
Abstract
BACKGROUND:
The outbreak of COVID-19 and its associated measures has resulted in a sizeable working population transitioning to working from home (WFH), bringing additional challenges, and increasing work-related stress. Research has indicated that yoga has promising potential in reducing stress in the workplace. However, there are very few studies exploring the impact of online streamed yoga on stress management for people-WFH.
OBJECTIVE:
To investigate the feasibility and outcome of an online streamed yoga intervention on stress and wellbeing of people-WFH during COVID-19.
METHODS:
A six-week pilot randomized controlled trial (RCT) yoga intervention was designed with yoga (n = 26) and a wait-list control group (n = 26). A mixed two-way ANOVA was used to assess changes in standardised outcome measures at baseline and post-intervention. Likert and open-ended questions assessed enjoyment, acceptability and perceived benefits of the program, which were analysed thematically.
RESULTS:
Compared with the control, the yoga group reported significant improvements in perceived stress, mental wellbeing, depression and coping self-efficacy, but not stress and anxiety. Participants experienced physical and mental health benefits and reported high acceptability and enjoyment of the intervention.
CONCLUSIONS:
An online yoga intervention can help people WFH manage stress and enhance wellbeing and coping abilities.
Introduction
The World Health Organization (WHO) defines work-related stress as “the response people may have when presented with work demands and pressures that are not matched to their knowledge and abilities and which challenge their ability to cope” [1, p.424]. In contrast wellbeing at work is defined as building an atmosphere to foster a state of contentment that enables employees to thrive and to realise their full potential for their own good and for their organisation [2]. Long-standing and unattended stress can have adverse effects on an employee’s mental and physical health along with outcomes related to the organisation such as employee absenteeism, employee disability claims, and lost productivity [3]. Workplace stress has been consistently associated with cardiovascular disease [4, 5], psychosomatic problems, musculoskeletal disorders [6], mental health problems [7, 8], and non-adaptive HPA axis [9], cardiovascular [10] and immune responses [9].
Mental health in the workplace is increasingly a problem, and with 32.5 million people aged 16 to 64 in employment in the United Kingdom (UK), 75.3% of its working population [11], the cost to the UK economy is estimated to be up to £99 billion each year [12]. Mental health problems have been deemed as having a more significant impact on people’s ability to work in comparison to any other group of disorders [13].
In 2020, the American Psychological Association, revealed that 64% of employed adults reported work as a source of stress in the US with serious consequences for years to come due to COVID-19 [14]. Workplace stress is one of the most significant problems facing the organisations across Europe [15]. In 2019/20, 828,000 workers reported suffering from work related stress, depression or anxiety, which contributed to a loss of 17.9 million working days in the UK [16]. In the same period, work-related stress, anxiety or depression accounted for 51 per cent of all the cases of work-related ill health in Britain [16]. A survey (n = 1815) found that these numbers have exponentially increased, with 79% of British adults in employment commonly experiencing work-related stress in 2020 [17]. One in eight of the current employees in the UK reported having a mental health condition, and 42% of employees felt their health condition affected their work a great deal or up to some extent [18].
Many non-pharmacological interventions have been tested to address the problem of workplace stress, including mind-body and mindfulness interventions. The literature related to mind-body stress reduction is continuously evolving in the field of workplace wellness and simultaneously in clinical populations. Several recent systematic reviews and meta-analyses have reported beneficial effects of mindfulness-based stress reduction (MBSR) interventions in improving mental health for employees at a workplace setting [19], nurses [21], psychological functioning of employees [20], and reducing stress in physicians and medical students [22]. However, several studies have also reported association of mindfulness/meditation with exacerbated mental health issues such as depression, anxiety, perceived stress and adverse effects like negativity, disorientation, addiction to meditation, worsened relationships, and hypersensitivity [23–25]. MBSR interventions include mindfulness performance of hatha yoga postures as one of the components [26], with yoga demonstrating the most benefit in several populations [27, 28].
It is suggested that the practice of yoga is a natural way to engender mindfulness, as attention is focussed on the present moment, in part due to the intensity of the bodily sensations [19]. Poses (asana) are usually practised with slow controlled breathing which activates the parasympathetic response thereby inducing relaxation which helps an individual remain with the experience while simultaneously inhibiting negative cognitions [20]. It has been demonstrated that yogic breathing techniques (pranayama) can facilitate increased vagal tone also activating parasympathetic response [20]. Therefore, asana and pranayama can support mindfulness through body awareness as well as by strengthening positive neuroplasticity in higher brain structures [21].
Yoga is an ancient and comprehensive mind-body practice originating in India, encompassing all facets of the human existence: spirituality, psychology, philosophy and physiology [20]. It has gained in popularity mainly because of its therapeutic health benefits, both physical and mental [22–24]. Yoga-based practices such as postures, breathing techniques and meditation (dhyana) are defined as psychophysiological therapeutic practices that use several of these techniques inspired by a variety of yogic traditions [19]. There is accumulating research vouching for the promising potential of the therapeutic application of yoga in health management and mental health care. A few systematic reviews and meta-analyses have revealed positive effect of yoga interventions on mental health conditions [25, 26], structures and functions of brain [27], cardio-metabolic health [28], menopausal symptoms [29], osteoarthritis [30], COPD [31], chronic non-specific neck pain [32], among other conditions.
The practise of yoga for therapeutic benefits is increasingly gaining popularity in the UK. A cross-sectional survey reported the perception of yoga as having a positive impact on mental and physical health conditions and an association with positive health behaviours [24]. Thus, based on ever-increasing evidence, it is not surprising that research has indicated the potential of yoga in improving workplace stress and wellbeing. The National Institute for Health and Clinical Excellence (NICE) has recommended an increase in levels of physical activity at the workplace to improve wellbeing [33]. Increased physical activity has been found to have an association with lower job burnout, lower levels of depression [34] and lower physiological stress outside work [35]. A cohort study revealed that chronic workplace stress could lead to an increase in physical inactivity [36]. Moreover, several studies suggest that we have been living in a pandemic of physical inactivity and sedentary behaviour for many years [37–39], with COVID-19 threatening to increase this [40].
Yoga has demonstrated promising potential in combating stress in the workplace and increasing physical activity as evidenced by two recent systematic reviews. Della Valle and colleagues in their recent meta-analysis of six RCTs, found workplace yoga interventions to be more effective in comparison to no intervention in workplace stress management [41]. Puerto Valencia and colleagues in their systematic review of 13 RCTs revealed that yoga had a positive effect on health in the workplace, particularly in reducing stress, with no adverse effects reported [42]. Wolever and colleagues found that both mindfulness-based, and therapeutic yoga programs could provide effective interventions in alleviating stress in employees [43]. A review of 56 studies found that workplace stress can also lead to musculoskeletal symptoms especially of back, neck and shoulders [44] and yoga can help deal with stress-induced musculoskeletal symptoms of the neck [45], back [46], and shoulders [47], among other symptoms.
The outbreak of COVID-19 and associated social distancing measures has resulted in a sizeable working population transitioning to working from home whilst concurrently managing family life, which can increase daytime stress, anxiety and depression levels, and also disrupt sleep [48]. A recent survey found additional challenges, such as lack of social contact, issues with work-life balance, and difficulty focusing; and for people with children younger than twelve the biggest challenges were increased household and care responsibilities [49]. Workplace stress ‘pre-COVID-19’ had already been identified as one of the major causes of low job performance, lack of motivation, low morale, low output and organisational sabotage [50]. Current circumstances have further accentuated this situation with new challenges like zoom fatigue (emotional and physical exhaustion caused by video conferencing), inability to unplug after office hours, difficulties communicating with colleagues, increased stress, and decreased mental health [48, 51–54].
The culture of homeworking was on gradual, although slow, rise even before lockdown in the UK. It tripled from 1.5% in 1981 to 4.7% in 2019, but rose substantially during the lockdown with an eightfold rise from 5.7% in January/February 2020 to 43.1% in April 2020 and even though there was decline by June 2020, it continues to remain high at 36.5% [55]. A survey from the British Council of Offices discovered that pandemic has changed working patterns for good with almost half of the employees (46%) eager to split their time between homes and workplaces in future [56]. Another survey by the Institute of Directors revealed that three quarters of the directors predicted increased homeworking and more than half are planning to decrease their long-term use of workplaces [57]. One study also suggested that more than 40% of jobs can be performed at home in the UK [58]. Therefore, in the future, due to unpredictable circumstances of COVID-19 and inclination of both employers and employees toward a balanced approach, we may have a ‘mixed’ workforce working both ‘on-site’ and from home leading to long-term changes to working practices.
A yoga-based lifestyle has been recommended by the Government of India and various yoga organisations worldwide to help people remain healthy and promote optimal immune functions during the COVID-19 pandemic [59, 60]. In the wake of COVID-19 imposed social distancing measures, most of the fitness industry has moved to the online delivery of their programs, the popular virtual workouts app ‘Mindbody’ revealed yoga as the most popular virtual class booked with 32% of virtual bookings with an average of nearly 22,000 yoga bookings per day [61]. The delivery of mind-body programs online can help overcome barriers to participation because these programs can be accessed at convenient times, participants can work through recordings at their own pace, and maintain privacy [62]. Web-based interventions also offer benefits of cost-effectiveness for both participants and instructors related to traveling, high scalability and ease of access [63]. Nonetheless, there are some limitations of online yoga such as the lack of opportunities for instructors to adjust participants, lack of social connection, technical issues and difficulty in following the instructor [64].
There are, however, very few studies exploring the impact of the online mode of delivery or comparison with face-to-face (ftf) delivery. Research on online yoga is scant, more so on its potential to alleviate stress among people working from home. However, online mind-body interventions have been found to show promising potential in alleviating stress and enhancing wellbeing among various population groups. In a review and meta-analysis of 15 RCTs, Spijkerman and colleagues indicated the promising potential of online mind-body interventions in improving mental health outcomes, particularly stress in various population groups including employees [65]. Several other studies point to the benefits of online yoga interventions, including stress reduction and improved coping skills among nurse-midwives [66], a reduction of depression and grief in mothers who experienced stillbirth [64], improved physical and mental wellbeing in university students [67], and improved psychological outcomes in adults with cancer [68]. These studies also indicated the potential of the online mode of delivery to increase access, being convenient in terms of time and portability of devices e.g., smartphones, laptops or tablets and the opportunity to practise in privacy if desired.
Existing studies comparing ftf and online yoga/mindfulness interventions have found no differences in effectiveness or acceptability [43, 69]. Barak et al. (2008) in their comprehensive review and meta-analysis of internet-based psycho-therapeutic interventions, showed that there is no difference in effectiveness when compared to ftf interventions and in some cases internet-based interventions has been rated as superior by clients [70]. However, more research is needed to explore the acceptability and benefits of online yoga/mindfulness interventions in the context of working individuals. In the current circumstances of continued, changeable social distancing measures, it is pertinent to look at remote delivery of yoga interventions for people working from home.
One major limitation in evaluating yoga studies’ impact on any physiological or psychological condition is non-consensus on dosage of intervention to achieve desired outcomes i.e., number of days and hours per week and duration of the intervention [71]. Wolever and Hartfiel in their separate workplace studies for stress reduction delivered a yoga intervention for 50 to 60 minutes weekly or twice weekly for eight to twelve weeks [43, 72]. Sherman (2012) reported a trend of classes in western studies lasting between 60 to 90 minutes – weekly or twice weekly [71]. However, a survey of 24 yoga teachers with expertise in applying yoga to address mental health conditions revealed that practice should consist of five 30–40 minutes sessions per week for at least six weeks for improving anxiety [73]. Traditional Yogic texts and scriptures also allude to the benefits of practice for longer durations and its regularity [74]. Therefore, it is possible that longer interventions with higher frequencies of classes per week could be beneficial for alleviating mental health conditions.
In summary, there are limitations in the current literature which this pilot study aims to address. The extant literature measuring the effects of online mode of delivery scarcely consider the workplace. Furthermore, all existing studies were conducted with nurses, students or patients rather than the general working population, with an inadequate explanation of yogic components (e.g., poses, breathing techniques, and meditation), their techniques (how they were performed?), and rationale (why they were performed?).
This study investigated whether an online streamed yoga intervention reduces stress and increases mental wellbeing in people working from home. It was hypothesized that online streamed yoga would lead to increase in mental wellbeing and coping self-efficacy and decreases in perceived stress, anxiety and depression compared with a control group. We also explored qualitatively yoga group participants’ experiences of the intervention and the acceptability of an online synchronous program.
Methods
Study design
This pilot study used a randomized wait-list control design comparing pre-and post- (six-weeks) intervention scores between and within groups on validated outcome measures. Thematic analysis was performed on open ended questions to analyse prominent themes about participants’ experiences and acceptability of the program.
Participant recruitment
The study received ethical approval from the University of Westminster (ETH1920-0764).
During May and June 2020, employees aged 18 and over, working from home were self-selected via emails sent out during weekly employee communication by corporate organizations and academic institutions based in London. Participant inclusion criteria were: 18 years or older, currently employed, speak and understand English and, not currently practising yoga. Participant exclusion criteria were: a physical/medical condition that would make practising yoga unsafe or not possible, plans to take leave from work during the study and, current mental health diagnosis.
Interested employees were emailed a participant information sheet (PIS) which explained the purpose of the study, and a link to an online screening questionnaire. This invited participants to identify any health concerns from a list of 19 common conditions (e.g., arthritis, asthma, back pain, depression, anxiety, stress, heart conditions, etc.). Completed questionnaires were then assessed by the researcher, an experienced yoga practitioner. The questionnaire also asked participants to rate their self-identified stress levels on the scale of 1 to10 and to indicate if they currently practice yoga or yoga-related activities. Participants who already practised yoga or yoga related activities were excluded from the study to prevent bias.
A total of 60 participants signed up for the study and 52 were electronically randomised into the yoga intervention (n = 26) or wait-list control group (n = 26) – Fig. 1. After randomisation, the intervention group was informed by email of class timings, Zoom meeting links and the nature of the sessions; the control group was informed of post-study Zoom meeting links and class timings by email and were asked not to practice yoga during the six-week period. Upon completion of the study, the control group received five yoga classes and a video of the program. Group membership was not blinded, and all classes were free of charge to participants. Outcome variables were measured at the beginning (baseline) and the end of the program (six weeks later). Informed consent was taken through the consent forms embedded with the baseline questionnaires through the Qualtrics link.
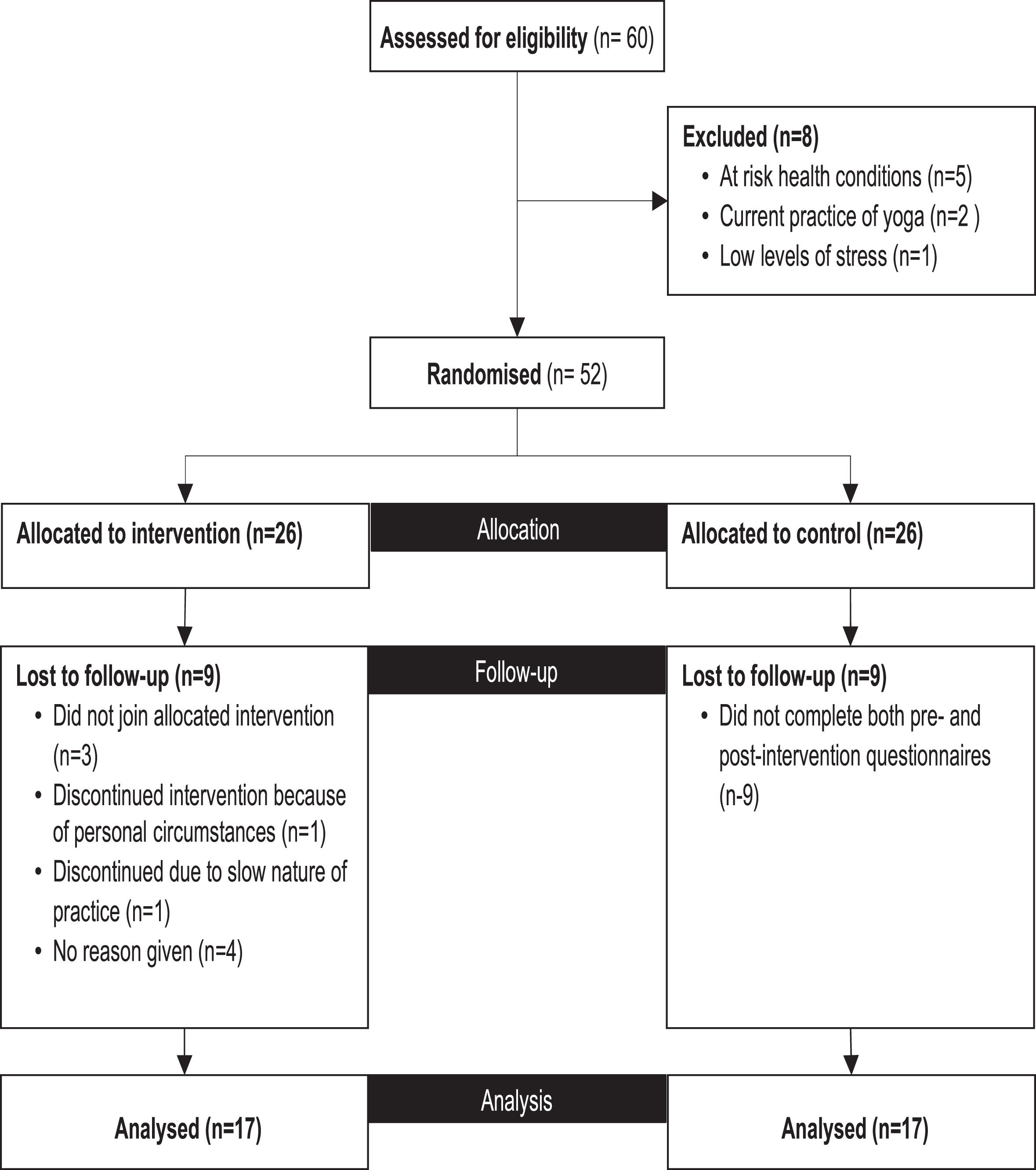
Recruitment flow chart.
This pilot study was conducted online through the Zoom online meeting platform with employees working for various organisations from home. Zoom is a video conferencing software that allows two or more people in different locations to communicate using audio and video imaging in real-time [75].
The 26 participants in the yoga intervention group were asked to attend a minimum of two and a maximum of three 50-minutes classes each week for six weeks (June/July 2020) led by the researcher who is a registered yoga teacher with eight years of experience. Participants could choose from any of the six classes scheduled per week via Zoom – three in the morning at 8 AM (Monday, Wednesday, and Friday) and three in the evening at 6 PM (Tuesday, Thursday, and Saturday). These timings were agreed after surveying eligible participants. Each participant also received a YouTube video link to a video recording and an instruction manual of the program to practice on their own, after the first week, to make up for any missed classes.
Intervention design
The Yoga program was informed by the tradition of Hatha Yoga and consisted of simplified and modified versions of various components such as poses, breathing techniques and relaxation/meditation techniques to suit the needs of the participants assessed using yoga screening questionnaire. The poses, breathing and relaxation components were selected on the basis of current research evidence in stress management and from yoga scriptures.
The inherent spiritual element of yoga was an important part of the intervention design. Taught yoga classes in modern western societies primarily focussed on potential physical and mental health benefits [71]; however, many scholars concur that decontextualization deconstructs the heart and spirit of yoga [76]. Authenticity was an important consideration in the design of the intervention and was in part, delivered through the chanting of Sanskrit prayers of togetherness in the beginning and fullness at the end. It was further enhanced by encouraging participants to find stillness and patience in the poses (asana) by holding them and focussing on the muscles engaged, pace of breath and thoughts arising in the mind. The scriptural origins and current scientific evidence supporting the selection of all program components is available on request.
Class format
The format of each class followed a consistent pattern: setting the mood, chanting (mantra-uchharan), joint movements (pawanmuktasana samuh), seated postures, standing postures, lying (supine) postures, breathing practices (pranayama) and relaxation through a short-guided meditation (dhyana) (see Table 1)
The hatha yoga intervention
The hatha yoga intervention
An instruction manual with a detailed explanation of each component was made available to participants and is available on request. A few minor modifications of the poses were introduced in week four to maintain the interest of the participants. There was a gradual progression from simpler version of poses to the actual poses. Alternate nostril breathing was introduced in the second week after participants learned right and left nostril breathing techniques. There was a progression throughout the program in gradually increasing the duration of each pose and introduction of minor variations.
Nine outcome measures were selected to assess baseline and post-intervention stress and wellbeing: Perceived stress (Perceived Stress Scale-14 items; PSS-14), Mental wellbeing (The Warwick-Edinburgh Mental Wellbeing Scale; WEMWBS), Coping self-efficacy (Coping Self-Efficacy Scale; CSES-26) and its three subscales - Problem focused coping, Stopping unpleasant thoughts & emotions, Getting support from family & friends, DASS (Depression, Anxiety & Stress scale; DASS-21).
All four scales (PSS, WEMWBS, CSES and DASS), have demonstrated a substantial degree of concurrent validity and internal reliability [77–80].
The PSS is a 14-item scale, commonly used as a psychological instrument to measure the perception of stress, with seven positive items and seven negative items. It measures the extent to which a person perceives life situations as stressful. Participants are asked how often they experienced stress in the last month on a five-point Likert scale from 0 ‘never’ to 4 ‘very often’ e.g. “In the last month, how often have you felt that you were unable to control important things in your life?” Higher total scores indicate higher stress with possible scores ranging from 0 to 56 [81].
The WEMWBS is a 14-item scale used as a measure of mental wellbeing, focusing entirely on positive aspects of mental health [82]. It covers the broad picture of wellbeing, including affective-emotional aspects, cognitive, evaluative dimensions and psychological functioning. The questionnaire collects data about the experiences of participants over the previous two weeks on 14 questions each answered on a five-point Likert scale from 1 ‘none of the time’ to 5 ‘All of the time’ Likert scale e.g. “I’ve been feeling optimistic about the future”. Higher total scores indicate higher levels of mental wellbeing with possible scores ranging from 14 to 70.
The CSES is a 26-item scale used as a measure of an individual’s confidence in performing coping behaviours when faced with life challenges. It analyses coping self-efficacy through three subscales: use of problem-focused coping, stopping unpleasant emotions and thoughts and getting support from friends and family. Participants were asked, “when things aren’t going well for you, or when you’re having problems, how confident or certain are you that you can do the following?” The instrument collects data at any given point in time on an 11-point rating scale – 0 to 10 with anchor points on the scale at 0 – ‘cannot do at all’; 5 – ‘moderately certain can do’ and 10 – ‘certainly can do’ e.g. “look for something good in a negative situation” [77].
The DASS-21 is a shorter version of the DASS 42-item scale used as a measure of negative affect in adults (depression, anxiety and stress); seven items measure each factor. The instrument asks questions about physiological arousal, subjective awareness, low positive effect, along with a few other symptoms. It collects data on depression, anxiety and stress during the last week answered, ranging from 0 “Did not apply to me at all” to 4 “Applied to me very much or most of the time” e.g. I couldn’t seem to experience any positive feelings at all [79]. The cut-off points for severity of each of the categories are described in Table 2:
DASS cut-off points
DASS cut-off points
All four scales and their subscales demonstrated acceptable levels of internal consistency in our sample as determined by Cronbach’s alpha levels (α) ranging from 0.70 to 0.97.
Four open ended questions were asked to assess the overall experiences of the participants in taking part in the program such as perceived benefits, challenges, motivation to attend and acceptability of the online yoga program.
Quantitative analysis
Quantitative analysis was performed using the IBM Statistical Package in the Social Sciences version 26. The data were checked for homogeneity of variances using Levene’s test for equality of variances (p > 0.05), for outliers by boxplot, for normal distribution by Shapiro-Wilk’s test of normality (p > 0.05) and for covariances by Box’s M test (p > 0.001). Pre- and post-intervention data were compared using a 2 (Group) x 2 (Time) mixed-model ANOVA for PSS-14, WEMWBS, all three domains of CSES and on all three domains of DASS-21. An independent t-test was performed to check baseline differences in yoga and control groups on the four outcome measures (PSS-14, WEMWBS, CSES and DASS-21). Only the CSES had any missing responses, where means were calculated providing at least 80% of questions were answered, following author guidelines [77,p424]. Significance was assessed at p < 0.05 and false discovery rate (FDR) approach (Q < 0.05) was used to adjust the impact of yoga intervention on all domains, FDR is considered better alternative than traditional Bonferroni method [83].
Qualitative analysis
Responses were analysed inductively using thematic analysis based on an essential/realist epistemology [84]. A list of core themes was developed after reading answers to open-ended questions several times and coding them. One author (VW) appraised all responses and developed a list of codes and broader themes representing recurrent patterns in the data. Next, a senior qualitative researcher (TC), read through the data, reviewed all codes and broader themes. In the final stage, both researchers discussed each theme and subtheme, debating any discrepancies to agree on a final thematic structure. Two overarching themes were identified.
Results
Quantitative analysis
A total of 26 participants were randomised into the yoga and control groups. In the control group nine participants did not complete both the pre- and post-intervention questionnaires and were therefore excluded, leaving 17 participants for analysis. Of the 26 participants in the yoga intervention group, nine dropped out leaving 17 participants for analysis. Thirty-four participants were therefore included in the final analysis (see Fig. 1).
The mean age of the 34 participants was 42.5 years, 91% were women, 38% were teaching staff, 29% were corporate employees, 9% were employed in administrative roles and the remainder worked in other fields (see Table 3). The majority of participants worked full time (M = 37.2 hours, SD = 4.2).
Characteristics of study participants
Characteristics of study participants
All 17 participants in the yoga intervention group attended the minimum number of 12 recommended sessions during the six-week intervention period. The overall average attendance was 16.6 classes (live streamed classes plus home practice from video) over the six-week program; 2.7 classes per week. Ten participants (59%) completed 18 classes, an average of three classes per week and seven participants (41%) completed more than 12 classes, an average of 2.4 classes per week.
An analysis of pre-intervention variable scores revealed no significant differences between the yoga and control groups as assessed by independent t-tests. Non-completers differed from completers on the demographic variable of age (t = 2.04, df = 24, p = 0.05): the mean age of completers was 42.7 years compared with 34.3 years for non-completers. There was no significant difference between completers and non-completers on any of the nine baseline outcome variables.
A significant interaction was obtained for all outcome measures with p < 0.05 except for ‘anxiety’ and ‘stress’ (subscales of DASS). Analysis of mean scores also revealed significant improvements in seven outcome measures. This indicates that there were significant improvements in seven of the nine outcome measures for the yoga group compared to the control group from pre- to post-intervention (see Table 4).
Mean scores, F-ratios, Interaction P-values and Q-values from two-way mixed ANOVA analysis of PSS, WEMWBS, CSES and DASS
Significance values were determined after calculating FDR corrections for each domain [89].
A 2 (Group) x 2 (Time) mixed-model ANOVA revealed that the main effect of time was significant for seven of the nine outcome measures; it was not significant for ‘stopping unpleasant thoughts and emotions’ and ‘seeking help from family and friends’ (subscales of coping self-efficacy scale (CSES) which indicates improvements in outcome measures in both groups over time but more pronounced in the yoga group. The main effect of Group was non-significant for all outcome measures (see Table 5).
Main effect p-values for PSS, WEMWBS, CSES and DASS
In summary, the two-way mixed ANOVA showed that in comparison to the control group, the yoga group reported significant reductions in perceived stress (PSS); depression; a significant improvement in mental wellbeing (WEMWBS); and coping self-efficacy (CSES); (see Figs. 2,3,4,5, 2,3,4,5). An analysis of the individual domains within the CSES showed that the yoga group in comparison to the control group reported significant improvements in problem focussed coping, stopping unpleasant thoughts and emotions and in getting support from family and friends. Although non-significant, the yoga group also demonstrated feeling less stressed and anxious on DASS scale in comparison to the control group (see Table 4).
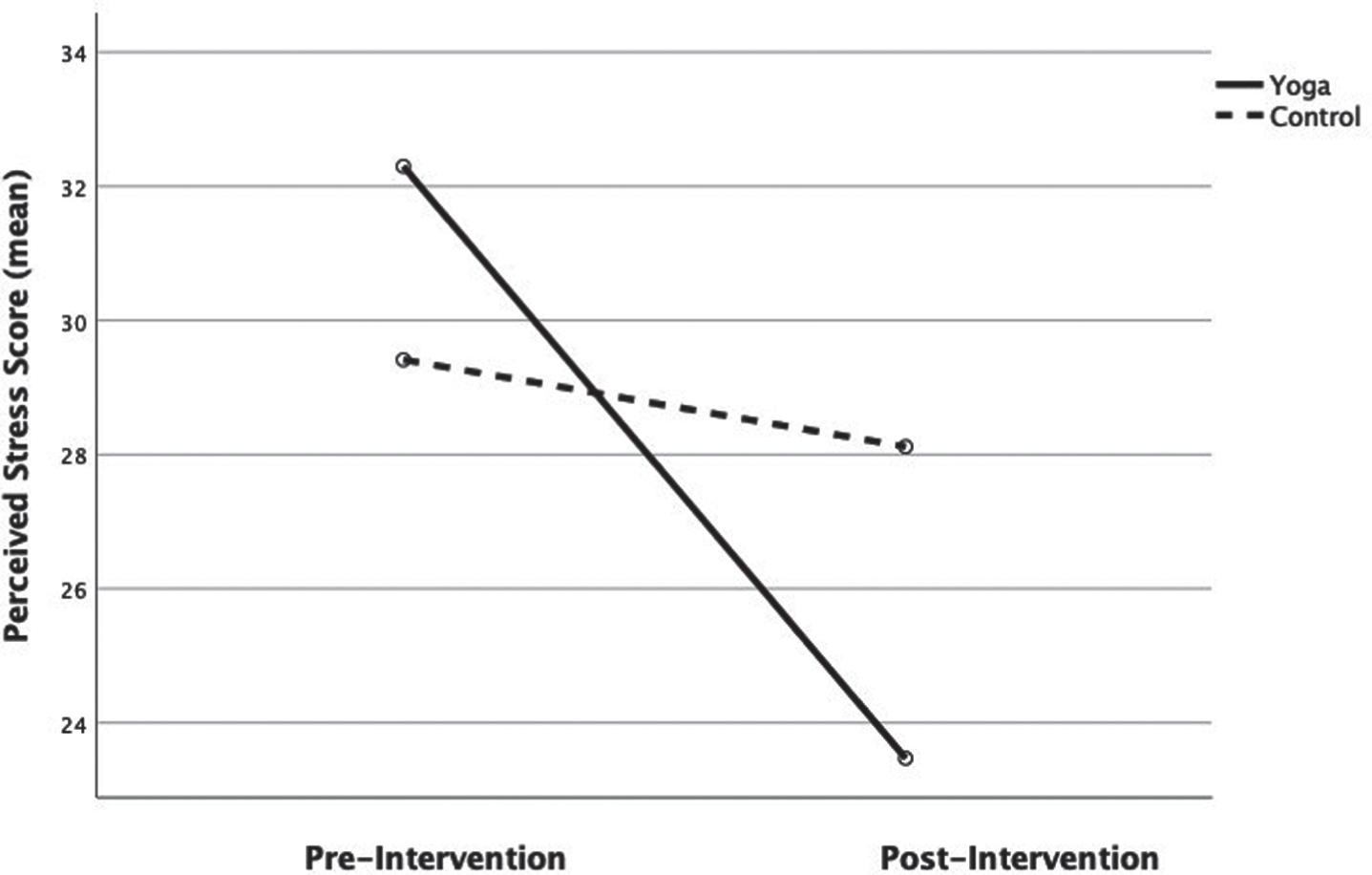
Mean PSS scores. Pre-and post-intervention.
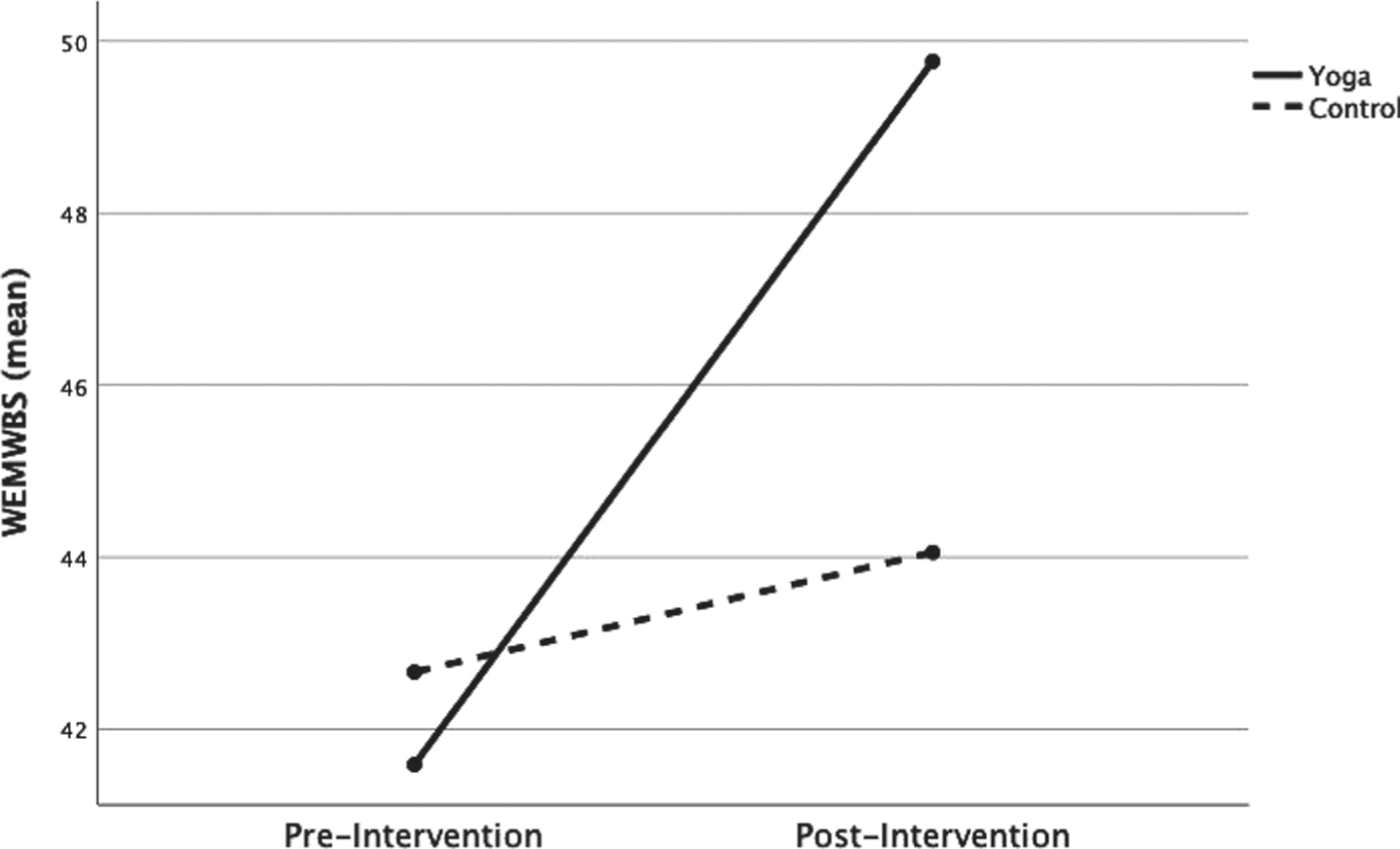
Mean WEMWBS scores. Pre-and post-intervention.
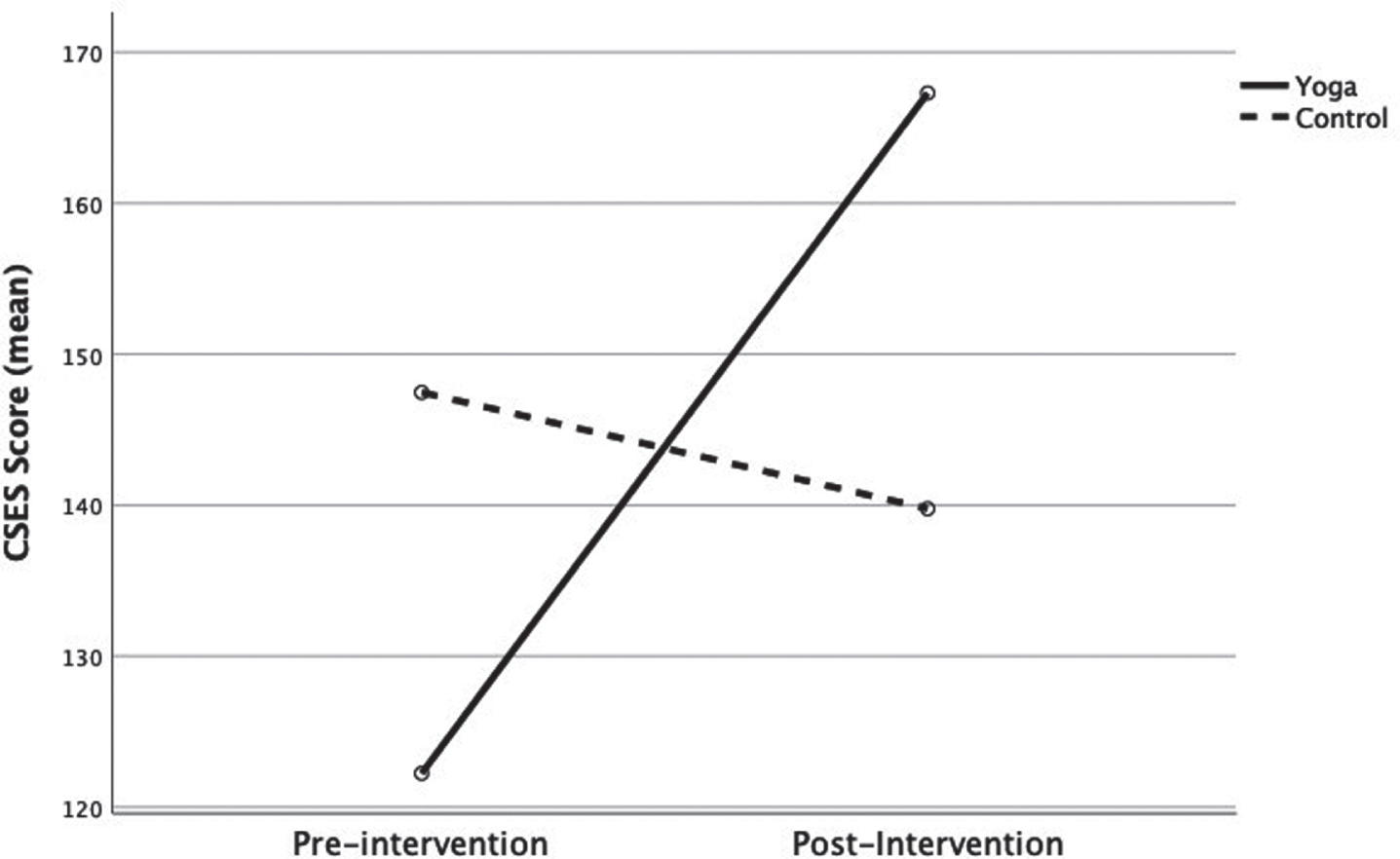
Mean CSES scores. Pre-and post-intervention.
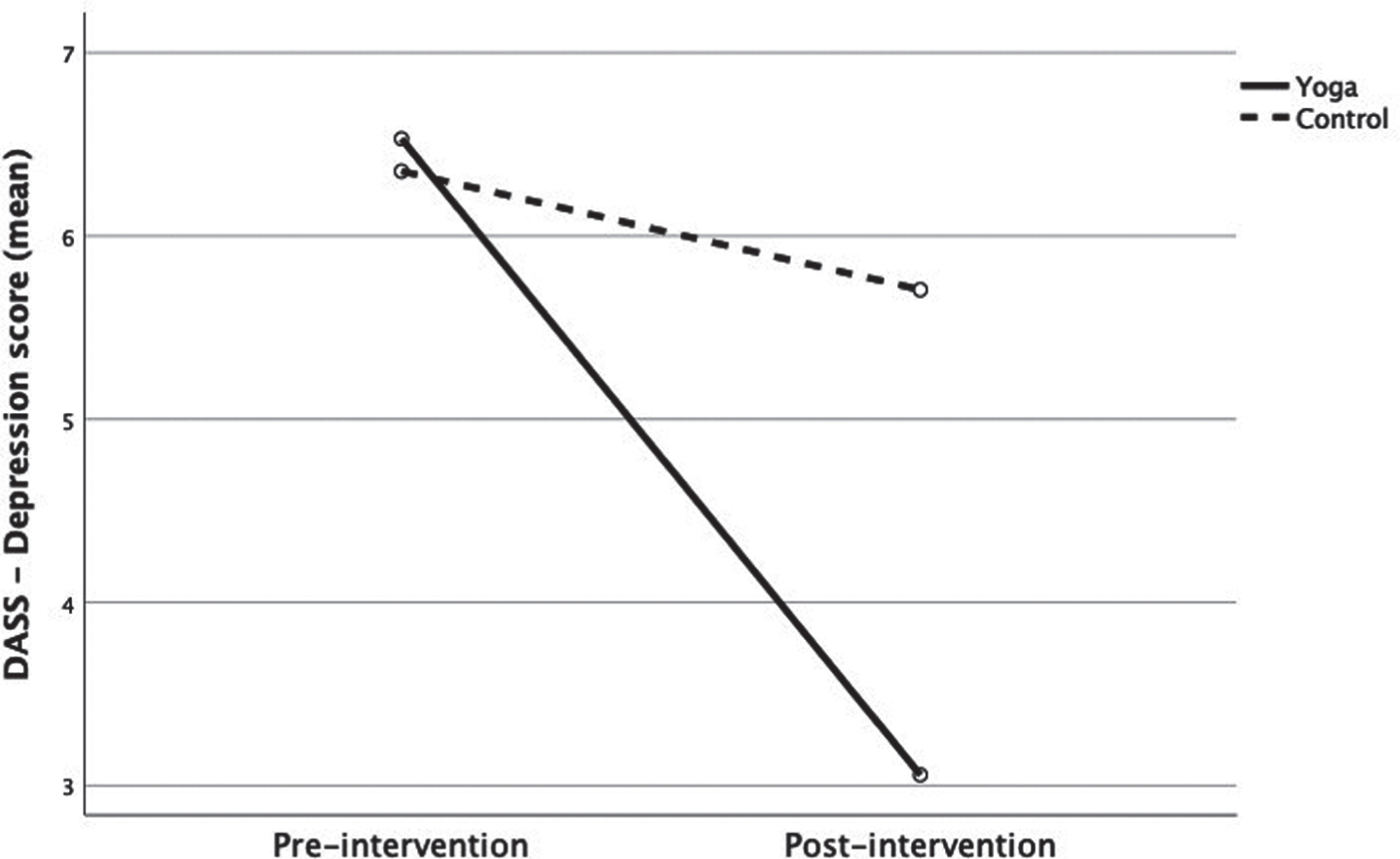
Mean DASS scores. Pre-and post-intervention.
An analysis of DASS cut-off scores revealed that at baseline only 17% of the participants had ‘normal’ levels of depression in the yoga group but this increased to 70% post-intervention. In contrast, in the control group, the percentage of participants with ‘normal’ levels of depression only increased from 29% to 35%. ‘Normal level’ anxiety scores in the yoga group increased from 35% of participants at baseline to 70% post-intervention. However, for the control group, ‘normal level’ anxiety scores declined from 52% to 47% of participants. ‘Normal level’ stress scores in the yoga group improved from 35% of participants at baseline to 64% (+29%) post-intervention. For the control group, ‘normal level’ stress scores also increased, from 23% to 47% (+24%) of participants. Mental wellbeing mean scores increased from 41.59 to 49.76 (+8.17) for yoga participants. In comparison control group participants only showed an increase of 1.48 from 42.76 to 44.24.
Participants were asked several Likert-scale questions to assess the ‘difficulty’ and ‘enjoyability’ of the program, their ‘willingness to continue’ after the study and ‘perceived improvements’ in physical and mental health. Regarding ‘difficulty’ 10 of the 17 participants (59%) found the program not at all difficult whereas 3 participants scored it ‘a little difficult’. Regarding ‘enjoyability’, 94% (n = 16) said that the program was ‘extremely’ or ‘moderately’ enjoyable. Regarding ‘willingness to continue’, 88% (n = 15) said they were ‘extremely’ or ‘moderately’ likely to continue the practice. Regarding perceived improvements in physical and mental health, 76% (n = 13) strongly or somewhat agreed that their physical health had improved; all 17 participants ‘strongly or somewhat agreed’ that their stress level had improved; and 88% (n = 15) ‘strongly or somewhat agreed’ that their overall mental health had improved after the program. Seven participants (41%) ‘strongly’ or somewhat agreed’ that they had changed their lifestyle as a result of this yoga program.
Thematic analysis of participants’ experiences
Participants were asked four open-ended questions to assess their experiences of participation in the yoga program, from which two themes were identified: Perceived impact of the program Experiences of the program
Themes and sample quotes. Perceived impact of the program
Themes and sample quotes. Perceived impact of the program
Themes and sample quotes. Experiences of the program
Several participants commented upon the style and nature of the program. The majority reported an appropriate level of program progression and difficulty. Some reflected on their experience of a gentle form of yoga emphasizing slow and repetitive movements, which helped them experience the poses more deeply. Participants reported a range of challenges, including personal (difficulty in keeping eyes closed), program-specific (slow-repetitive movements being frustrating), technology-related (internet and connection problems) and platform-specific challenges (limitation of not being adjusted in poses or missing a sense of social connection due to online mode of delivery).
To our knowledge, this is the first study that has explored the impact of an online streamed yoga intervention on stress and wellbeing of people working from home during COVID-19. It found that participants in the yoga intervention group reported significant reductions in perceived stress, depression and increases in mental wellbeing, coping self-efficacy and its three subscales: problem focussed coping, stopping unpleasant thoughts and emotions, and seeking help from family and friends, after the intervention. Although non-significant, scores on measures of stress and anxiety also reduced after the yoga intervention. In comparison, the waitlist control group did not show a significant improvement in any of the measures after six weeks. As ascertained by the thematic analysis of participants’ experiences, the convenience of the online mode of delivery and high adherence to the program demonstrated the promising potential, acceptability and feasibility of an online streamed yoga intervention for stress alleviation of people working from home.
These findings are consistent with studies reporting the effects of ftf yoga interventions. In two separate studies, Hartfiel and colleagues found improvements in mood, resilience, psychological wellbeing, perceived stress and back-pain following a ftf yoga workplace intervention [72, 85]. Similarly, a recent systematic review of 13 RCTs found positive mental health and stress reduction benefits of ftf yoga interventions, with nine of them using self-reported measures [42]. Our findings that coping self-efficacy increased after the intervention supported a previous pilot study of an online yoga intervention which improved coping skills and reduced stress in nurse-midwives [66]. Several studies have found an association between increased coping and: better stress management, healthier employees [86], reduction in negative effects of job insecurity [87], high levels of buoyancy, wellbeing and engagement [88] and ‘better’ productivity [89]. These outcomes, along with those of the current study, are particularly salient for wellbeing officers and leaders of organizations in the current context of the volatile pandemic environment.
Several studies have demonstrated that ftf and online mind-body interventions are similar in terms of acceptance, effect and convenience [43, 69], with online interventions rated as superior in some cases [70].Together with the current findings, this supports the potential value of online interventions for organisations who support hybrid working (i.e. on-site and from home). The qualitative findings from this study provide a deeper understanding of participant perceptions of an online program. The majority of participants responded positively to the style and nature of the yoga program by describing experiences of program being of the right style, level and progression. All participants found an online streamed yoga intervention highly convenient, flexible, enjoyable, creating a personal oasis, sense of calm and relaxation with self and body awareness and helpful in stress management as evidenced by both scales (PSS and WEMWBS) and thematic analysis.
These findings are consistent with previous yoga research where participants reported benefits such as mind-body awareness [90, 91], stress reduction [41, 42], and increased mental wellbeing [25]. Participants also noted the benefits of not having to travel and ease of access which is consistent with the findings of Heber and colleagues who found web-based interventions to be cost-effective in terms of travel-related costs for both participants and instructor, high in scalability and easily accessible [63]. Therefore, there is promising potential for an online yoga intervention to offer a cost-effective and convenient tool for workplace managers to improve employee health and productivity, both during the current pandemic [92] and beyond.
The three limitations of an online yoga intervention identified in this research were technology-related (connectivity) problems, lack of social connection (two participants only), and the absence of physical adjustment by the instructor, consistent with previous findings [64]. Our program endeavoured to overcome this latter limitation by incorporating the same series of simple poses to develop self-efficacy in participants; with many reflecting how this enabled them to engage more deeply with the practice. Perceptions of social connection were mixed, with some participants reporting a sense of community, whilst others missed the opportunity to interact, consistent with findings from an international survey exploring the acceptability of online yoga during COVID-19 [93].
Adherence to the program was high, which could be due to a several factors. Participants were sent weekly emails to explain what they would experience and the purpose and philosophy of slow and gentle movements which may have contributed to high attendance and retention. Participants were also given the option to choose from a mix of evening and morning sessions delivered six times each week. However, this has cost implications if replicated in a larger trial. Qualitative findings suggest other potential motivating factors, such as providing a sense of stability to routine, enjoyment, feelings of being supported and held in a safe space, the convenience of using an online platform and experience of tangible benefits. Our findings are consistent with previous research which has found enjoyment, social support, the satisfaction experienced from physical activity, the convenience of access and routine as important factors enhancing adherence and thus increasing the potential for health benefit in women [94–96].
The majority of participants discussed the use of breathing techniques in managing stress outside of the class and found them helpful. This is consistent with previous research where participants reported using breathing techniques to cope with stressful situations beyond the intervention [97, 98]. This ongoing uptake of breathing practices can help maintain the effects of yoga. Breathing techniques were reported as being both enjoyable and having the most notable impact on stress reduction and inducing a calmer state. Indeed, yogic breathing techniques have been found to show promising potential in managing stress [99–102]. Research has demonstrated that yoga breathing can modulate autonomic nervous system (ANS) function, stress responses, cardiac vagal tone, heart rate variability (HRV), central nervous system excitation, vigilance, attention, chemoreflex and baroreflex sensitivity, and neuroendocrine functions [103]. For most adults, slow breathing has been shown to optimally regulate the sympatho-vagal stress response [104–107]. An intervention solely focussed on pranayama (breathing) components of yoga could be beneficial for people with self-image issues who may be hesitant to engage in a postural class. A pranayama-only intervention could be delivered in a relatively shorter duration for stress management and represents an area for further research.
In addition to physiological mechanisms, psychological processes include increased mindfulness, interoceptive awareness, self-compassion, self-control and spiritual well-being [108]. These proposed mechanisms are concordant with our findings where participants described their perceptions of the program impact as increasing self and body awareness, finding a personal oasis, and a sense of calm and relaxation. Some researchers have suggested that yoga practice enhances coping mechanisms that allow practitioners to deal with stress more effectively, thereby reducing stress [109, 110]. This hypothesis is consistent with our finding of a significant increase in coping self-efficacy of yoga group participants in comparison to the control group after six weeks.
In this study, the sample was predominantly female (91%) with no men in the yoga group, similar to Hartfiel et al.’s study (90% female) on yoga for workplace stress and back pain [46]. This reflects national survey data on yoga practice which consistently finds yoga practitioners are predominantly female [24]. However, a contrasting trend was observed in a survey in India, where practitioners were more likely to be men, perhaps due to cultural factors and the Indian origins of the discipline [111]. A similar trend was observed in Puerto Valencia et al.’s systematic review where the female majority studies were conducted in the west whilst male majority studies were conducted in India [42]. Given the potential benefits for health and wellbeing, it is important to identify ways to attract men to participate in mind-body interventions. Further research should be undertaken to better understand the perception of men toward yoga, ways to increase engagement and thereby increase uptake by men in future studies.
As with any study, there are limitations to this research which merit attention. This was a pilot study with small sample size; thus, it can only be considered preliminary work and warrants more extensive study. The sample was recruited through self-selection; therefore, it was representative of employees who were interested in online yoga for workplace stress management. The Hawthorne or placebo effects on the outcomes in the yoga group cannot be ruled out due to the waitlist nature of the control. There was no measurement of stressors affecting individuals during the intervention period – the control group showed a decrease in coping self-efficacy, which could have been due to stressors during pandemic uncertainty. This study only addressed short term impact of an online yoga program; it would be valuable to evaluate whether these changes could be maintained over a longer period of time and should be the focus of future research. ‘Dosage’ is an important factor that needs consideration. Sherman pointed at the non-consensus on optimum dosage for desired outcomes [71]. Further research could explore the optimum dosage for working populations who lack time to commit to longer interventions and/or a high frequency of weekly attendance. A long-term study could assess the continuing acceptability of attendance three times a week. A combination of subjective and objective measures such as heart rate variability (HRV), heart rate, blood pressure, and salivary cortisol should be used in future research to triangulate subjective and objective outcome measures.
Despite these limitations, the hypothesis that a six-week online yoga program will assist people working from home during COVID-19 in managing stress, improving mental wellbeing and enhancing coping self-efficacy was supported, and the findings are promising in terms of providing employers with a low-cost means to support the wellbeing of their employees who work from home. Furthermore, these findings are in no way restricted to people working from home – the intervention could be readily extended to employees working onsite and indeed, other population groups.
Conclusion
This study demonstrated not only the effectiveness but also the acceptability, feasibility and viability of a six week online streamed yoga intervention for stress reduction (of women) when working from home. Participants reported a wide range of benefits to health, wellbeing and stress-management from engaging in a yoga intervention delivered online in the stressful and unprecedented times of COVID-19.
Footnotes
Acknowledgments
The authors would like to express their gratitude to all participants for their time in taking part in the study.
Conflict of interest
None to declare.