
Abstract
BACKGROUND:
Mindfulness interventions aim to foster greater attention and awareness of present moment experiences. Uptake of mindfulness programs in the workplace has grown as organizations look to support employee health, wellbeing, and performance.
OBJECTIVE:
In support of evidence-based decision making in workplace contexts, we created an evidence map summarizing physical and mental health, cognitive, affective, and interpersonal outcomes from systematic reviews of randomized controlled trials (RCTs) of mindfulness interventions.
METHODS:
We searched nine electronic databases to July 2017, dually-screened all reviews, and consulted topic experts to identify systematic reviews on mindfulness interventions. The distribution of evidence is presented as an evidence map in a bubble plot.
RESULTS:
In total, 175 systematic reviews met inclusion criteria. Reviews included a variety of mindfulness-based interventions. The largest review included 109 randomized controlled trials. The majority of these addressed general health, psychological conditions, chronic illness, pain, and substance use. Twenty-six systematic reviews assessed studies conducted in workplace settings and with healthcare professionals, educators, and caregivers. The evidence map shows the prevalence of research by the primary area of focus. An outline of promising applications of mindfulness interventions is included.
CONCLUSIONS:
The evidence map provides an overview of existing mindfulness research. It shows the body of available evidence to inform policy and organizational decision-making supporting employee wellbeing in work contexts.
Introduction
Increased use of the complementary integrative health practice called “mindfulness meditation” is evident in occupational health. Based on ancient Eastern meditation practices, mindfulness is anon-religious practice that facilitates an attentional stance of detached observation. It is characterized by paying attention to the present moment with openness, curiosity, and acceptance [1, 2]. Psychologists and medical providers have turned to mindfulness for therapeutic use and created manualized protocols to treat a myriad of clinical conditions such as stress and chronic pain. Non-clinical populations are using these protocols to support wellness. The most commonly used ones are described in Table 1 [1].
Interventions based on Mindfulness Meditation
Interventions based on Mindfulness Meditation
Organizations are adopting approaches such as mindfulness to improve workplace functioning and support optimal performance of employees [3]. Prominent companies such as Google, Aetna, and General Mills are offering employees mindfulness training to improve their effectiveness [4] and thirteen percent of U.S. workers report engaging in mindfulness-enhancing practices [5]. Empirical research on the effectiveness of mindfulness in the workplace has accelerated [6–8]. Emerging literature in organizational psychology and management suggests that mindfulness is linked to better workplace functioning [9] and recent findings from research on human service professionals suggest that cultivating resilience and mindfulness may assist in preventing psychological distress burnout and secondary traumatic stress [10]. By far the largest base of evidence is found in disciplines such as biomedicine and health, evaluating physical, mental, cognitive, affective, and interpersonal outcomes.
The aim of this evidence mapping study is to present an overview of mindfulness intervention research and summarize the vast body of findings on health and wellness for evidence-based decision-making in workplace contexts.
Methods
Evidence maps are umbrella reviews that are based on a systematic search of a broad research field [11]. Systematic reviews search multiple sources, screen studies against inclusion and exclusion criteria, and summarize results across studies, often aggregating data in meta-analyses. To give a broad indication of the effectiveness of mindfulness interventions, we used the results reported across randomized controlled trials (RCTs) as they provide the most rigorous research design for intervention assessment.
Data sources and searches
We searched AMED (Allied and Complementary Medicine database), Campbell Collaboration database, CDSR (Cochrane Database of Systematic Reviews), CINAHL, DARE (Database of Abstracts of Reviews of Effects), PsycINFO, PubMed, Scopus, and the Web of Science to identify English-language systematic reviews focusing on mindfulness interventions from database inception to July 2017. Additionally, we screened published reviews of reviews and consulted with topic experts. This research builds on a larger project to inform evidence-based decision making at the US Department of Veterans Affairs [12]. The project was supported by an expert panel.
Study selection
To be included in the evidence map, publications had to meet the following four criteria. First, they had to be
Two literature reviewers independently screened the search results. Citations deemed potentially relevant by at least one reviewer were obtained as full text. Full text publications were screened against the inclusion criteria by both independent reviewers; disagreements were resolved through discussion. We documented reasons for exclusion and recorded the literature flow in an electronic database.
Data abstraction and critical appraisal
A content expert and experienced systematic reviewer extracted the review topic, number of included mindfulness RCTs, the comparator, and the results using a pilot tested data extraction form. We documented the format type of mindfulness intervention used, differentiating structured programs such as Mindfulness Based Stress Reduction (MBSR) or Mindfulness Based Cognitive Therapy (MBCT), and other mindfulness-based intervention approaches. We abstracted the author-reported results using the documented metrics such as standardized mean differences (SMD) together with the 95% confidence interval (CI). To address the validity of the systematic review, we extracted whether the review was published by an organization known for their expertise and high quality systematic reviews (e.g., Cochrane reviews).
Data synthesis and analysis
The evidence base was distilled into a broad visual overview using the format of a bubble plot. We used five dimensions to display information: the x-axis; y-axis; and the number, size, and color of the bubbles.
The evidence base was summarized in a narrative synthesis. All included systematic reviews are included in the reference section to provide more information for the interested reader.
Results
The search identified 1,024 citations. Title and abstract screening yielded 320 publications which we obtained as full text. We identified 175 unique systematic reviews meeting the inclusion criteria [13–187].
The distribution of evidence is shown in Fig. 1. The y-axis shows that many research studies have evaluated mindfulness interventions. The largest review, that included research studies evaluating mindfulness interventions and that reported on health outcomes (
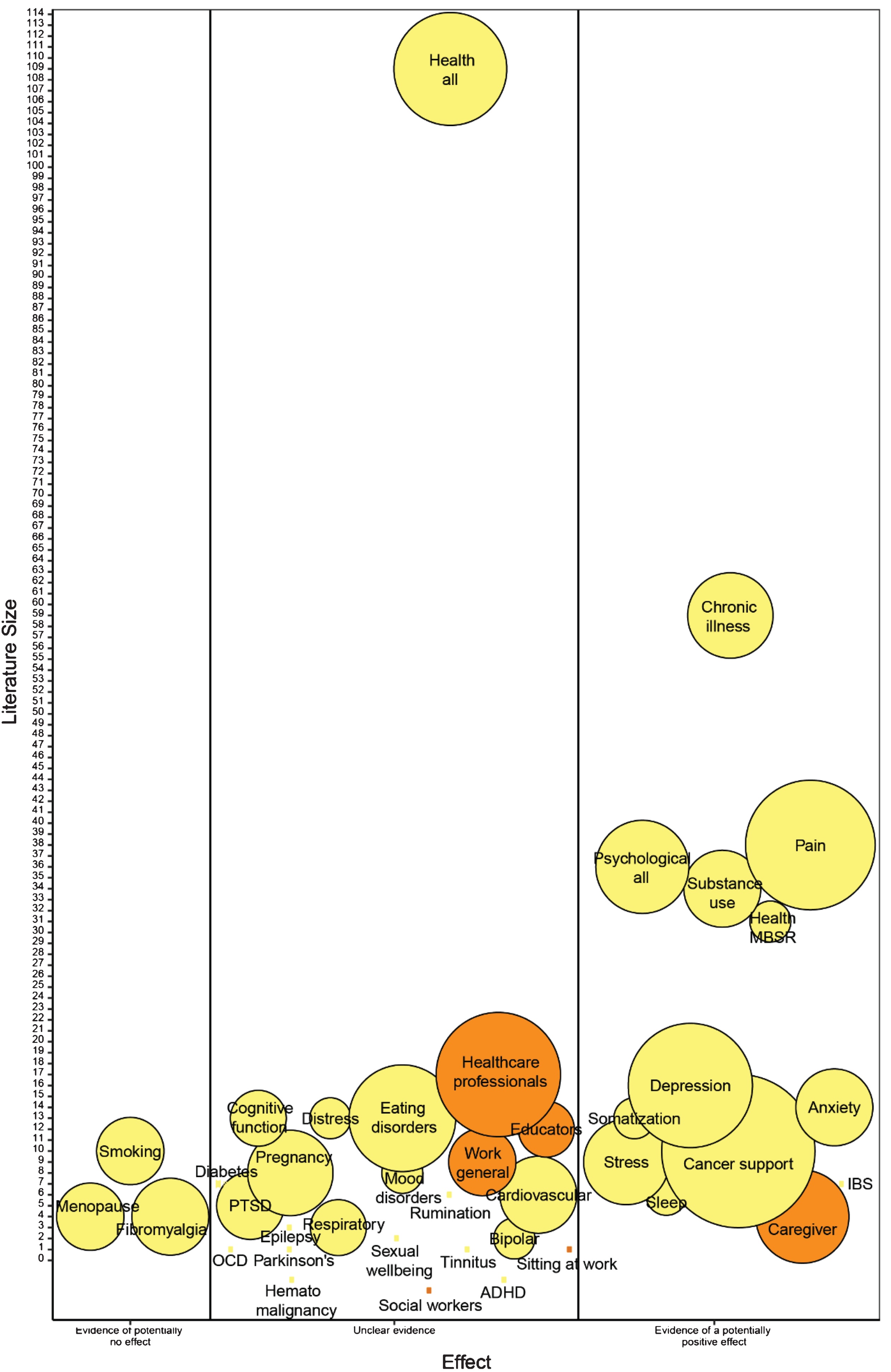
Mindfulness Meditation for Workplace Wellness.
The large number of bubbles demonstrates that mindfulness approaches have been applied in a variety of individual applications, addressing different participant groups, clinical indications, or health outcomes. The evidence map differentiated 39 topic areas to document the available research. The number of systematic reviews per topic area ranged from a single review to 18 identified systematic reviews published on the topic.
The evidence map aims to give a broad indication of the effectiveness of the interventions. The map documents that a large proportion of the existing evidence base is unclear with respect to the effectiveness of the interventions. Reviews either included only a single study without replication of results, reported conflicting results across studies or did not provide summary estimates across studies, while reviews sometimes came to different conclusions.
We identified 28 reviews that addressed the health and wellness of healthcare professionals, social workers, informal caregivers, educators, or general work populations.
Twelve systematic reviews focused on outcomes for
We identified seven reviews of mindfulness interventions for informal or family
Three reviews were found on
Four reviews addressed general
We identified a Cochrane review dedicated to identifying workplace interventions for reducing
Most promising areas in health and wellness
Six systematic reviews addressed mindfulness interventions in
We identified seven systematic reviews that addressed psychological wellbeing (
We identified 12 systematic reviews focusing on
Positive effects were also found across studies and reviews for
Conclusion
The evidence map provides a broad overview of the available research evidence on mindfulness interventions. These findings support and extend the current efforts underway to apply mindfulness interventions in work contexts to enhance employee health, wellness, and performance [3, 191]. Most research is related to general overviews of health benefits. Evidence of potential positive effects is documented for the topic areas chronic illness, pain, substance use, depression, anxiety, perceived stress, somatization, cancer support, and IBS. Mindfulness interventions appear to have general benefits for a range of psychological variables and research shows effects of MBSR on a variety of health outcomes and positive effects on caregivers have been documented. Mindfulness interventions have been applied to a large range of clinical indications but many areas are still based on only a small number of robust research studies.
The evidence summarizing workplace mindfulness interventions focused on groups of professionals and healthcare providers in particular. Systematic reviews of RCTs conducted in work contexts show promise for healthcare providers, nurses, and medical students but require further research for more definitive evidence statements. Positive effects are documented for caregiver burden in caregivers. These findings echo evidence from the organizational science literature [192]. Findings of effects of mindfulness interventions for educators were mixed. Additionally, barriers of feasibility and sustainability of interventions for healthcare professionals may exist, requiring further exploration [193, 194].
The evidence map has several limitations. First, the map only provides a broad overview and is not designed to provide detailed and definitive information on the effectiveness of interventions. Interested stakeholders should review the identified systematic reviews of interest to obtain a more detailed summary. Furthermore, the evidence suggests differential effects of MBSR, MBCT, and other mindfulness-based interventions, and definitions of “mindfulness-based” varied widely in the studies contributing to the research field. Effects of interventions are likely to vary by intervention characteristics and the comparator and the available research is based on a large spectrum of interventions. Interventions included reviews contributing to the evidence map were offered by healthcare professionals in a clinical context and it is unclear how easily the approaches will translate to work context applications (e.g., a mindfulness meditation course for employees to support wellbeing or work performance). Finally, this evidence map was designed to support wellbeing in the workplace and excluded interventions for clinical indications such as psychosis; more information on topics outside the scope of work can be found in an earlier clinically-oriented research report [12].
This evidence map provides a very broad overview of the evidence base indicating areas in which research has been conducted. The results can be used to help workplace setting stakeholders interpret the state of the evidence. The map aims to inform policy and organizational decision making in support of employee wellbeing in work contexts.
Conflict of interest
None of the authors have any conflict of interest to declare.
Footnotes
Acknowledgments
We would like to thank Paul Shekelle, Stephen Ezeji-Okoye, Laura Krejci, Jill Bormann, David Kearney, and John (Greg) Serpa for their expert advice, and Patty Smith for administrative assistance.
The manuscript is based in parts on research funded by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Quality Enhancement Research Initiative. The findings and conclusions in this document are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or the United States government.