
Abstract
BACKGROUND:
Active break programs at the workplace are a promising initiative for increasing workers' physical activity (PA) levels, health, work-ability (WA), and social relationship.
OBJECTIVE:
To determine the impact of an Active Breaks workplace program based on Bandura’s Social Cognitive Theory (SCT) aligned with Behavior Change Techniques (BCT) on PA levels, cardiorespiratory fitness (CRF), WA, and social relationships among university workers.
METHODS:
#UCLMuévete is a quasi-experimental, 12-week intervention designed according to the TREND and TIDieR-PHP checklists. Sixty-nine university workers were recruited and placed into 17 teams of 3 to 5 people. Participants were instructed to take a 20-min active break every working day (walking, cycling, and functional training). The following variables were measured before and after the 12-week intervention: (1) Amount of PA with accelerometers, (2) CRF through the 6 Min-Walking Test (m), (3) Body composition (fat mass (gr), muscle mass (gr), and bone mineral content (g/cm3) through densitometry), (4) Stress with the BodyGuard2 device, (5) WA through Work Ability Index (WAI), and (6) Social relationships through an ad-hoc questionnaire. Part-time workers, pregnant women, and workers with physical disability were excluded.
RESULTS:
Significant improvements were observed in the amount of daily moderate-to-vigorous PA (Difference (Dif)., women +8.05 and men +12.31 minutes; p < 0.05; ES = 0.224; 0.379), CRF (Dif., women +52.98 and men +25.53 meters; p < 0.05; ES = 0.578; 0.209), and (Dif., women +2.16 and men +2.39; p < 0.05; ES = 0.150; 0.177). No significant changes were observed in body composition and stress.
CONCLUSION:
20 min/day of aerobic and strength active breaks, based on SCT aligned to BCTs, improves university workers’ amount of PA, CRF, WAI, and social relationships.
Introduction
Evidence suggests that workplace wellness programs based on physical activity (WWPPA) are effective in reducing non-communicable diseases and WA of workers that occur as a result of an increase of physical inactivity among workers [1–3]. Furthermore, WWPPA are also associated with improvements in mental health if the delivered physical activity (PA) includes socially connecting with others [4, 5]. For these reasons, international organizations such as the WHO [6] encourage the implementation of WWPPA in occupational environments.
Despite this strong evidence in favor of WWPPA, widespread application in workplaces is yet to be achieved [4]. This is the case on university campuses, where few studies have been reported [7], even though many university workers accumulate long periods of sitting time, are physically inactive, and/or report high body mass index [8]. Meanwhile, factors such as strict deadlines, overwork or communication problems with colleagues and superiors may lead to considerable mental stress that enhance psychological risks [9]. Therefore, further attempts to introduce WWPPA among university workers are needed [10].
One reason for the lack of WWPPA programs on university campuses is that designing these programs is complex (e.g., timing, target population, intervention settings, etc.), especially if it requires restructuring the physical environment or if university workers are spread across several physical locations [11]. The current wave of literature suggests structural changes in the work environment (e.g., standing desks, active workstations) [12] and the use of active breaks (e.g., 10-20 min break within the workday to do some resistance, strength, stretching, etc., structured or semi-structured PA) or full structured-PA sessions of 45–60 min (e.g., biking or yoga) are beneficial to promote healthier habits in workers [3].
Some attempts using the full structured-PA session approach has been applied to university workers with promising results on increasing their PA level and health through aerobic (cardiorespiratory endurance) or anaerobic (muscle strengthening resistance) exercises [13]. However, the PA duration (≥45 min), the required materials, resources, and the used facilities are barriers to replicate the approach in other universities and to achieve high adherence-level to the implemented programs [11]. Active breaks might overcome these barriers as the PA timing session is much shorter (≈10–20 min), can be designed to use minimal or null fitness equipment (e.g., back exercises), and worker can have the flexibility of doing the brake anytime along the workday [14].
As a health promotion intervention, WWPPAs can be designed using behavior change theories such as the Bandura’s Social Cognitive Theory (SCT) [15] aligned to Behavior Change Techniques (BCTs) which are the active components that aim to bring about change [16]. Several studies have examined the effectiveness of SCT in increasing adherence [17] and the quality of social environments [18]. Whereas the use of technological advances (i.e., mHealth) combined with the SCT constructs can drive greater impact in workers’ habits [19]. However, to date no intervention targeting university workers has used mHealth tools or the SCT aligned with BCTs (e.g., goal setting, action planning, feedback on outcomes of behavior, self-monitoring and social comparison) to increase WWPPAs effectiveness by delivering BCTs [20]. Smart offices are another option to promote PA among workers by visualizing activity status, reminders, summaries, and exercise suggestions [21], but this technology is still to be implemented in Spanish public universities.
Thereby, the aim of this study was to analyse the impact of a WWPPA, a program which includes 20 minutes of active breaks, on the amount of PA, cardiorespiratory fitness level (CRF), work-ability index (WAI) and social relationships on university workers.
Materials and methods
Design
This is a quasi-experimental study conducted among a single group of university workers with pre-post measures, between September and December 2021. The protocol received approval from the Clinical Research Ethics Committee of the University Health Service, Spain based on the latest version of the Declaration of Helsinki (Ref.: 742/01072021). Written informed consent was obtained from all participants prior to data collection.
Participants
69 workers, either faculty or university staff on the same campus, were recruited for the study. From this total, 61 workers finished the program, but due to the COVID-19 pandemic, two participants were unable to complete post-test measures. The final sample was composed of 59 workers of UCLM (n = 39 female; n = 20 male; 24–55 years). The primary inclusion criteria required the individuals to participate in teams as social interaction was one of the BCTs applied. Accordingly, they signed up as teams of 3 to 5 people. A total of 17 teams participated in the program. This decision was made based on previous studies have reported that teams increase adherence to WWPPA by increasing the intrinsic motivation and attitude toward the intervention [22]. The members of these teams did not necessarily have to belong to the same job position. Volunteers working less than 6 hours/day, part time workers, pregnant women, and workers with physical impediment that prevents or discourages the practice of PA were excluded from the study.
Study timeline
During the recruitment and enrollment phase, a media campaign of the project, and material was distributed by e-mail, newspaper, social media, and posters throughout the university campus. Interested workers completed a questionnaire and signed up in teams. Once all the teams were enrolled, the research team met with the participants in person to explain the study, answer questions, and review and sign the informed consent. UCLMuevete intervention spanned 12 weeks. The principal investigator completed the baseline and 12-week post-intervention data collection (see Fig. 1).
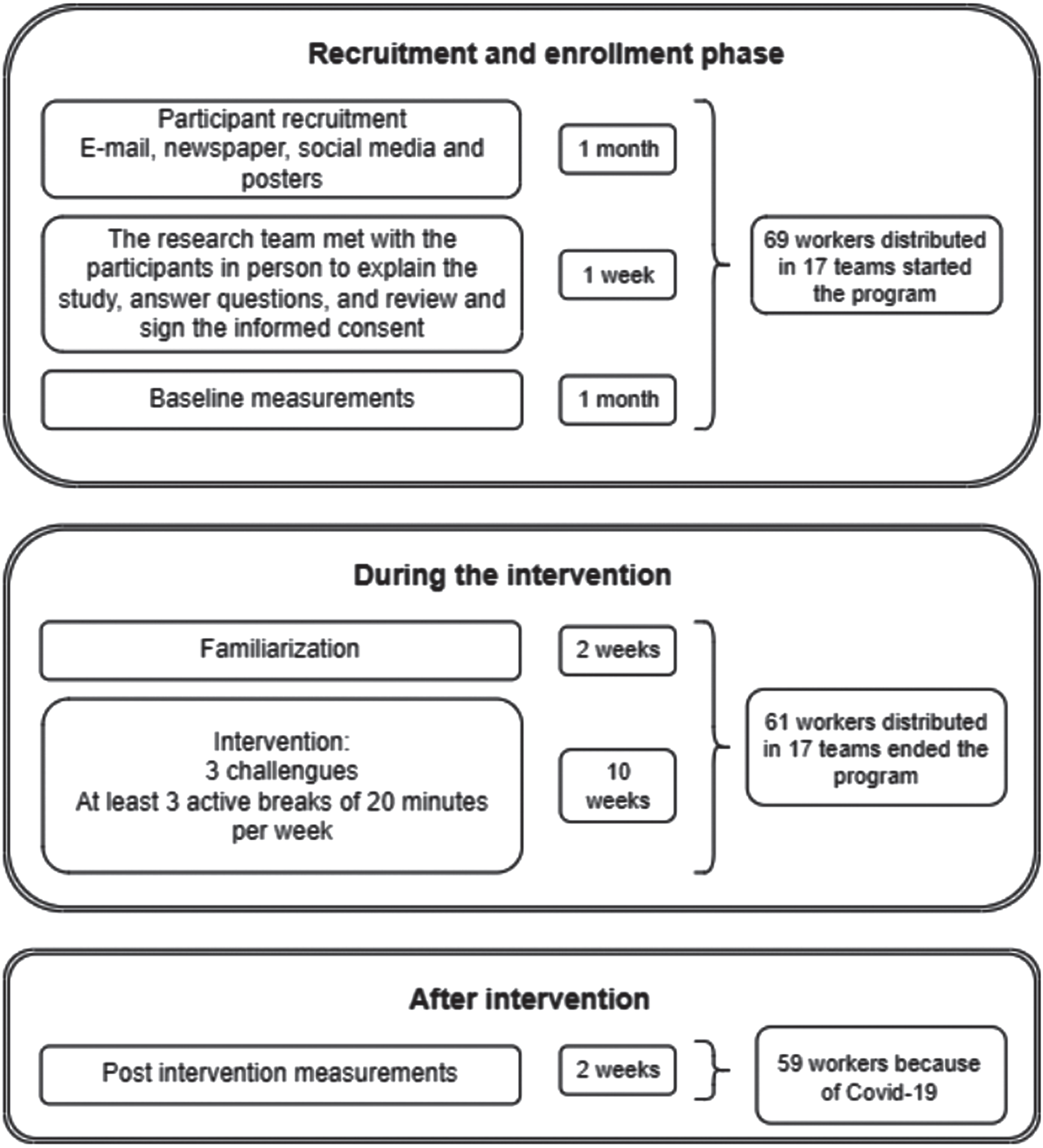
Flow diagram phases of UCLMuevete.
The PA intervention was designed to assist the workers in achieving the current PA guidelines for adults recommended by the World Health Organization (WHO) [6], consisting of 20-min sessions of both moderate to vigorous aerobic (cardiorespiratory endurance) and anaerobic (muscle strengthening resistance) PA, 5-days/week for a period of 10-weeks. Participants were instructed to complete one session per day during the working day and encouraged to do a minimum of 3 sessions per week. For each session, participants could choose any space in Campus University for partaking the active break and could use the campus sports facilities (gym, bicycle and walking path). A detailed breakdown of UCLMuevete project is provided in Supplementary file 1 according to the TREND and TIDieR-PHP checklists [23].
The intervention was tailored according to Bandura’s Social Cognitive Theory (SCT) because it is one of the most widely used theories for tailoring wellness programs. This theory suggests that individuals’ behavior is regulated through reinforcement (internal and external social reinforcement, social influences and past experiences) and control (self-efficacy) [15]. Moreover, the main construct of this theory, self-efficacy, defined as the belief in one’s capabilities to execute the desired behavior, has been associated with increasing the effectiveness of PA interventions [24]. Following the previous studies’ recommendations, the intervention was designed using the behavior change techniques taxonomy 1 (BCTs) [25]. (see Supplementary Table 1).
Mobile app –Apptivados- wereables –mHealth
As part of the project, a Mobile App “Apptivados” was developed with four sections: a) news, b) personal trainer, c) nutrition, and d) challenges. In section a) news, participants received a daily notification about the exercise they should do and a motivational message. In addition, participants could interact through this section, replying to each other in comments and likes. In section b) personal trainer, participants had access to an agenda with the five active breaks of the week, and the participants could choose the active break to perform. This session included exercise descriptions, recommendations, times, repetitions, muscles involved, and instructional videos. In section c) nutrition, participants received weekly posts on nutritional aspects such as food properties or healthy food recommendations for the workplace. In section d) challenges, the rankings and points of the different teams were published. In addition, all participants were supervised by an activity bracelet model Xiaomi Mi Band 4, which has been validated in other studies with similar purposes, to record their daily activity such as total time, number of steps, and heart rate [26].
Challenges
The intervention was delivered to each team in form of three challenges. The challenge achievement resulted into points and rewards (fruit, restaurant gift cards, and t-shirts). Challenge 1-“Camino de Santiago by bicycle”: aerobic exercise, that required participants to pedal for at least 20 minutes, simulating a stage of the Camino de Santiago Road. Challenge 2-“Get to know the Fábrica de Armas Campus”: aerobic exercise, consisted of a 20-minute walk around the university campus. Challenge 3-“Be strong”: strength exercises, a set of 4 strength exercises involving major muscle groups.
These three challenges were alternated each week, so the participant completed three aerobic sessions and two strength sessions (e.g., 3 sessions of walking and 2 of strength). The session volume increased weekly, and participants were asked to complete the sessions at the highest intensity possible to ensure they performed vigorous PA. Rankings resulting from challenges were based on three criteria: (1) days of participation per week; (2) the total invested time of the active pause (which could oscillate between 15 and 20 min per day); and (3) the average heart rate or steps recorded. Daily activity, heart rate and steps were registered using an activity bracelet Xiaomi Mi Band 4 [26].
Social media
To promote participant engagement, interaction, and motivation, a marketing campaign was developed through the @uclmuevete accounts on Instagram, Twitter, Youtube, and email. Daily goals photos and videos were published on the social media accounts and in the app.
Data collection
Two data collection periods were established: baseline and after the 12 weeks’ intervention. The first measurement included two questionnaires (the WAI and Ad-hoc questionnaire) a physical health assessment (densitometry, body composition, and CRF), the use of a Bodyguard 2 device for 48 hours (for Heart Rate Variability (HRV) registration, stress and relax) and an accelerometer for five days (for PA levels). The data were collected in the laboratory of the research group.
Questionnaires
Participants were asked to complete two questionnaires: The Work Ability Index (WAI) and an ad-hoc questionnaire. The questionnaires were administered on paper.
Work-Ability Index (WAI)
The WAI is a questionnaire used to assess the WA of workers [27]. The index is determined from answers to a series of questions, which consider job demands, workers’ health status and resources. The questionnaire contains 10 questions and 7 dimensions ranging from 7 to 49, with higher values indicating better WA. The results are classified into four groups: –weak (7-27) –average (28-36) –good (37-43) –excellent (44-49) [28].
Ad-hoc questionnaire
The following questions were formulated at the end of the intervention participants were asked the following questions: 1) Do you consider that the relationship with your teammates has improved after participating in UCLMuevete? With categorical answer: Yes; no; 2) After the program, do you consider that social relations with the rest of the teams have improved? Yes; no; 3) Do you consider that taking active breaks has been a motivating factor in your daily working life? With dichotomous answers yes or no; and 4) Do you consider that you have suffered stress as a result of the active breaks? With dichotomous answers yes or no.
Physical health assessment
a. Densitometry and body composition
Bone mass (BMC; in g) and bone mineral density (BMD; in g/cm2), fat mass (g) and muscle mass (g) were calculated using DXA (Hologic Series Discovery QDR, Physician’s Viewer Software, APEX System Software Version 3.1.2., Bedford, MA, USA), following the DXA best practice guidelines described previously [29]. Before any measurements, the DXA was calibrated each day with phantoms, as per the manufacturer’s guidelines. The participants were in a supine position with their hands level with their hips and their feet slightly apart. All DXA scans, completed with the same device and software, were performed by certified and trained DXA technicians who positioned the participants, performed the scan, and executed the analysis following research facility standard operating procedures. All scans were analyzed using the software auto-analysis feature, followed by manually correcting analysis markers when necessary to avoid measurement errors. Total body and regional analyses were performed in a routine clinical manner. Fat mass was obtained from the sum of the lean soft tissue mass and bone mineral content and was calculated from whole-body scans excluding the head. The fat mass coefficient of variation for repeated measures was < 3.3% [29].
b. Cardiorespiratory fitness capacity
The six-minute walk test (6MWT) is a widely used measure of exercise capacity in many conditions affecting young adults. The 6MWT tests were performed following American Thoracic Society guidelines, and subjects were instructed to walk from end to end 30 m with signs every 3 m marked with a cone, at their own pace, while attempting to cover as much ground as possible in the allotted 6 minutes [30]. Technicians encouraged subjects with the standardized phrases “You’re doing good” or “Keep it up.” Subjects were allowed to stop and rest during the test, but were instructed to resume walking as soon as they felt able to do so. The 6MWT present the values in meters and it classified the participant according to their CRF percentile: very low (<5th), low (5th to 25th), regular (26th to 50th), good (51th to 75th), excellent (76th to 95th) and superior (>95th) [31].
c. BodyGuard 2 device. HRV, stress and recovery
HRV measurement refers to the measured heartbeat-to-heartbeat intervals, and through this parameter the amount and intensity of PA, stress and recovery can be determined. Using the Firstbeat BodyGuard 2 device, the heartbeats recorded during two working days are analyzed to determine the stress and recovery load of the participants (Firstbeat Technologies Ltd., Jyväskylä, Finland, 2014). For this purpose, the subject had to place the device on their chest. This information was downloaded into the Firstbeat SPORTS software (version 4.7.2.1). The validity of the device has been demonstrated in other investigations, being considered accurate for monitoring HRV [32].
d. Accelerometry
The MOX1 is a validated accelerometer-based activity recording device that measures high-resolution raw acceleration data for up to 5 days [33]. Using the IDEEQ software, objective measurements of PA can be classified and quantified. It provides information on: (1) Accelerometer raw data (x, y, z); (2) Posture detection (sedentary (lying/sitting) or standing); (3) PA intensity (counts per minute); and (4) PA classification (low, medium and high intensity). The subject attached the sensor to the upper leg with a biocompatible adhesive [33].
Outcomes
The primary criteria for determining intervention efficacy were the changes in the amount of PA (minutes). Using accelerometer data, the sitting time, standing time, and low, moderate and/or vigorous PA (MPA; VPA; MVPA) have been analyzed. Secondary outcomes include WA, CRF (based on distance), body composition (fat mass, muscle mass, body weight and bone mineral density), stress level and social relationships. These secondary outcomes were chosen to understand the underlying mechanisms/processes by which the overall health improve.
Data analysis
Data were analyzed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). A repeated-measures ANCOVA test was used to compare intergroup mean differences. A p-value less than 0.05 was considered to indicate statistical significance. The analysis was divided by women and men, repeating the same tests by corresponding genders. The assumption of a normal distribution of the dependent variables in the group was checked. The effect size (ES), a measure of the magnitude of change, was calculated using Eta squared (η2). ES was assessed using the following criteria: 0–0.1 = low, 0.1–0.6 = medium, >0.14 = high [34]. Continuous data were presented in terms of mean±SD. The categorical data were presented in terms of frequencies and percentages.
Results
Descriptive data is displayed in Table 1: Statistical scores of body composition, accelerometry, stress, WA and 6 MWT in women before and after the intervention and Table 2. Statistical scores of body composition, accelerometry, stress, WAI and 6 MWT in men before and after the intervention. Sedentary time decreased in the post-measure (p < 0.05; women -27.76±13.29 and men -65.14±27.67 minutes), while improvements after intervention were found for MVPA (p < 0.05; women +16.10±4.99 and men 24.64±7.40 minutes), VPA variables (p < 0.05; women 15.83±3.03 and men 17.04±5.45 minutes), WAI (women +2.16±0.83 and men +2.39±1.18) and 6MWT (p < 0.05; women +52.98±7.34 and men +25.53±11.38 meters). All differences showed moderate to high effect sizes (between 0.103 and 0.578). Finally, a decreased in relax was displayed in men (stress variable) (p < 0.05; -11.32±3.83%).
Statistical scores of body composition, accelerometry, stress, WAI and 6 MWT in women before and after the intervention
Statistical scores of body composition, accelerometry, stress, WAI and 6 MWT in women before and after the intervention
BMD: Bone mineral density; LPA: Low physical activity; MPA: Moderate physical activity; VPA: Vigorous physical activity; MVPA: Moderate-to-vigorous physical activity; RMSSD: Square of the root mean square of successive differences between R-R interval; WAI: Work-ability index; & 6MWT: Six-minute walking test. * p<0.05.
Statistical scores of body composition, accelerometry, stress, WAI and 6 MWT in men before and after the intervention
BMD: Bone mineral density; LPA: Low physical activity; MPA: Moderate physical activity; VPA: Vigorous physical activity; MVPA: Moderate-to-vigorous physical activity; RMSSD: Square of the root mean square of successive differences between R-R interval; WAI: Work-ability index; & 6MWT: Six-minute walking test. * p<0.05.
Before the intervention 69.23% and 80% of women and men performed more than 300 min of MPA per week. After the intervention an increase of 2.56% were observed in MPA in women, while no changes were observed in men. On the other hand, an increase of 30.77% and 15% in women and men performing more than 150 minutes of VPA per week was observed after the intervention. Concerning the classification of 6MWT by percentile, the number of women increase in the excellent (76th to 95th) and superior (>95th) categories (n=+4; n=+2), while the low and regular (26th to 50th) decreased (n=-3; n =-3). Regarding men, an increase was observed in the excellent category (76th to 95th) (n=+3) and a decrease in the low (<5th) (n=-3). Regarding WAI, all categories: weak, average, good, and excellent described improvements after the intervention. In the case of women, a decrease in the average and good categories (n=-3; n = -4) and an increase in the excellent group (n=+7) were observed. In men, the average and good categories decreased (n=-3; n = -2), while the excellent category increased (n=+5).
Finally, according to the results measured by the ad-hoc questionnaire on social relationship, 1) 70.3% of participants considered that the relationship with their teammates (belonging to the same team) improved after the intervention, 2) 74.8% of participants felt that social relations with other colleagues of UCLMuevete also improve after the intervention, 3) 96.4% of participants said that taking active breaks was a motivating factor in their daily work life, and 4) 37.5% considered that suffered stress as a result of active breaks.
This is the first intervention in university workers that promotes physical exercise and impacts on the social relationship through a WWPPA which include active breaks based on Bandura’s Social Cognitive Theory of Self-Regulation aligned to Behavior Change Techniques, using mHealth as a tool to promote adherence to the practice. The results show an improvement in the amount of daily PA, WA, CRF, social relationship, and high adherence in women and men.
One of the main findings of this study is that participating in short-active breaks at the worksite that includes strength and aerobic exercise contributes to increasing the average daily MVPA engagement of workers in both women (16.10±4.99 min) and or men (24.64±7.40 min). This confirms that university campuses present opportunities to target healthy behaviors such as PA [35], as well as active breaks in the workplace are effective to increase daily PA levels of workers. Moreover, the increase of the average daily MVPA engagement due to active breaks substituting sitting behavior is associated with lower all-cause, CVD and cancer mortality risk (3). In addition, the increase of women who surpassed the threshold of 150 min of VPA by 30.77% suggests that interventions based on active breaks in worksites are effective tools to target the gender gap in PA reported in previous studies [36] and the fact women usually report lower engagement in VPA [37].
Sedentary behavior in the workplace is frequently targeted in health-related interventions at the workplace because of its association with non-communicable diseases and premature death [38]. Even if this behavior was not targeted in the UCLMuevete, the outcomes from accelerometers suggest that the 20 min break intervention at the workplace contributed to decrease the average daily sedentary time over 40 minutes (women -43.14 min; men -65.14 min). These findings might mean that participants substituted some sedentary behavior for light-to-MVPA not only at the workplace, but also in their time off work. Future studies should explore this further to confirm these findings and the nature of the changes in sedentary behavior in time off work.
On the other hand, this intervention aimed to increase the CRF of participants as a result of their participation in active breaks as higher cardiorespiratory fitness is associated with lower risk of cardiovascular diseases [31, 39]. Even if the goal standard test for measuring CRF was not used, the outcomes from 6MWT distance to estimate participants’ CRF has been reported to be reliable enough in the general population and permits measuring CRF of workers in an easy and fast way so can be implemented in real interventions at the workplace. The outcomes from the UCLMuevete suggest that WWPPA with 20 min of active breaks based on strength and endurance exercise not only increases the average CRF levels, but also helped several participants to move from the initial CRF stage to higher stages, including the 5 people who initially reported low CRF (n = 5), so, although further research is needed, just 20-min break at the workplace might reduce the risk of cardiovascular diseases.
According to previous studies, 30 min to 40 min of PA intervention at the workplace can improve the WA [40, 41], which might contribute to decrease absenteeism [42]. The UCLMuevete program indicates that 20-min break can also improve the WA, as those participants with low WA at baseline displayed a considerable improvement after the intervention. However, these findings are limited by (a) the high average WA reported in baseline and (b) the fact of this project’s methodology does not permit to set cause-effect because we could not conduct a follow up; so further research is needed in this regard.
The relax variable was significantly affected by the intervention in men. Therefore, contrary to other authors [43], the increase in PA at work may not lead to significant improvements in stress levels measured objectively. According to the ad-hoc questionnaire completed after the intervention, the lack of improvement in the stress level in men may be attributed to the fact that 37% of workers reported suffering stress during the intervention; being the non-stop high mental workload, frequent interruptions during work, and unfinished tasks [44]. Nonetheless, stress is a multicomponent construct that fluctuates over time [45]. Therefore, conducting multiple stress measurements throughout the intervention could enhance our understanding of how stress is affected by environmental fluctuations [45].
Changes in body composition are strongly influenced by dietary habits, PA, and/or sedentary time [46]. Thus, although dietary habits were not controlled, the increase in PA and the decrease in sedentary time led us to expect improvements in participant’s body composition [46], but this hypothesis was not fulfilled in the study. The possible reasons are (a) the short duration of the intervention (12 weeks), (b) the length of active breaks (20 minutes), and (c) the fact post-intervention measurements coincided with the week before Christmas day and many participants reported to increase social events and food intakes [47, 48].
One of the topics of interest to researchers is identifying the factors necessary to increase adherence to PA programs in order to achieve long-term effects [49]. According to Bourne and colleagues [25], behavior change theories might increase effectiveness of interventions at the workplace, although a misguided application of this theory has been reported in previously [37]. To reduce the risk of misuse, and also, facilitate future comparisons [16] the intervention was designed considering only those BCTs that match with Bandura’s SCT [15]. On the other hand, we could not test the effect of the intervention in comparison to a control group. However, the 88.40% of adherence and the improvement in social relationships and motivation of the participants after the intervention are in line with other researchers which suggest SCT-aligned BCTs and integrated in mHealth are effective to promote behavior change in PA, motivation, adherence, and social relationship [25, 51]. Finally, it would have been interesting to measure the effect of the intervention on musculoskeletal disorders, which are considered a common pathology among office workers [52]. Moreover, other studies have demonstrated that taking active breaks of 10-20 minutes could have a positive impact on musculoskeletal disorders [52]. Therefore, we will consider musculoskeletal disorders as a measurement variable in future research.
Conclusions
Implementing a PA program through active breaks of 20 minutes, including aerobic and strength exercise, at least three times per week is beneficial for increasing the MVPA, decreasing sedentary levels, and improving either workers’ health or WA. Moreover, underpinning PA interventions with the SCT-aligned BCTs seem to be effective for achieving high adherence, motivation, and social relationships of workers.
Ethics statement
The protocol received approval from the Clinical Research Ethics Committee of the University Health Service, Spain based on the latest version of the Declaration of Helsinki (Ref.: 742/01072021). Written informed consent was obtained from all participants prior to data collection.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
This paper has been made possible thanks to the Spanish Ministry of Science, Innovation and Universities and the Formation of University Teachers (grant number: FPU19/00146). In addition, this research has been developed with the help of Grant EQC2019-005843-P, funded by MCIN/AEI/10.13039/501100011033 and ERDF, ‘A Way of Making Europe’.