
Abstract
BACKGROUND:
Work-related musculoskeletal disorders (WRMSDs) remain a challenge despite research aimed at improving their prevention and treatment. Extrinsic feedback has been suggested for the prevention and rehabilitation of WRMSDs to improve sensorimotor control, and ultimately to reduce pain and disability. However, there are few systematic reviews on the effectiveness of extrinsic feedback for WRMSDs.
OBJECTIVE:
To perform a systematic review investigating the effect of extrinsic feedback for the prevention and rehabilitation of WRMSDs.
METHODS:
Five databases (CINAHL, Embase, Ergonomics Abstract, PsycInfo, PubMed) were searched. Studies of various designs assessing the effects of extrinsic feedback during work tasks on three outcomes (function, symptoms, sensorimotor control) in the context of prevention and rehabilitation of WRMSDs were included.
RESULTS:
Forty-nine studies were included, for a total sample of 3387 participants (including 925 injured) who performed work-related tasks in the workplace (27 studies) or in controlled environments (22 studies). The use of extrinsic feedback was shown to be effective in controlled environments for short-term prevention of functional limitations and sensorimotor alterations (very limited to moderate evidence) and for improving, in injured participants, function, symptoms and sensorimotor control (moderate evidence). In the workplace, it was shown to be effective for short-term prevention of functional limitations (limited evidence). There was conflicting evidence regarding its effect for WRMSD rehabilitation in the workplace.
CONCLUSION:
Extrinsic feedback is an interesting complementary tool for the prevention and rehabilitation of WRMSDs in controlled environments. More evidence is needed regarding its effect for the prevention and rehabilitation of WRMSDs in the workplace.
Introduction
Despite research aimed at improving their prevention and treatment, work-related musculoskeletal disorders (WRMSDs) continue to cause significant economic, social and individual burdens [1]. WRMSDs are challenging due to the multifactorial risk factors associated with their development and persistence (e.g., physical work demands, poor posture, altered sensorimotor control, biopsychosocial context) [2]. Previous systematic reviews on WRMSDs have mainly focused on specific treatments against pain [3, 4] and stiffness [5], neglecting other impairments that could explain their high prevalence and rate of chronicity, such as sensorimotor disturbance.
Sensorimotor disturbance is a discordance between motor output and peripherical feedback [6]. It may modulate pain sensation [6] and movement control [7, 8] due to changes in the central nervous system [9, 10]. Outcomes related to sensorimotor disturbance may be important to consider, as recent publications have promoted sensorimotor rehabilitation for musculoskeletal disorders [11, 12]. Therefore, awareness of sensorimotor disturbances could be key for the prevention and rehabilitation of WRMSDs. The use of extrinsic feedback has been proposed as a good option to decrease sensorimotor disturbance, and thus improve movement control [13, 14].
Feedback is described as sensory afferent information resulting from the movement of our body in relation to the environment [14]. Intrinsic (or internal, or proprioception) feedback refers to the brain’s awareness of somatic information occurring during movement, while extrinsic (or augmented) feedback is defined as external information provided by a third party regarding movement outcomes or how the movement is performed [15]. Using extrinsic feedback can enhance intrinsic feedback and help people learn and improve their motor skills [13]. Extrinsic feedback (referred to as “feedback” for the rest of this manuscript) can be produced from various sources: health professionals (e.g., therapists providing manual or auditory feedback), “simple” interface (e.g., mirror, videos) or sensors (e.g., surface electromyography [sEMG], inertial measurement units [IMUs]). Feedback can be delivered using different sensory modalities such as audio (e.g., voice or alarm), visual, or tactile modalities individually or in combination. They can also be set at various frequencies: continuous, intermittent or faded, during or after a task [16, 17]. In addition, feedback can be self-controlled or imposed by a health professional [17]. Finally, feedback provided to the individual can relate either to the movement outcome (e.g., accuracy, time) at the end of the task (knowledge of results[KR]) or to movement characteristics (e.g., joint angle, muscle activation) during the task (knowledge of performance [KP]) [13].
Three previous systematic reviews explored the effect of feedback for the prevention or rehabilitation of WRMSDs, but these reviews only targeted the upper extremities. Two systematic reviews [18, 19] found conflicting effects of feedback for prevention, while one systematic review found no effect for workplace rehabilitation [20]. The interpretation of these results is limited due a lack of studies (total of six included studies for the three systematic reviews), the various outcomes evaluated, and their focus on the upper extremity only. Evaluating the effectiveness of feedback in prevention and treatment of WRMSDs with common comparison variables (function, symptoms, sensorimotor control) could lead to more optimal use of feedback by rehabilitation professionals.
The main objective of this systematic review was to determine whether feedback is effective in the prevention and rehabilitation of WRMSDs by evaluating its effects on function (e.g., work ability, disabilities), symptoms (e.g., discomfort, pain) and sensorimotor control (e.g., posture, muscle activation) in individuals with and without WRMSDs.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) [21] statement and registered on PROSPERO (CRD42020188863).
The search strategy was developed in collaboration with a university librarian. Five bibliographic databases (CINAHL, Embase, Ergonomics Abstract, PsycInfo, PubMed) were searched from inception to August 2022 (2022/08/02). Specific search strategies were developed in OVID (for PubMed, PsycInfo), Embase and EBSCO (for CINAHL, Ergonomics Abstracts) using Medical Subject Headings (MeSH) and free text. Three concepts were exploited for the database search: (1) Population: workers with or without WRMSDs or healthy people performing work-related tasks, AND (2) Intervention: prevention or rehabilitation, AND (3) Modality: feedback. The screening and management of duplicates were performed using Covidence [22], an online software for systematic reviews.
All titles and abstracts were screened independently by two authors using the following inclusion criteria: 1) study design: cross-sectional studies, prospective studies, quasi-randomized controlled studies, cross-over studies, randomized controlled trials; 2) population: individuals with or without WRMSDs; 3) setting: work tasks performed in a work environment or in a controlled environment (e.g., laboratory, clinics, home); 4) intervention: any prevention or rehabilitation intervention using feedback; 5) outcome measures: function, symptoms and sensorimotor control.
Two reviewers (AF and MH or CP or EC) independently screened the titles and abstracts of all retrieved articles, then screened full-text articles. In the case of disagreements, a consensus was reached by discussion, or a third reviewer (JSR) was consulted if needed. Study data were extracted by the first reviewer (AF) and audited for accuracy by a second reviewer (MH or CP). A data extraction form was created, and the data extracted included study design, intervention, characteristics of feedback studied, location of MSK injury (if any), clinical stage (prevention, acute, chronic), research setting, work activity level (sedentary, physical, mixed [23]), outcome measures, and results.
Two reviewers (AF and MH or CP) independently assessed the risk of bias and the quality of evidence using the Downs and Black checklist [24] and a consensus was reached for the final score. Any disagreements were resolved through discussion. The pre-consensus inter-rater agreement between reviewers for total scores was calculated using Gwet’s gamma coefficient [25] and the intraclass correlation coefficient (ICC). The Downs and Black checklist evaluates risk of bias using a 27-item scale in three domains: reporting, external validity, and internal validity. It has good inter-rater reliability (ICC 0.73 to 0.94) [26, 27]. The maximal score that corresponds with a minimal risk of bias is 28. Articles with scores >20 are considered strong, 14–20 moderate, 7–13 limited and <7 poor [28].
Two reviewers (AF and MH or CP) used the GRADE (Grading of Recommendations, Assessment, Development and Evaluations) qualitative approach [29] to determine the overall quality of evidence (Table 3) [30, 31]. Four domains were used to characterize the evidence of each outcome: 1) number of studies/participants (imprecision); 2) methodological quality (risk of bias); 3) methodological and outcome similarities (indirectness); and 4) direction of results (inconsistency) [32]. Quality of evidence is rated using a five-level classification system. Strong evidence was characterized by multiple high-quality studies with consistent results; moderate evidence was characterized by multiple studies including at least one high quality study or multiple moderate or low-quality studies presenting consistent results; limited evidence was characterized by multiple moderate quality or low-quality studies with inconsistent results, or one high quality study; very limited evidence was characterized by only one low or moderate quality study; conflicting evidence was characterized by multiple studies providing inconsistent results, regardless of the methodological quality.
Narrative reporting was used to synthesize results (see Table 1). Table 2 presents description of the various scales used as outcome measures in the included studies.
Synthesis of the articles included
Synthesis of the articles included
Descriptions of the various scales used as outcome measures in the included studies
The database search yielded 4,931 articles after removing duplicates. After full text analysis, 49 studies were included (See Fig. 1 and Table 1). There were 14 cross-sectional laboratory studies (CSLS), 2 cross-sectional workplace studies, 11 prospective cohort studies (PCS), 1 crossover study, 2 pilot randomized controlled trials (RCT), 1 pseudo RCT and 18 RCT. The studies enrolled healthy participants who performed tasks in controlled environments (n = 16) or in the workplace (n = 15), and/or injured workers who performed tasks in the workplace (n = 10) and controlled environments (n = 5). Three studies included both healthy and injured participants in the workplace. Work activity levels were sedentary (e.g., static sitting or standing position, n = 31), physical (n = 11), mixed or nonspecific (n = 7) (See Table 1, Fig. 2). Feedback focused on the neck and upper extremities (n = 24), low back (n = 16), lower extremities (n = 1), and mixed or nonspecific locations (n = 8). The total number of participants was 3387: 2204 healthy, 925 injured, and 258 undefined participants. The main sources of feedback used included sEMG (n = 14), IMUs (n = 11), and cranio-cervical pressure (n = 4), while 5 studies mixed two sources of feedback. The feedback sensory modalities used were audio (n = 8), tactile (n = 10), visual (n = 9), mixed (n = 12), and two studies compared the effects of different sensory modalities [33, 34] (See Fig. 2). The frequency of the feedback was continuous (n = 14), intermittent (n = 21), final (n = 4), mixed (n = 10), and two studies compared the effects of different frequencies of feedback [34, 35] (See Fig. 2). The delivered feedback pertained to the knowledge of performance (n = 40) or results (n = 9), and one study compared the effects of different methods of delivery [33]. Studies explored the effects of the feedback intervention alone (n = 35) or in combination with other interventions (exercise n = 7, ergonomic adjustments n = 7). The effect of feedback was evaluated during (n = 8), just after the intervention (n = 34), in the short term (<2 months, n = 17), in the midterm (<6 months, n = 9), and in the long term (≥6 months, n = 9).
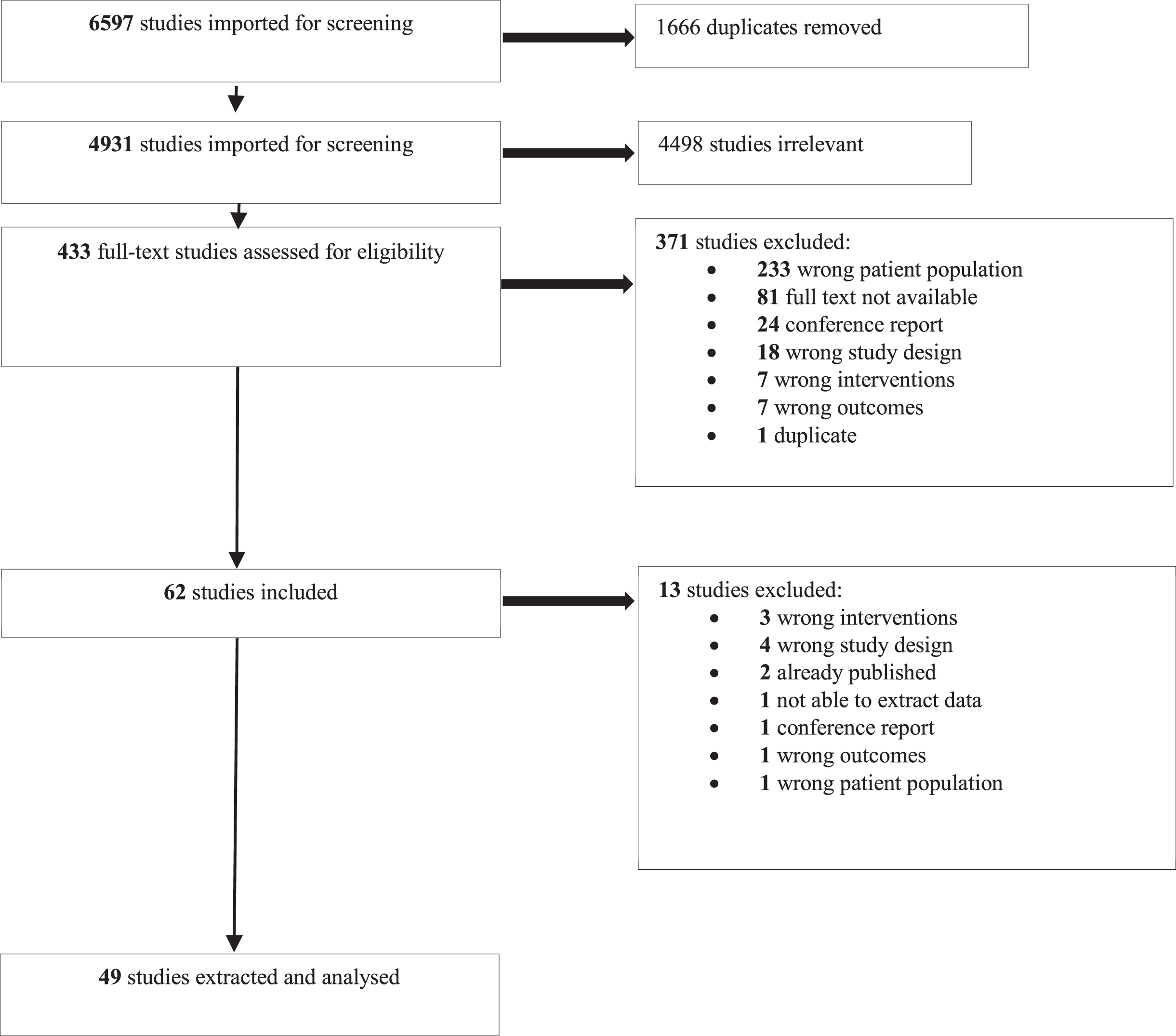
Study flowchart.
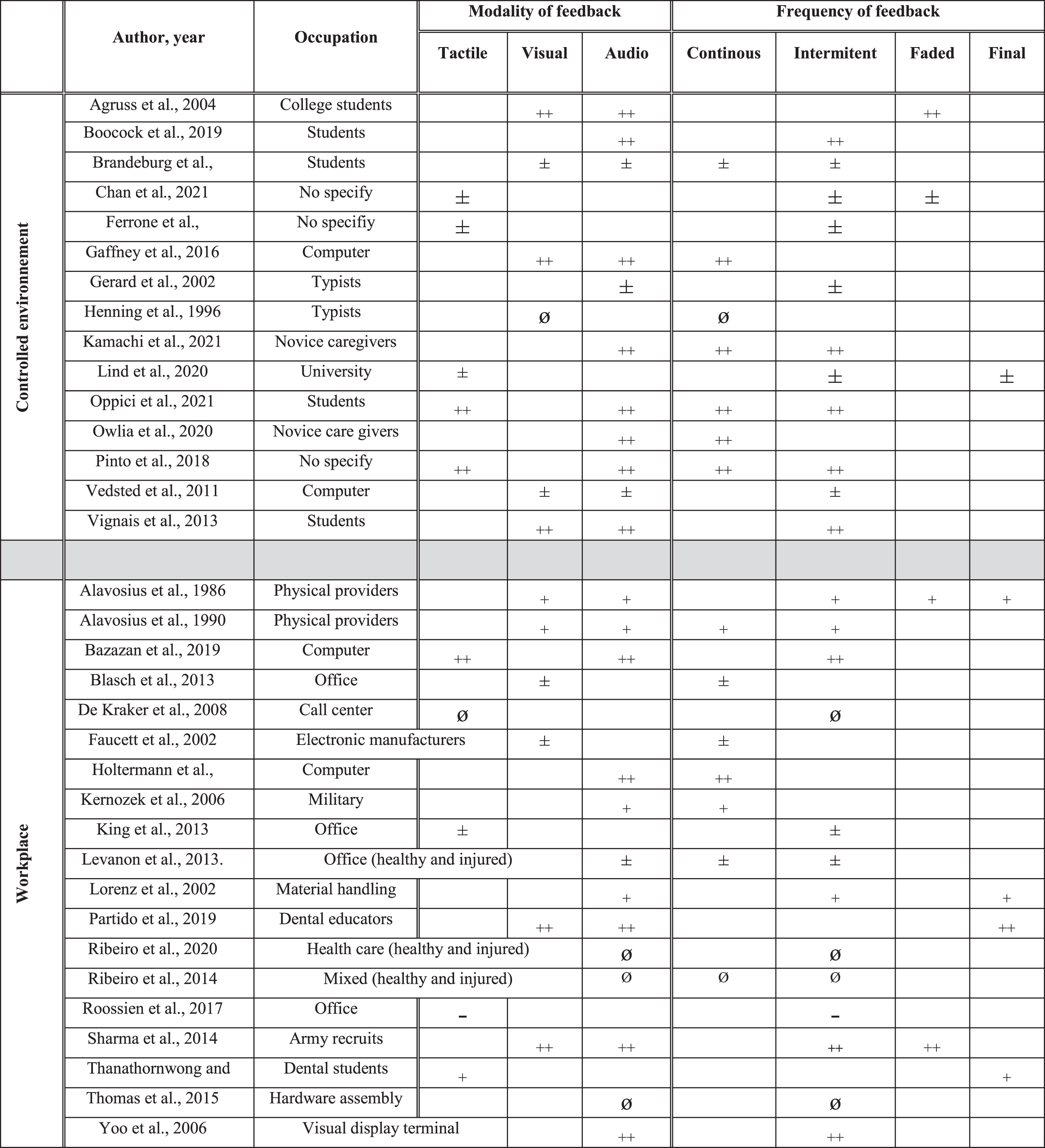
Occupation, modality and frequency of feedback and their effects in prevention. ++: effect superior compared to another intervention or to a control group. +: positive effect (not compared to another intervention). ±: partial positive effect. ∅: inferior or no additional positive effect compared to another intervention. -: negative effect.
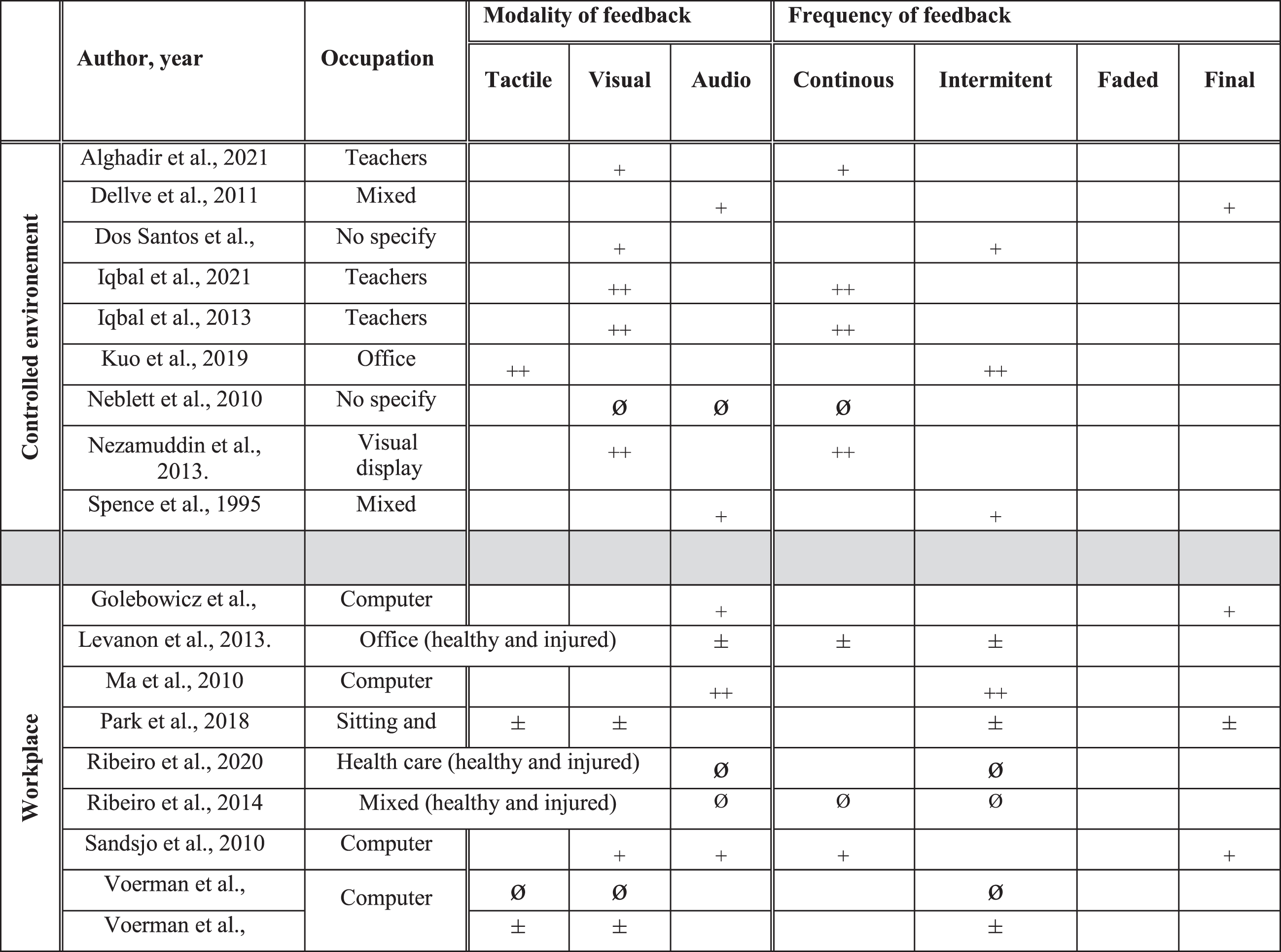
Occupation, modality and frequency of feedback and their effects in rehabilitation. ++: effect superior compared to another intervention or to a control group. +: positive effect (not compared to another intervention). ±: partial positive effect. ∅: inferior or no additional positive effect compared to another intervention.
The pre-consensus inter-rater agreement was considered good between reviewers for each item (Gwet’s gamma coefficient = 0.84) and for total scores of the Downs and Black checklist (ICC = 0.86). Fourteen studies were of limited quality, 32 were of moderate quality, and 3 were of strongquality.
Results are organized by stage (prevention, rehabilitation), environment (controlled, workplace) and outcomes (function, symptoms, sensorimotor control). For each outcome, the studies are organized by work type (in terms of activity level) and type of effect (positive, null, negative). For each study, the p value, the study design and risk of bias are indicated. For details on the type of feedback used, see Table 1 and Fig. 2, for the synthesis of the body of evidence see Table 3.
Synthesis of body of evidence by outcome (function, symptoms and sensory-motor control) in prevention (CSS: cross-sectional study, LB: low back, LL: lower limb, LQ: low quality, M: mixed, MQ: moderate quality, NUL: neck and upper limb, NSP: not specified, NS: not significant, PCS: prospective cohort study, P: physical, PQ: poor quality, RCT: randomized controlled trial, S: significant, Se: sedentary, SQ: strong quality, T0: just after intervention)
Synthesis of body of evidence by outcome in rehabilitation (CSS: cross-sectional study, LB: low back, LL: lower limb, LQ: low quality, M: mixed, MQ: moderate quality, NUL: neck and upper limb, NSP: not specified, NS: not significant, PCS: prospective cohort study, P: physical, PQ: poor quality, RCT: randomized controlled trial, S: significant, Se: sedentary, SQ: strong quality, T0: just after intervention)
The body of evidence on the effect of feedback for prevention in controlled environments on function (one study, total of 12 participants) is considered very limited and suggests a positive effect. The single study on this topic found a positive effect: audio and visual feedback based on a computerized Rapid Upper Limb Assessment (RULA) [36] led to a decrease in injury risk during four simulated industrial manufacturing tasks (p < 0.05, CSLS, LQ)[37].
The body of evidence on the effect of feedback for prevention in controlled environments on symptoms (4 studies, total of 75 participants) is considered conflicting. Two studies found positive effects. During typing tasks, the addition of rest breaks to work time, using a visual display to manage the length of rest breaks, led to a decrease in low back discomfort during a cognitive task, but not during a standard condition (p < 0.05, CSLS, LQ) [38]. During a screwdriving task, the use of a mirror to improve neck posture reduced discomfort; the addition of a verbal reinforcement by a researcher caused no further reduction (p < 0.05, CSLS, LQ) [33]. In two other studies, the use of feedback had no effect on musculoskeletal symptoms. Auditory feedback based on finger sEMG or on keyboard force monitors did not influence pain during a typing task (p < 0.05, PCS, MQ) [39]. Instructions with or without vibration feedback to reduce adverse arm movements and posture during mail sorting tasks did not influence symptoms (CSLS, MQ) [40].
The body of evidence on the effect of feedback for prevention in controlled environments on sensorimotor control is considered moderate and suggests positive effects (twelve studies, total of 264 participants). The 12 studies found positive effects. During computer tasks, audio and visual feedback based on sEMG led to a decrease in muscle activity (p < 0.05; PCS, MD; CSLS, LQ) [39, 41]. The addition of continuous visual feedback (based on high density sEMG) to verbal feedback related to posture also led to a change in the spatial distribution of trapezius activity and in shoulder position (p < 0.05, CSLS, LQ) [42]. The addition of vibration feedback based on IMUs to verbal feedback also led to a decrease in arm elevation during mail sorting tasks (p < 0.005, CSLS, MQ) [40]. Various types of feedback led to improved lumbar posture during handling tasks: audio feedback based on lumbar IMUs to assess lumbar flexion (p < 0.05, CSLS, MQs) [43, 44], lumbar rigid strapping tape (p < 0.0001, CSLS, LQ) [45], final faded verbal feedback (based on 3D motion analysis), intermittent audio feedback based on sEMG to reduce lumbosacral compression (p < 0.01, CSLS, MQ) [46], and intermittent vibration feedback and terminal verbal feedback (based on 3D motion analysis, p < 0.005, CSS, MQ) [47]. During repetitive lifting tasks, auditory feedback (based on 3D motion analysis) led to decrease sacro-lumbar peak flexion more than continuous tactile feedback (based on tape applied, p < 0.05, CSS, MQ) [34]. In addition during care tasks, intermittent haptic or faded intermittent auditory feedback (based on IMUs) led to improve lumbar posture in forward/backward (p < 0.05, PCS, LQ) [48, 49].
The body of evidence on the effect of feedback for prevention in the workplace on function is considered limited and suggests a positive effect (six studies, 473 participants). The six included studies found positive effects. Audio or vibration feedback based on IMUs to control upper-back posture in control room operators led to a decrease in RULA scores in the long term (p < 0.05, RCT, MQ) [50]. In dental educators aiming to self-evaluate specific ergonomic criteria, the addition of feedback that was based on pictures of posture improved posture ergonomic score more than ergonomic self-assessment [51] alone (F = 6.295, p < 0.01, RCT, MQ) [52]. When verbal and visual feedback on transfer techniques (e.g., knee bending, maintaining a straight spine) was offered by therapists based on a checklist, the percentage of safely performed transfers in residential facilities was significantly increased in the short and long term (p unknown, 2 PCS, LQ [53] and MQ [54]). Pressure sensors (treadmill) feedback in combination with verbal feedback from therapists decreased the incidence of tibial stress syndrome in army recruits (p = 0.05, RCT, MQ) [55]. However, either visual feedback based on sEMG combined with Muscle Learning Therapy [56] or cognitive behavioral techniques were not more effective than application of ergonomics guidelines on the occurrence of upper extremity injuries in electronics manufacturers (p < 0.05, RCT, MQ) [57].
The body of evidence on the effect of feedback for prevention in the workplace on symptoms is considered conflicting (seven studies, 533 participants). Five studies found positive effects. Audio or vibration feedback based on IMUs to assess shoulder and trunk position (Nordic Musculoskeletal Questionnaire, p < 0.05, RCT, MQ) [50], and vibration feedback provided from chair pressure sensors to improve sitting behavior (Localized Musculoskeletal Discomfort [58], p < 0.01, PCS, MQ) [59] led to a decrease in the occurrence of musculoskeletal symptoms. Similarly, use of a vibrating computer mouse to modify hand posture (Daily Symptom Survey [60], p < 0.05, RCT pilot, MQ) [61], and visual feedback based on skin conductance level and finger temperature to assist relaxation and stretching (frequency of symptoms immediately after the intervention and in the mid-term, p < 0.05, pseudo RCT, MQ) [62] in sedentary seated workers led to a decrease in the occurrence of musculoskeletal symptoms. Visual feedback based on sEMG combined with Muscle Learning Therapy decreased upper extremity symptoms (Visual Analog Scale and body chart) in electronic manufacturers compared to cognitive behavioral techniques or ergonomics guidelines in the short term (p < 0.05, RCT, MQ) [57]. However, three studies did not observe such changes in symptoms for types of feedback such as: computer mouse feedback (Localized Musculoskeletal Discomfort, RCT, LQ) [63], feedback based on sEMG alone (audio, body chart, PCS, LQ) [64], or feedback based on sEMG with Muscle Learning Therapy (visual, VAS and body chart, immediately after intervention, in the mid- and long term, RCT, MQ) [57] to discourage awkward hand posture in line workers.
The body of evidence on the effect of feedback for prevention in the workplace on sensorimotor control is considered conflicting (12 studies, total of 1688 participants). Seven studies found positive effects. Vibration feedback from pressure sensors fixed on a chair led to modified sitting (p < 0.05, CSS, MQ) [65], while vibration feedback from one accelerometer on the upper back led to improved posture of dental educators and to a decrease in upper trapezius sEMG (p < 0.05, crossover study, LQ) [66]. Audiovisual feedback based on trapezius sEMG alone (p < 0.05, RCT, MQ) [67] or combined with Muscle Learning Therapy (p < 0.04, RCT, MQ) [57] in office workers led to a decrease in muscle activity. Auditory feedback based on magnetic motion measurement of lumbar moments combined with verbal therapists’ feedback decreased lumbar flexion and side bending torque during material handling (p < 0.05, PCS, MQ [68] and RCT, MQ [69]). Visual feedback based on pressure sensors (in a treadmill) in combination with a therapist’s verbal feedback to prevent tibial stress syndrome improved foot balance and time to reach peak heel rotation in army recruits (p = 0.05, RCT, MQ) [55]. However, five studies did not find any positive effect. Audio feedback based on forearm sEMG did not influence grip strength in electronics manufacturers (PCS, LQ) [64]. Visual feedback based on skin conductance level and finger temperature to assist relaxation and stretching did not influence computer users’ upper trapezius’ sEMG activity (pseudo RCT, MQ) [62]. Vibration feedback, provided by pressure sensors fixed on the operator’s chair, did not modify sitting behaviors (e.g., sitting duration, PCS, MQ) [59]. Computer mouse feedback (vibration), meant to decrease awkward computer mouse hand posture, increased awkwardness of computer mouse hand posture after feedback exposure (p < 0.03, RCT, LQ) [63], (p < 0.05, RCT pilot, MQ) [61].
The body of evidence on the effect of feedback for rehabilitation in controlled environments on function is considered moderate (four studies, 339 participants). All four studies found positive effects. Visual pressure feedback used to manage cranio-cervical flexion exercises in addition to conventional exercises led to greater improvement in teachers’ Neck Disability Index [70] scores after the intervention (p < 0.05, RCT, MQ) [71] and in the short term (p < 0.05, RCT, MQ) [72]. Verbal feedback by a therapist (based on sEMG) led to improved Work Ability Index [73] scores in the short and mid-term follow-ups in a chronic neck pain population (p < 0.05, RCT, MQ) [74]. Intermittent visual feedback (based on sEMG) associated with scapular focused exercises led to improve DASH (Disabilities of the Arm, Shoulder and Hand) [75] and SPADI (Shoulder Pain and Disability Index) [75] scores (p < 0.05, PCS, MQ) [76].
The body of evidence on the effect of feedback for rehabilitation in controlled environments on symptoms is considered moderate (eight studies, 508 participants) and suggests positive effects. Five studies found positive effects. Visual pressure feedback for cranio-cervical flexion exercises in addition to conventional exercises led to a greater decrease in pain (Numeric Pain Rating Scale [77]) than conventional exercises alone [78], in both teachers [71, 72] and visual display terminal workers [79] (p < 0.05, RCTs, MQ and SQ) immediately after the intervention [71, 79] and in the short term (p < 0.05, RCT, MQ) [72]. Feedback based on sEMG alone [74, 80] or in combination with relaxation training [80] in a population of physical and sedentary workers led to a decrease in neck pain (p = 0.05, RCT, MQ, Von Korff rating scale [81]) [74] and in upper extremity pain (p < 0.05, RCT, LQ, Pain Beliefs Questionnaire [82] and Self-Monitored Pain [80]) immediately after the intervention [74, 80] and in the mid-term [74]. Intermittent visual feedback (based on sEMG) associated with scapular focused exercises led to improve NPRS scores (p < 0.05, PCS, MQ) [76]. However, one study concluded that vibration feedback based on IMUs to monitor upper body posture led to an increase in neck and shoulder pain (Numeric Pain Rating Scale) in office workers just after the intervention (p < 0.001, CSLS, MQ) [83].
The body of evidence on the effect of feedback for rehabilitation in controlled environments on sensorimotor control is considered moderate (six studies, total of 539 participants) and suggests positive effects. Three studies found positive effects. Visual pressure feedback for cranio-cervical flexion exercises in addition to conventional exercises led to improved neck muscle endurance compared to conventional exercises alone (p < 0.05, RCT, MQ [71] and RCT, SQ [79]) or cranio vertebral angle (p < 0.05, CSS, MQ) [78]. Vibration feedback based on IMUs to monitor upper body posture led to a decrease in cervical erector spinae sEMG amplitude and to decreased neck and thoracic flexion measured in office workers after the intervention (p < 0.05, CSLS, MQ) [83]. Intermittent visual feedback (based on sEMG) associated with scapular focused exercises led to improve range of motion, strength and neuro muscular control (p < 0.05, PCS, MQ) [76]. However, the addition of visual and audio sEMG feedback to a functional restoration treatment program [84] for low back pain did not lead to greater improvement of muscle relaxation during standing flexion [85] (PCS, SQ) [86].
The body of evidence on the effect of feedback for rehabilitation in the workplace on function is considered conflicting (six studies, 282 participants). Four studies found positive effects. Verbal or visual [87, 88] feedback through telerehabilitation based on upper extremity sEMG data alone [88], or with an ergonomic intervention [87] aiming to increase muscle relaxation, led to decreased physical loading (RULA, p = 0.003, PCS, LQ) [87] and to improved Work Ability Index and Pain Disability Index [89] scores, similarly to effects observed with conventional care, immediately after the intervention and in the short term (p < 0.05, RCT, LQ) [88] in computer operators with neck and shoulder pain. Audio feedback based on sEMG improved computer users’ Neck Disability Index scores more than shoulder muscle strengthening, passive treatment or educational ergonomics booklets (p = 0.012, RCT, MQ) [90]. On the other hand, two studies did not observe any positive effect in computer operators when tactile [91] and audio [69, 91] feedback based on sEMG were added to ergonomics counseling. Outcomes were Pain Disability Index scores immediately after the intervention and in the mid and long term (RCT, MQ) [91], and physical loading (RULA, RCT, SQ) [69].
The body of evidence on the effect of feedback for rehabilitation in the workplace on symptoms is considered conflicting (six studies, 313 participants). Four studies found positive effects. Verbal or visual [87, 88] feedback through telerehabilitation based on upper extremity sEMG data alone [88] or with an ergonomic intervention [87] led to a decrease in pain in the short term (Standard Nordic Questionnaire [92], p = 0.003, PCS, LQ) [87] or an effect similar to conventional care immediately after the intervention and in the short term (Visual Analog Scale, p < 0.05, RCT, LQ) [88]. Audio feedback based on sEMG led to a decrease in computer users’ pain (Visual Analog Scale), more effectively than shoulder muscle strengthening, passive treatment or ergonomics booklets, immediately after the intervention and in the long term (p < 0.05, RCT, MQ) [90]. Visual feedback based on pedometers and vibration based on lumbar posture (IMUs) led to reduced low back pain (Cornell Musculoskeletal Discomfort Questionnaire) after the intervention in standing and sitting workers (p = 0.02, RCT, MQ) [93]. Two studies did not observe such positive effects. In computer workers, the addition of tactile [91] and audio [69, 91] feedback based on sEMG to ergonomics counseling did not significantly influence symptoms immediately after the intervention (Visual Analog Scale, RCT, MQ), in the short term (Standard Nordic Questionnaire, RCT, SQ) [69] or in the long term (Visual Analog Scale, RCT, MQ) [91].
The body of evidence on the effect of feedback for rehabilitation in the workplace on sensorimotor control is considered limited and suggests no effect (five studies, total of 397 participants). One study found positive effects: audio feedback based on sEMG reduced muscle activity of office workers compared to strengthening exercises, passive treatment, or educational ergonomics booklets (p < 0.05, RCT, MQ) [90]. On the other hand, four studies did not observe any positive effect. Continuous or intermittent audio feedback based on IMUs to limit excess forward bending posture did not significantly improve lumbar posture compared to a control group in physically active [35, 94] and sedentary [35] health workers (RCTs, SQ) in the short [35, 94] and long term [94]. The addition of tactile [91] and audio [69, 91] feedback based on sEMG to ergonomics counseling in computer workers did not significantly modify sEMG activity [69, 91] and upper extremity kinematics immediately after the intervention, and in the short (RCT, SQ) [69] and long term (RCT, MQ) [91].
This systematic review of 49 studies offers a large overview of the effects of extrinsic feedback used during simulated or real working tasks in the prevention and rehabilitation of WRMSDs. For the prevention of WRMSDs, findings show that feedback leads to improved function in controlled environments (very limited evidence) and in the workplace (limited evidence), and to improved sensorimotor control in controlled environments (moderate evidence). Its effects on symptoms, however, are conflicting. For the rehabilitation of WRMSDs, feedback mostly had a positive effect on function, symptoms and sensorimotor control (moderate evidence) in controlled environments, while its effects in the workplace were conflicting for function and symptoms and null for sensorimotor control. The lack of studies comparing the different characteristics of feedback (e.g., sensory modalities, frequency) made it impossible to suggest specific feedback. These findings are more exhaustive than previous systematic reviews [18–20] which reported conflicting evidence based on a very small number of studies on the effect of different types of feedback for the upper extremity.
Our review is the first to attempt to address the effects of feedback in two different environments, namely controlled (clinics or research laboratories) and real-world environments (workplace). Specific working tasks (e.g., lifting a patient out of their bed) may not be similarly conducted and experienced by the therapist in controlled environments versus in the workplace. This is due to the possible unforeseen events present in the real world (e.g., medical bed blocked in a low position), work-related fatigue (e.g., therapist may have previously lifted multiple patients), and the biopsychosocial context of the workplace [95–97] (e.g., stress [98], organization [99]). These differences between environments could explain the discrepancy between results obtained in controlled and real environments.
The advantages of using feedback in controlled environments are isolation of the specific working task and, hopefully, improvement of movement quality. The positive outcomes conclusions reported in controlled environments show the clinical relevance of using feedback in clinics as their use in the included studies can be compared to a typical session in the clinic where clinicians use external feedback during movement or task simulations. Although multiple devices or sensors can be used to give feedback to patients, there are various non-technological types of feedback that can easily be used by clinicians. Examples include ergonomics counseling (verbal feedback) based on the therapist’s observations or based on a checklist, visual feedback based on cranio-cervical flexion pressure, and tactile feedback from rigid strapping tape to improve posture sensation. Therapists can therefore use feedback in their clinical practice to prevent or decrease pain and disability, and to optimize sensorimotor control during simulated work tasks before returning to work.
Feedback could be a useful tool in the prevention of WRMSDs, as certain studies in controlled environments have shown that it may reduce factors associated with the development of WRMSDs, e.g., decreased muscle activity during computer tasks or reduced lumbosacral compression during lifting tasks. These results are in line with findings concerning the use of feedback for the prevention of sport-related injuries. Examples include using feedback for gait retraining in runners [100] (leading to reduced ground reaction force variables) or for modifying jump-landing technique for the prevention of anterior cruciate ligament injury [101] (leading to reduced vertical ground reaction forces and knee abduction/flexion angle).
However, most WRMSDs develop gradually, over several months or years, due to repetitive movements, sustained posture or exposure to stress [2, 102]. The lack of high-quality, long-term studies evaluating the effect of feedback for the prevention of WRMSDs in the workplace prevents us from concluding on the potential of feedback to decrease the prevalence of WRMSDs. In addition, most included studies recruited young, healthy individuals without any symptoms, who had fewer risk factors for developing WRMSDs [103], and only a small margin for the outcomes progression. Further long-term longitudinal studies with workers should be conducted to determine whether feedback can be used for the prevention of WRMSDs.
The effect of feedback in the workplace was found to be null to very limited. These results are not surprising as several studies compared feedback to ergonomic adjustment and demonstrated the superiority of ergonomic adjustment in the workplace. By optimizing the working environment according to the physical characteristics of the worker, ergonomic adjustment is the most comprehensive, simple and effective intervention in the workplace to correct posture or movement [20, 105]. Feedback, perceived as a more complex intervention by workers, should be used once work ergonomics have been optimized. Further studies could explore the value of adding feedback after ergonomic interventions.
The findings of this systematic review allow us to propose different clinical implications. Firstly, feedback can be used to preserve function in both controlled (very limited evidence) and work (moderate evidence) environments, and to improve/preserve sensorimotor control in controlled environments (moderate evidence). Secondly, clinicians can include interventions using feedback in controlled environments, as they have been shown to reduce symptoms and enhance function and sensorimotor control. Thirdly, feedback alone is not indicated for the rehabilitation of WRMSDs in the workplace as ergonomic adjustment should be performed first. More evidence is needed from long term studies before recommending the use of feedback for WRMSD prevention or in workplace rehabilitation as a complement to ergonomic interventions.
The main source of limitations in this systematic review is the heterogeneity of the included studies which prevented us from concluding on the specific effects of the different types of feedback (for instance, whether faded verbal feedback is more effective than continuous verbal feedback for pain prevention) and from performing meta-analyses. In addition, the lack of RCT and high-quality studies decreased the level of evidence and the possibility of producing clear recommendations. Still, the inclusion of cross-sectional and non-randomized studies allowed us to explore the effect of feedback on various body regions and environments. Moreover, 17 of the 43 included studies combined verbal feedback with another feedback modality, without assessing the effect of each type of feedback. Therefore, it is impossible to determine whether the use of a second type of feedback contributed to the observed outcomes. Finally, the paucity of studies with long-term assessments only allowed us to conclude on the immediate and short-term effects of feedback.
Conclusion
Extrinsic feedback is a valuable complementary tool for the management of WRMSDs and future studies should further evaluate its clinical applications in prevention and workplace rehabilitation.
Ethical approval
Not applicable (systematic review).
Informed consent
Not applicable (systematic review).
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors would like to thank Marie-Marthe Gagnon, librarian, for her assistance in database searches, Isabelle Poitras for her advice and Émilie Champagne for her involvement.
Funding
AF is supported by a scholarship the Fonds de recherche du Québec-Santé. J-SR is supported by a career award from the Fonds de recherche du Québec-Santé.