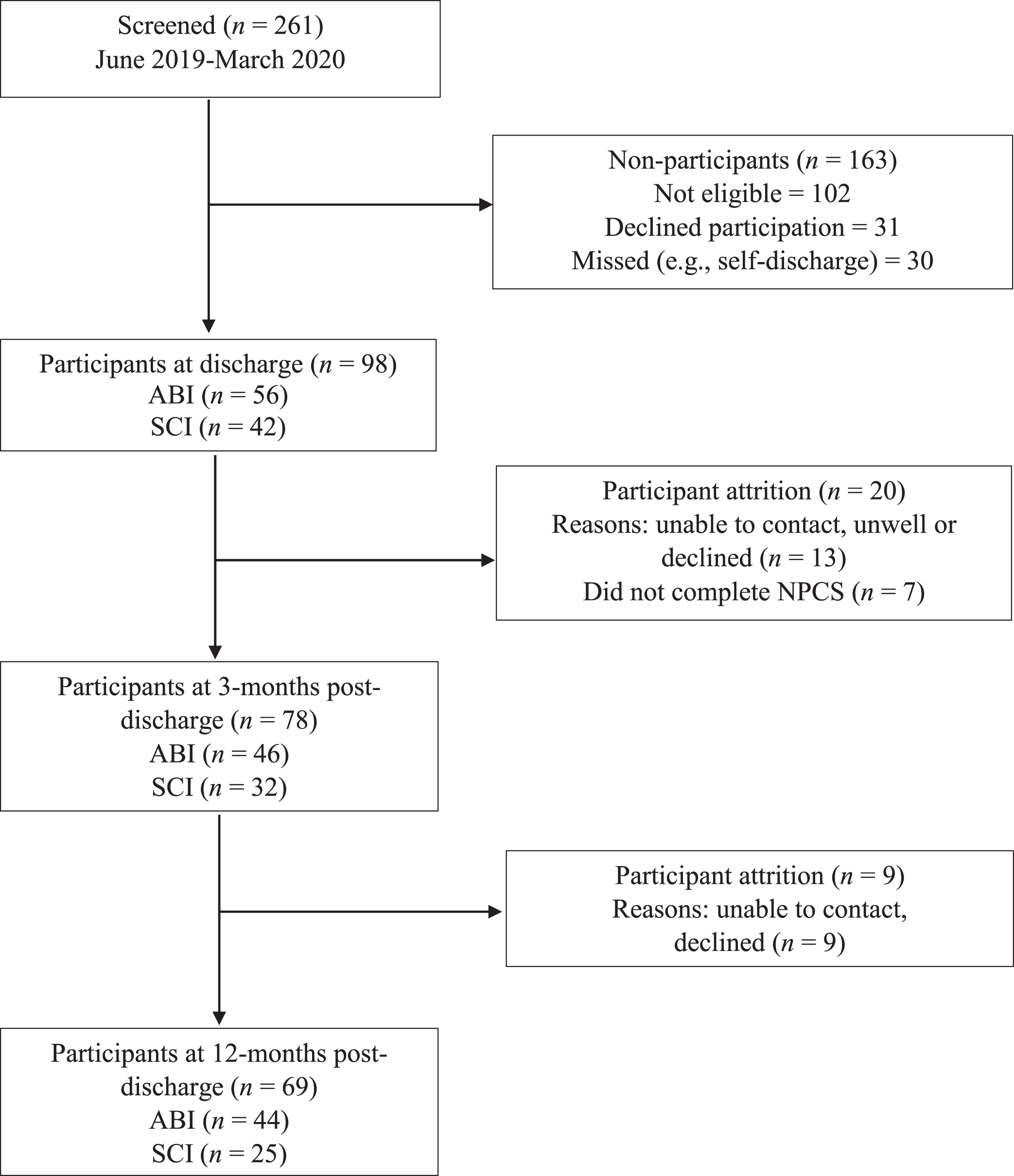
Participant recruitment flow chart.
In total, 69 participants (44 with ABI; 25 with SCI) were included in the analyses. The demographic and injury-related characteristics of the sample are summarised in Table 1. Participants were predominantly male (68%), aged 17–64 years (M = 44.82, SD = 14.23) and in partnered relationships prior to injury (60%). For individuals with ABI, length of stay (LOS) ranged from 12 to 294 days (M = 56.07, SD = 51.2) and functional independence at discharge (FIM total) ranged from 31 to 122 (M = 103.27, SD = 19.9). LOS was longer for participants with SCI, ranging from 45–417 days (M = 187.76, SD = 115.6) and functional independence at discharge was lower (M = 94.32, SD = 24.1; range = 52–121) compared to participants with ABI. In terms of etiology, non-traumatic causes of injury, such as stroke and brain tumour, were the cause for just over half of participants with ABI (52%). Traumatic injury, primarily due to motor vehicle accidents or falls, was the most common cause of SCI (64%). Prior to injury, most participants were engaged in paid employment (77%), and approximately half (52%) were employed full-time. The most common pre-injury occupation type was manual labour (18.8%). As shown in Table 1, most participants (78%) received ABI or SCI rehabilitation through specialised post-hospital pathways, including transitional rehabilitation (70%) and/or community outreach (77%) services. Most individuals with SCI (64%) additionally received the specialist SCI Back2Work EIVR program.
Sample demographic and injury characteristics
Note. Percentages may not equal 100% due to rounding. ABI = acquired brain injury; SCI = spinal cord injury; FIM = functional independence measure. aTransitional rehabilitation refers to Acquired Brain Injury Transitional Rehabilitation Service (ABI) or Transitional Rehabilitation Program (SCI); bCommunity outreach services refers to Acquired Brain Injury Outreach Service (ABI) or Spinal Outreach Team (SCI); cBack2Work EIVR = early intervention vocational rehabilitation (SCI).
At 12-months post-injury, just over half of the sample (54%) indicated that paid employment was a primary desired social role on the MPAI-4, whereas the other participants identified roles such as child rearing, homemaker and volunteer as their primary desired social role. Patterns of RTW and perceived vocational support for participants who were employed at 12-months are summarised in Table 2. At 3 months post-discharge, six participants (9%) reported returning to paid employment, including four employed full-time, and two employed part-time. All participants employed at 3-months post-discharge were still employed at 12-months post-discharge. All but one reported returning to the same duties, although their working hours varied (less hours = 3, same hours = 2, more hours = 1).
Patterns of return-to-work and vocational support for individuals employed at 12-months (n = 15)
Patterns of return-to-work and vocational support for individuals employed at 12-months (n = 15)
Note. ABI = acquired brain injury; SCI = spinal cord injury; FT = full-time, PT = part-time, Y = yes, N = no, M = male, F = female. TR = transitional rehabilitation program (ABI or SCI specific); COS = community outreach service (ABI or SCI specific); SCI-EIVR = spinal cord injury Back2Work early intervention vocational rehabilitation.
At 12 months post-discharge, 15 participants (22%) reported working in paid employment with the majority returning to the same employer (87%) and same duties (60%). Just over half (n = 8; 53%) were employed full-time. The proportion of participants employed was similar across the ABI (25%) and SCI groups (16%) ( η2 = 0.76, p = 0.55). Of these 15 participants, the majority (80%) had received specialist ABI or SCI rehabilitation, which entailed both transitional and community outreach rehabilitation services (see Table 2). All four of the individuals with SCI in the employed group received the SCI Back2Work EIVR program. On the NCPS, seven (47%) had identified a need for vocational support at either 3-months or 12-months post-discharge, which was met. Six participants (40%) did not perceive a need for, nor receive, vocational support in the context of RTW at 12-months post-discharge. A further individual who did not perceive the need for vocational support had received vocational support. Only one participant employed at 12-months post-discharge perceived a need for vocational support (i.e., work assessment/advice) that was unmet. This young female participant (aged 17 years, 11 months) with ABI had been a full-time university student at the time of injury. At 12-months post-discharge she was working part-time with a new employer and new duties.
The 15 participants employed at 12 months had significantly shorter LOS (M = 50.64, SD = 42.74) compared to the 54 participants not employed at 12 months (M = 117.98, SD = 108.73), t(55.150) = 3.602, p < 0.001, Cohen’s d = 0.68, reflecting a medium effect size. They also had significantly greater functional independence at discharge (FIM total M = 112.46, SD = 9.13) compared to those not employed at 12 months (M = 96.79, SD = 22.98), t(50.293) = –3.873, p < 0.001, with a medium to large effect size (Cohen’s d = 0.74). There were no significant differences in age, gender, injury type or access to specialist ABI or SCI rehabilitation (p > 0.05) between the employed and not employed groups (See Table 3).
12-month employment status † examined across gender, injury type, age, length of stay (LOS), and functional status at discharge (FIM) (N = 69)
Note. Percentages may not equal to 100% due to rounding. ABI = acquired brain injury; SCI = spinal cord injury; LOS = length of stay; FIM = functional independence measure. †1 = No (i.e., not employed at 12 months), 2 = Yes (i.e., employed at 12 months). *p < 0.05, **p < 0.01, ***p < 0.001.
Preliminary correlations identified that higher functional independence at discharge (FIM total) was significantly associated with greater home and community participation (r = –0.63, p < 0.001), but was not associated with HRQOL (r = 0.17, p = 0.17) or depression, anxiety, or stress at 12 months (r = –0.04–15, p > 0.05). Greater LOS was significantly associated with lower home and community participation (r = 0.46, p < 0.001), lower HRQOL (r = –0.26, p = 0.034) and higher anxiety (r = 0.40, p < 0.001), but not depression or stress (r = 0.21–23, p > 0.05). Injury type was significantly associated with psychosocial functioning, with individuals with SCI reporting significantly lower home and community participation (r = 0.34, p = 0.005) and HRQOL (r = –0.49, p < 0.001) and greater depression (r = 0.35, p = 0.003), anxiety (r = 0.32, p = 0.008), and stress (r = 0.26, p = 0.028) than individuals with ABI. Female gender was significantly associated with higher anxiety symptoms (r = 0.32, p = 0.007). No other demographic or injury-related variables were significantly associated with psychosocial functioning (p > 0.05).
Descriptive data on psychosocial functioning for the employed and not employed groups are presented in Table 4. Analyses of covariance (ANCOVA) controlling for LOS, functional independence at discharge, and injury type identified that the employed group reported significantly better home and community participation than the not employed group (F = 9.71, p = 0.003, ηp2 = 0.14). Further, after controlling for LOS and injury type, the employed group reported significantly higher HRQOL than the not employed group (F = 4.70, p = 0.034, ηp2 = 0.07). Controlling for injury type, individuals in the employed group also reported significantly lower levels of depression (F = 10.22, p = 0.002, ηp2 = 0.13), and stress (F = 5.25, p = 0.025, ηp2 = 0.07), than those in the not employed group. These differences represented medium to large effect sizes. There was no significant difference in level of anxiety between individuals employed and not employed at 12-months post-discharge (F = 2.18, p = 0.145, ηp2 = 0.03).
Comparison of home and community participation, health status, and psychological distress of the employed and not employed groups at 12-months post-discharge (n = 69)
Comparison of home and community participation, health status, and psychological distress of the employed and not employed groups at 12-months post-discharge (n = 69)
Note. LOS = length of stay; FIM = functional independence measure; HRQOL = health-related quality of life. *p < 0.05, **p < 0.01, ***p < 0.001.
A comparison of perceived vocational support needs and support received on the NPCS identified that the proportion of individuals with needs met did not significantly differ between the employed (87% with needs met) and not employed (82% with needs met, η2 (1,69) = 0.22, p = 0.639) groups. As shown in Table 5, three subgroups were identified for the not employed subgroup, based on the pattern of perceived and received vocational support: 1) those who did not seek or receive vocational support (50%); 2) those who sought vocational support with unmet needs (18%); and 3) those who sought and received vocational support (32%).
Subgroups of individuals who did not return to employment at 12-months post-discharge (n = 54)
Subgroups of individuals who did not return to employment at 12-months post-discharge (n = 54)
*Missing 3-month data (NPCS needs subscale). ABI = acquired brain injury; SCI = spinal cord injury; TR = transitional rehabilitation program (ABI or SCI specific); COS = community outreach service (ABI or SCI specific); SCI-EIVR = Back2Work spinal cord injury early intervention vocational rehabilitation. †Includes FT, PT, casual, and self-employment.
This subgroup reflects individuals who did not perceive the need for vocational support and were not receiving vocational support at either 3- or 12-months post-discharge. Individuals in this subgroup were aged 17–61 years (M = 43.87, SD = 15.23). Although most (59%) were employed at the time of their injury (70% ABI), 30% were not previously working due to health reasons and 11% were actively seeking employment. The majority (89%) identified their injury as the primary reason for not working and identified goals other than employment. For example, one participant in this subgroup noted: “I’d really like some more physio[therapy] or OT [occupational therapy]. I haven’t even considered return-to-work yet” (Male, 17, SCI). A small proportion (11%) identified unemployment at the time of injury as the primary reason for not working at 12-months post-discharge. Most individuals in this subgroup had received specialist ABI or SCI rehabilitation (78%). One individual (4%) had received the SCI Back2Work EIVR program. None of the participants in Subgroup 1 identified paid employment as their primary desired social role.
Subgroup 2: Perceived vocational support needs that were unmet (n = 10)
This subgroup reflects individuals who perceived the need for but did not receive vocational support at either 3- or 12-months post-discharge. Individuals is this subgroup were aged 23-60 years (M = 43.89, SD = 14.20). All ten participants were employed at the time of their injury (80% ABI), and all attributed not working primarily to their injury. For example, one participant with unmet vocational support needs noted at 3-months post-discharge: “[I] would like to decrease rehab[ilitation] and would like support to return to volunteering or work” (Male, 25, ABI). Most had received specialist ABI or SCI rehabilitation (70%), and two (20%) received the SCI Back2Work EIVR program. Half of Subgroup 2 participants (n = 5) identified paid employment as their primary desired social role.
Subgroup 3: Perceived need for and received vocational support (n = 17)
This subgroup reflects individuals who perceived the need for, and subsequently received, vocational support at either 3- or 12-months post-discharge. Individuals in this subgroup were aged 23–64 years (M = 46.81, SD = 11.50) and the majority (88%) were employed at the time of injury. All participants in this subgroup identified their injury and related symptoms or complications as the primary reason for not working. For example, one participant noted: “Pain is still a very big issue for me. I’ve been to a pain specialist and I’m on medications, none of it helps really” (Male, 58, SCI). Another participant desired greater access to therapy to facilitate greater functional gains: “More OT [occupational therapy] would be good because I am getting gains with one session a week; I can only imagine what I could do with more” (Male, 37, SCI). Most individuals in Subgroup 3 had received specialist ABI or SCI rehabilitation (82%), and six received the SCI Back2Work EIVR program. All participants in this subgroup identified paid employment as their primary desired social role.
Injury-related characteristics and psychosocial functioning for individuals not employed at 12-months post-discharge
Supplementary analyses involving chi-square tests and ANOVA were conducted for the participant subgroups not employed at 12-months post-discharge to compare demographic, clinical and psychosocial variables (Table 6). Due to the small subgroup sizes, a Kruskal-Wallis One-Way analysis of variance (ANOVA) was used. The results indicated there were no significant differences between subgroups for age, LOS or FIM total or FIM motor at discharge or access to specialist ABI or SCI rehabilitation (p > 0.05). However, there was a higher proportion of individuals with ABI in Subgroup 2 (80%) relative to Subgroup 3 (35%, p < 0.05) and a higher proportion of individuals with SCI in Subgroup 3 (65%) relative to Subgroup 2 (20%) (p < 0.05). There was a significant difference in cognitive function (FIM cognition subscale) at discharge between the three subgroups (H = 6.53, p = 0.038). Post-hoc tests with a Bonferroni correction identified that cognitive function at discharge was significantly higher for Subgroup 3 (Perceived a need for and received vocational support) compared to Subgroup 1 (Did not perceive the need for or receive vocational support) (H = –12.01, SE = 4.73, p < 0.017). There were no other significant differences in cognitive status between the subgroups.
Kruskal-Wallis one-way ANOVAs comparing subgroups of participants not employed on demographic and injury-related characteristics, and psychosocial outcomes at 12-months post-discharge (n = 54)
Kruskal-Wallis one-way ANOVAs comparing subgroups of participants not employed on demographic and injury-related characteristics, and psychosocial outcomes at 12-months post-discharge (n = 54)
aMean rank, as reported for Kruskal-Wallis test. ABI = acquired brain injury; SCI = spinal cord injury; LOS = length of stay; FIM = functional independence measure; HRQOL = health-related quality of life. *p < 0.05, **p < 0.01, ***p < 0.001.
Results of a Kruskal-Wallis one-way ANOVA revealed no significant differences in home and community participation (H = 2.50, p = 0.286), HRQOL (H = 1.80, p = 0.406) or anxiety (H = 2.90, p = 0.234) between the subgroups at 12-months post-discharge. However, there was a significant difference in levels of depression (H = 6.15, p = 0.046) and stress (H = 6.22, p = 0.045). Pairwise comparisons with a Bonferroni correction identified that individuals in Subgroup 3 reported significantly higher levels of depression compared to those in Subgroup 2 (H = –14.97, SE = 6.22, p = 0.016). Further, individuals in Subgroup 3 reported significantly higher levels of stress compared to those in Subgroup 1 (H = –12.05, SE = 4.85, p = 0.013). There were no significant differences in levels of depression between participants in Subgroup 2 and Subgroup 1 (p > 0.017). Therefore, individuals who perceived the need for and received vocational support reported higher levels of distress at 12-months post-discharge compared to those with unmet vocational support needs, and those that did not perceive the need for or receive vocational support.
This study investigated RTW following ABI or SCI at 3-months and 12-months post-discharge, and associations between employment outcome and psychological distress (depression, anxiety, and stress), HRQOL, and home and community participation. Paid employment was the primary desired social role for 54% of participants at 12-month post-discharge, thus highlighting that nearly half of participants had other primary desired social roles (e.g., child rearing, homemaker, volunteer). As hypothesised, individuals who had returned to employment by 12-months post-discharge reported lower levels of depression, anxiety, and stress, better HRQOL, and greater home and community participation compared to individuals who were not employed at 12-months post-discharge. Contrary to the second hypothesis, employment outcomes did not differ according to individuals’ perceived need for and receipt of vocational support. For those not employed at 12-months, three subgroups were identified: 1) Did not perceive the need for or receive vocational support (n = 27); 2) Perceived vocational support needs that were unmet (n = 10); and 3) Perceived and received vocational support (n = 17). Participants in the latter subgroup reported greater symptoms of depression and stress at 12-months than those in the other subgroups.
Consistent with previous research [53–56] and the first hypothesis, RTW after acquired neurological injury was associated with better psychosocial functioning at 12-months post-discharge. Compared to those not employed at 12-months, individuals employed at 12-months post-discharge had shorter LOS and greater functional independence at discharge and reported lower psychological distress, better HRQOL, and greater home and community participation. The present findings reinforce previous research highlighting functional independence at discharge as a predictor of RTW outcomes following ABI [8, 14] and SCI [12, 47]. Six individuals in the employed group (40%) did not perceive a need for vocational support to facilitate RTW, which may be due to various factors including, but not limited to, greater functional independence, positive expectations of RTW and maintenance of the occupational bond with their employer [53]. Other individuals in the employed group had their vocational support needs met through work assessments, advice, or ongoing support, thus highlighting the value of early vocational rehabilitation [53].
A key finding of the present study is that employment outcomes at 12-months did not differ according to individuals’ perceived need for and receipt of vocational support. Only a small proportion (18%) of individuals in the not employed group reported having unmet vocational support needs which included a combination of work education, assessment or advice; ongoing work education and support; and formal vocational programs. Most individuals in this subgroup had ABI (80%), were working in paid employment at the time of injury and had shorter LOS (M = 77 days) than the other two subgroups (M > 120 days). Some possible explanations are that RTW was not a goal for these individuals at that early phase of community reintegration or their vocational goals were not addressed by rehabilitation services. Notably, for half of these participants (n = 5), paid employment was not their primary desired social role and access to specialist post-discharge rehabilitation services for ABI and SCI (70%) for this subgroup did not significantly differ from other subgroups (78–82%). Hence, their rehabilitation programs may have focused on goals other than paid employment. It is also possible that individuals in this subgroup received some form of vocational support but did not perceive or recall this support as constituting a RTW intervention, for example, due to impaired self-awareness or memory deficits.
Overall, the mismatch between individuals’ perceived need for and receipt of vocational support suggests the need for rehabilitation professionals to assess and revisit individuals’ vocational goals, ensuring rehabilitation is responsive to these goals, and to clarify or make more explicit the different forms of vocational rehabilitation supports being provided. A study on consumer perspectives of RTW interventions after ABI [41] identified the importance of early access to vocational rehabilitation, and highlighted individuals’ preferences for programs to provide intensive and individualised support, employer education and liaison, workplace support and peer mentors.
The second largest subgroup (32%) of participants not employed at 12-months (Subgroup 3) reported having their vocational support need met. Hence, the desire for and provision of vocational support may not ensure RTW in the first 12-months post-discharge. These participants identified their injury as the primary reason for not working and reported higher levels of depression and stress at 12 months than other subgroups. Importantly, mental health issues may precede or be a consequence of employment difficulties [11]. It is possible that individuals in Subgroup 3 experienced higher levels of distress prior to receiving vocational support for RTW, which in turn may have limited intervention effectiveness. In a qualitative investigation into factors impacting RTW after stroke, Hartke [72] highlighted a myriad of psychological issues that may impede work reintegration, including difficulties accepting new limitations, reduced self-confidence, performance anxiety, and motivational and coping difficulties. Notably, a supplementary analysis of DASS-21 data at discharge identified no significant differences in earlier levels of depression, anxiety, and stress between the not employed subgroups. At 12-months post-discharge, this subgroup had higher depression and stress levels but did not differ from the other subgroups on home and community participation or HRQOL. Although various personal and social factors may have influenced their distress levels at this time point, it is possible that inability to RTW as a primary desired social role was a contributor to their levels of depression and stress. Additionally, unsuccessful attempts to resume employment may have facilitated insight into one’s limitations which may have contributed to greater psychological distress. Furthermore, in some cases, the experience of unemployment despite vocational support may have been associated with job type, whereby individuals may not have been able to return to previous work positions as a result of injury-related consequences (e.g., a forklift driver unable to operate heavy machinery due to seizures resulting from an ABI).
Payne [73] similarly found that individuals with TBI living in the community who were not employed but wanted to be productive reported elevated psychological distress. Given that such individuals had received vocational support, they may have had greater self-expectations and/or perceived pressure from others to RTW [8, 72]. Further research is needed to examine reasons for lack of RTW success in those receiving vocational support, which may relate to diverse personal and socio-environmental factors such as interpersonal skills, self-awareness, motivation, strategy use, the type, availability and quality of vocational support, job type, workplace accommodations and employer support [11, 75]. Importantly, such research should seek the perspectives of multiple stakeholders involved in the RTW process.
The largest subgroup (50%) not employed at 12-months did not perceive the need for or receive vocational support. None of these individuals identified paid employment as their primary desired social role. Such individuals typically had low functional independence at discharge and nearly half were not employed prior to the injury, often due to pre-existing health issues. Therefore, their pre-injury circumstances combined with recognition of their functional limitations after ABI or SCI may have altered individuals’ goals and expectations regarding RTW. Although a significant proportion of individuals with ABI and SCI may return-to-work in the first 12-months post-discharge (∼40–50%) [1–3, 6], RTW can take many years for some individuals who may prioritise other goals (e.g., self-care and independence, parenting). Others may ultimately make the decision that RTW is not feasible or compatible with their interests and capabilities [3, 57], thus pursuing other valued occupations. In a severe brain injury cohort, Wang [6] found that delayed RTW was associated with receiving health insurance, lower educational level and more severe motor disability. They advocated for individualised pathways of vocational rehabilitation and support to align with individuals’ readiness and functional capabilities. Access to services that provide vocational rehabilitation and support to clients with ABI and SCI in the longer-term is a recommendation for future service development.
Clinical implications
A key clinical implication of the present findings relates to the need for clinicians to explore individuals’ perceived need for and preferences for vocational support and provide flexible and individualised support. To avoid a mismatch between individuals’ expectations and support received it may be beneficial to clarify, revisit and make explicit the different types or forms of vocational support. This includes supporting individuals to develop a broader concept of meaningful vocational activity that goes beyond paid employment (e.g., volunteering, study) [39–41]. The present findings also highlight the need to monitor the psychological well-being of those who are not able to RTW despite receiving vocational support, as they appear to be a subgroup at risk of depression and heightened stress. Additionally, it may be beneficial for rehabilitation services to revisit their clients’ readiness and need for vocational support and training over longer periods of time post-injury, and for funding bodies to recognise that RTW represents a longer-term goal for some individuals. In their review of employment outcomes after ABI, Van Velzen [15] found that changes in work tasks and loss of employment after job placement were common and recommended long-term follow-up and extended vocational support to enhance employment stability.
Although the focus of the present study was on perceived vocational support and RTW, the factors promoting job retention or sustained employment are critical considerations for vocational planning. A review on factors influencing job retention after ABI by Alves [35] highlighted a lack of research into workplace characteristics, with most existing studies focusing on individuals’ pre-injury and injury characteristics. In the SCI literature, a review by Karcz [13] identified that an interplay of person-related (e.g., age, education, impairment level, attitude) and socio-environmental factors influence work retention. In relation to the latter, job matching through a skills and work environment assessment and inclusive work environments (e.g., tailored assistive technology, work accommodations, flexibility, and supportive work colleagues) were most conducive to sustained employment outcomes.
Limitations
Several limitations associated with this retrospective cohort study are important to acknowledge. First, the study had a relatively high rate of attrition (30%) between discharge and 12-months follow-up. Although there were no significant differences in the demographic or injury characteristics of individuals retained and those lost to follow-up, both the attrition and small samples (ABI n = 44, SCI n = 25) affect the ability to generalise the findings to the broader ABI and SCI populations. Data were collected during the COVID-19 pandemic during a period of restrictions and lockdowns which is likely to have had multiple impacts on vocational rehabilitation and support services as well as work opportunities and environments. Individuals’ motivation to RTW, ability to action RTW plans and their perceived need for and receipt of vocational support may have also been affected, which cannot be accounted for in the current study. Second, due to the lengthy assessment battery individuals received as part of the broader study, only selective information was sought regarding participants’ RTW experiences, and their perceived vocational support needs and support received. For example, individuals were not asked about contact with former employers, job applications, interviews, or work trials, which may have illuminated some reasons why individuals in Subgroup 3 were unable to RTW despite receiving vocational support. Third, due to reliance on self-reports, it was not possible to verify the type or intensity of work-related education, assessment, advice, and other forms of vocational support individuals received. In future research it would be beneficial to obtain collateral information from clinicians and family members concerning individuals’ vocational goals and the related interventions and services accessed.
Conclusion
In the combined ABI and SCI sample, approximately one in five individuals had returned to work at 12-months post-discharge. Paid employment was the primary desired social role for just over half of the sample. RTW was associated with better psychosocial functioning. For those not employed, three subgroups were distinguished based on their perceived need for and receipt of vocational support. Only a small proportion (18%) reported vocational support needs that were not met. Levels of psychological distress (namely, depression and stress) were highest for those who perceived and received vocational support. Overall, the findings highlight the need for clinicians to explore and revisit individuals’ perceived need for and preferences for vocational support, provide flexible and individualised support over the longer term, and monitor the psychological well-being of those not successful in returning to work. Further research investigating reasons for individuals’ lack of success with RTW for those receiving vocational support is recommended.
Ethical approval
Ethics approval was obtained from the Metro South Hospital and Health Service (MSHHS) Human Research Ethics Committee (HREC) (HREC/2019/QMS/50271) and Griffith University Human Research Ethics Committees (2019/456).
Informed consent
Informed consent was obtained from all participants or their substitute decision-makers.
Conflict of interest
Not applicable.
Footnotes
Acknowledgments
The authors would like to thank all participants for their involvement in the study. They also acknowledge the early input of Professor Michele Foster on this project.
Funding
This project was funded by the Metro South Health Research Support Scheme and the Motor Accident Insurance Commission.