
Abstract
BACKGROUND:
Chinese chest pain centers (CPCs) have been expanding and maturing for the past decade, but patient wait times for pre-hospital care remain long.
OBJECTIVE:
To demonstrate that the remote electrocardiogram (ECG) monitoring system can ensure more efficient treatment for patients with ST-elevation myocardial infarction (STEMI) in CPCs, we compared patients with high-risk chest pain who used remote ECG monitoring systems to those who used conventional ECGs in retrospective cohort study.
METHODS:
Based on the inclusion and exclusion criteria, 290 patients who visited our CPC between June 2019 and March 2022 with acute chest pain and a diagnosis of STEMI as well as patients who had undergone an emergency primary percutaneous coronary intervention were selected. Among them, 73 patients with STEMI had employed remote real-time dynamic 12-lead ECG monitoring devices, while 217 patients with STEMI (i.e., the controls) had used conventional ECG monitoring. The effectiveness of treatment procedures for the two groups was investigated. As statistical measures, the symptom onset-to-wire times, first medical contact (FMC)-to-wire times, door-to-wire times, major adverse cardiac events in hospital, and the troponin T levels were analyzed.
RESULTS:
Compared with the control group, the patients with remote real-time dynamic 12-lead ECG monitoring devices showed shorter times for both symptom onset-to-wire (234.8
CONCLUSION:
With remote real-time dynamic 12-lead ECG monitoring equipment, myocardial ischemia can be treated more quickly, leading to fewer possible cardiac events and a better prognosis.
Keywords
Introduction
Chinese chest pain centers (CPCs) have been expanding and maturing for the past decade, and the results have been fruitful: the mortality rate for patients experiencing high-risk chest pain has dropped dramatically [1]. However, patient wait times for pre-hospital care continue to be unacceptable [2]. As reported in the 2020 Summary of China Chest Pain Center Quality Control Report, the average time from the onset of symptoms to the first medical contact (S2FMC) in standard accredited CPCs across China was 312.7 minutes [3, 4]. The key objective of the next stage of CPC development is to reduce the S2FMC time in comparison to the existing 90-minute door-to-wire duration. Work is ongoing to make the CPC more intelligent. To accomplish this goal, CPCs will require the assistance of smarter, more dependable technologies.
The remote real-time dynamic 12-lead electrocardiogram (ECG) monitoring system [5] used in our hospital has been perfected and is user-friendly, making it appropriate for at-home ECG monitoring. The artificial intelligence (AI)-based high-accuracy remote ECG monitoring system is advantageous for the early detection of cardiac traumatic ischemia in patients with acute myocardial infarction (AMI) in CPCs, facilitating referrals of critical patients through the network platform to acquire immediate ECG diagnoses and timely treatment. In addition, this system can notify the CPC team of its results, reducing the period from symptom onset to wire (total time of myocardial ischemia), allowing patients to be treated more efficiently. Similar to tonometers [6] and glucometers, the remote real-time dynamic 12-lead ECG monitoring system enables patients to monitor and record their ECG data at home, performs real-time transmission for the timely detection of suspicious ECG changes [7], and enables AI-based analyses to provide a crucial basis for doctors to diagnose and treat diseases and guide further treatment [8, 9].
By enabling remote and continuous monitoring of cardiovascular diseases, efficient management of health information, and the development of disease risk warning models, wearable ECG monitoring systems help shift healthcare from a reactive “onset-diagnosis-treatment” model to a proactive “prevention first” model, thereby reducing healthcare spending and easing a critical shortage of medical personnel and facilities. On the basis of these criteria, the remote real-time dynamic 12-lead ECG monitoring system is recommended for all patients at high risk for cardiovascular diseases, as it contributes to early detection, early diagnosis and treatment, and improved prognosis. In this study, we compared patients with high-risk chest pain using remote electrocardiogram (ECG) monitoring systems to those using conventional ECGs to demonstrate that the remote ECG monitoring system can facilitate more effective treatment for patients with ST-elevation myocardial infarction (STEMI) in chest pain centers (CPCs).
Materials and methods
Participants
Patients were admitted to our hospital’s CPC in one of three methods, as depicted in the flowchart created for this study (Fig. 1), including direct admission, transport by ambulances, and referral from other hospitals in our network. A total of 1,635 patients with high-risk chest pain were screened with the following five diagnoses: acute STEMI, acute non-STEMI, unstable angina, pulmonary embolism, and aortic dissection. Based on a final diagnosis of STEMI, 290 patients (193 males and 97 females) were enrolled in this study after screening according to the inclusion and exclusion criteria. The demographics of the patients in the two groups were compared in terms of gender, age, diabetes, hypertension, c-TNT, site of lesion, ejection fraction, FMC-to-wire time, and door-to-wire time; the differences were not statistically significant (
Study flowchart.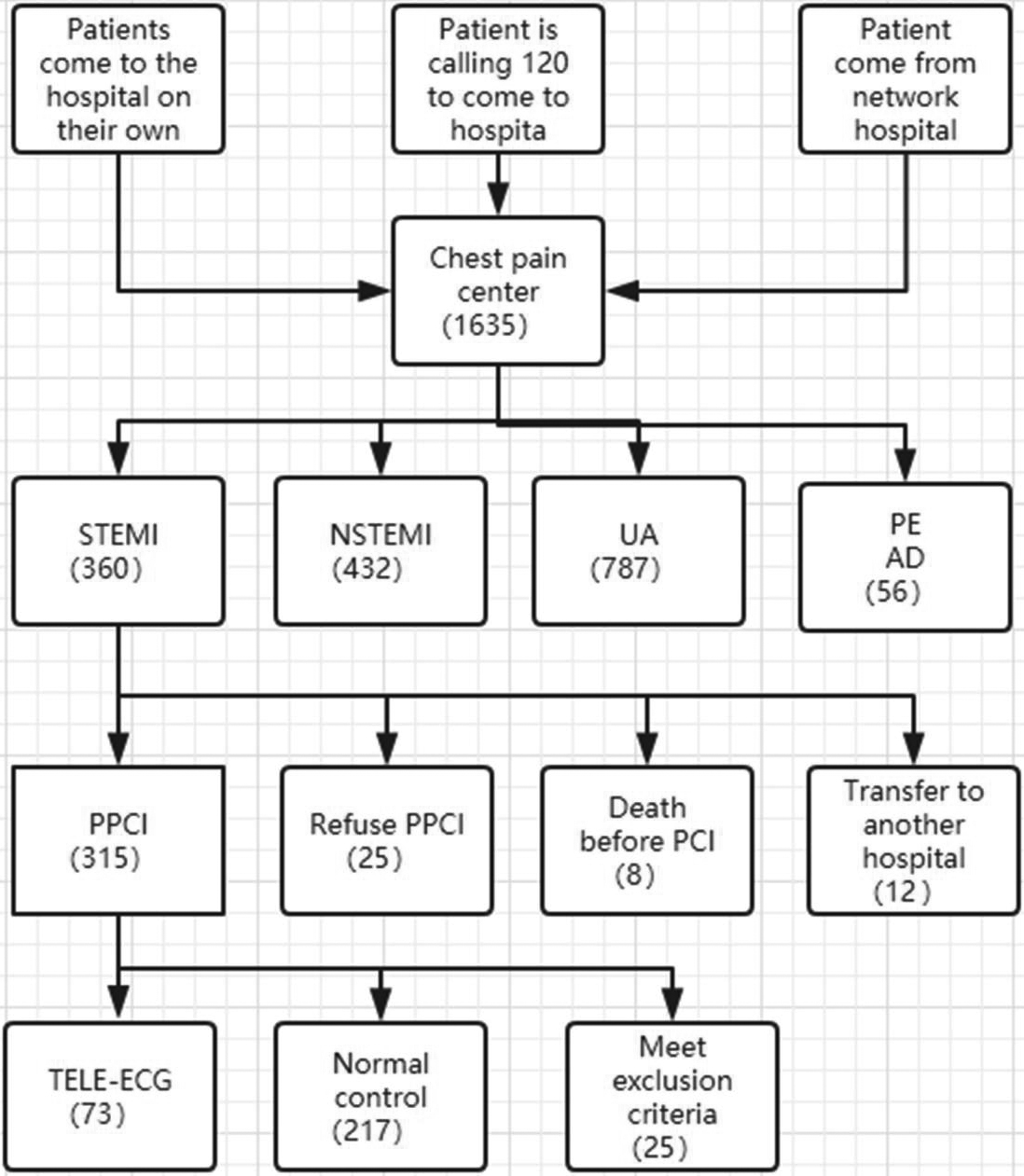
Patients who were admitted to the Shanghai East Hospital between June 1, 2019 and March 10, 2022 for acute chest pain and a diagnosis of STEMI, as well as patients who had undergone emergency percutaneous coronary intervention (PCI), were grouped based on their use of remote ECG monitoring systems.
The inclusion criteria were as follows: (1) patients who had visited the CPC in our hospital due to chest pain through a variety of ways and were diagnosed with STEMI; and (2) patients who had undergone primary PCI (PPCI). The exclusion criteria were as follows: (1) rescue interventional therapy and subsequent revascularization of an acute myocardial infarction (AMI) (after post-percutaneous coronary intervention and coronary artery bypass graft) had been performed; (2) presence of atypical symptoms, such as syncope, abdominal pain and tooth pain; (3) patients suffering from chronic mental disorders; and (4) failure to follow the chest pain procedures.
Process chart of patients with acute chest pain into chest pain center.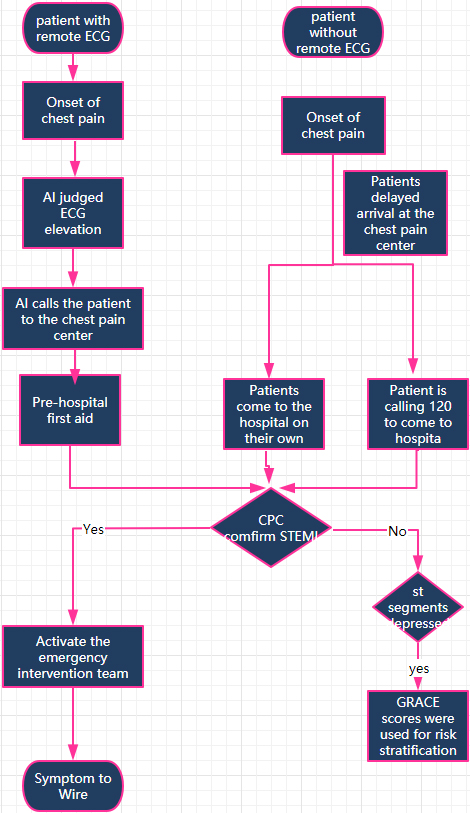
Patients in the experimental group were outfitted with the CONX remote dynamic ECG detection system (BEP186, Xinyun Hengan Medical Technology (Beijing) Co., Ltd., China) (Fig. 3a). The system consists of a collector and a positioning tape. The recorder is connected to four electrodes (Fig. 3b). The recorder has great anti-interference ability, high resolution, and good stability thanks to its 24-bit analog-digital conversion, high integration, and dedicated processing chip for electrocardiogram (ECG) with synchronous sampling in each channel. The positioning belt, which is worn on the patient’s chest, functions similarly to the chest lead of an ECG. In males, the positioning point was set at the median sternum line, and the baseline was at the level of the cleavage line. In female patients, the positioning belt was placed on the lower margin of the breast, and the breast was pulled up so that the electrode point at the positioning line was close to the bottom of the chest (Fig. 3c).
Schematic diagram of CONX remote dynamic ECG detection system.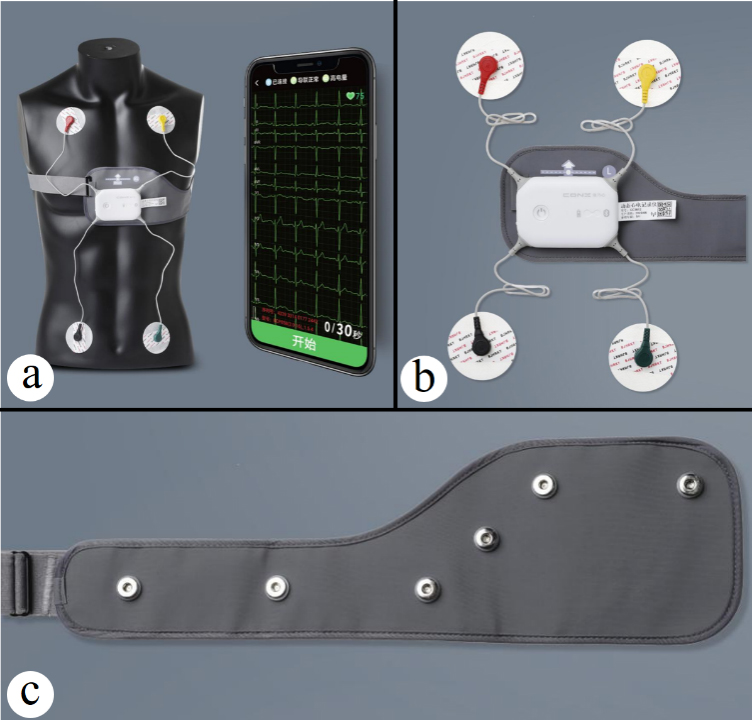
This group underwent the subsequent treatment process: At the onset of significant chest pain, the AI system analyzes the ECG to identify if the patient is experiencing high-risk chest pain. In that case, the patient is notified by the system to visit the CPC immediately. The AI system transmits an early warning and the ECG to the doctors in the CPC treatment group and the on-call physicians simultaneously; specialists subsequently make treatment decisions for the patient based on the ECG. If high-risk chest pain is confirmed, the system calls the 120 emergency medical number to enable communication between the patient and the emergency medical technician, and to assist in transferring the patient to the CPC. The emergency intervention team can speed up the coronary intervention process by arriving at the hospital before the patient arrives thanks to the early alert from the AI system and the doctors on duty in the treatment group. This means less time spent by the patient in a state of myocardial ischemia between system onset to wire [11].
Patients in the control group (non-ECGT) were subjected to the standard care protocols. Procedure in this group: When chest pain develops, often, the patient has difficulty deciding whether to seek medical treatment. By the time treatment is deemed necessary, there is a further delay in deciding the hospital or in calling the 120 emergency number. When the patient arrives at the hospital CPC, the on-duty physician then diagnoses STEMI and calls the emergency intervention team. However, due to the absence of an early warning from the 12-lead ECG monitoring system, the overall time involved is much longer and the time from symptom onset to wire is longer [12].
Outcomes of interventional therapy
All patients who were diagnosed with severe stenosis of the main branches of the coronary arteries (coronary artery stenosis
Database
A database of selected patients was established that included all demographic data, including surgical interventions, laboratory tests, examinations, and clinical events.
Outcome measures
Outcome measures included symptom onset-to-wire times, FMC-to-wire times, door-to-wire times, hospital major adverse cardiac events (MACE), and the maximum troponin T (TNT), wherein, the symptom onset-to-wire times and FMC-to-wire times served as the primary endpoints, and death while in the hospital (30 days) served as the secondary endpoint.
Statistical methods
Statistical analyses were performed using SPSS 26.0 software. The experimental group included patients wearing remote ECG monitoring systems, while patients who did not use remote monitoring systems were included in the control group. Clinical data from both groups were compared. The measurement data are expressed as mean
Basic information and laboratory findings of STEMI patients with Tele-ECG and Control
Basic information and laboratory findings of STEMI patients with Tele-ECG and Control
CPCs often employ two major policies. The duration from when patients’ symptoms first appeared until they reached the FMC is known as the symptom onset-to-FMC time. During this period, patients are assessed by asking them the following questions: Do they need to go to the hospital? How will they get to the hospital? Will they be going to the hospital alone or accompanied by family members? Which hospital should they go to? The time required to conduct such assessments tends to cause delays. The CPC team can save time by having patient information provided in advance when patients use remote ECG monitoring systems, which rely on AI to analyze the ECGs for high-risk ischemia, send the reports to the patients’ cellphones and our CPC duty group, and instruct the patients to come to the hospital.
Myocardial ischemia in a patient with chest pain is measured as the period between the symptom onset-to-wire. When the CPC intervention team is aware ahead of time that a patient with chest pain needs an interventional procedure, the time it takes to activate the catheter room, make a decision and preparations, and notify the appropriate parties is minimized, resulting in a more streamlined process. There is statistical evidence to suggest that the process time is much shorter for patients who receive an early warning. For individuals suffering from STEMI, time is literally life or death. Thus, the prognosis for patients who use remote ECG monitoring equipment is improved [13, 14].
All patients with STEMI were subjected to standard treatment. Dual antiplatelet medications and intensive statins were administered prior to surgery, unless contraindicated, and beta-receptor blockers and angiotensin-converting enzyme inhibitors/angiotensin receptor blockers were administered based on the patients’ circumstances, as shown in Table 2.
The baseline medication selection of STEMI patients after confirmed diagnosis
The baseline medication selection of STEMI patients after confirmed diagnosis
Inadequate awareness and insufficient attention to symptoms in patients with myocardial infarction and the impact of COVID-19 can likely result in delayed diagnoses and treatment [15, 16]. The mean S2FMC time in standard accredited CPCs nationwide in 2020 was 312.7 min. The mean S2FMC time in primary CPCs was 340.6 minutes [17]. Treatment delays are related with an increased risk of ischemia and death for patients with AMI. By aiding in the timely acquisition of pre-hospital ECGs, remote ECG monitoring may greatly raise the myocardial infarction diagnosis rate and lower the PPCI therapy time, both of which can significantly reduce the risk of death in patients with chest pain.
This study included 13,151 patients who had called an ambulance due to chest pain. One-to-one matching was used to compare 2,524 patients who had pre-hospital ECGs with 2,524 patients who did not have pre-hospital ECGs (possibly because emergency medical technicians did not feel it was necessary to perform ECGs because the patients’ chest pain was not persistent, was mild, or had shifted in location), to analyze the correlation between the acquisition of pre-hospital ECGs and the in-patient mortality risk. Previous studies have determined that timely acquisition of pre-hospital ECGs can significantly reduce the risk of death in patients with chest pain [18]. In another study, a total of 4,090 patients with STEMI who had undergone emergency transfer to the hospital were enrolled and divided into two groups (ECGT-FC vs. non-ECGT) based on the presence of ECG transmission equipment in the ambulance. Patients who went to the hospital on their own were included in the control group. The results showed that the ECGT-FC group achieved a significant increase in the STEMI diagnosis rate and a significant decrease in the door-to-balloon time [19].
Recent years have seen the development of wearable, intelligent, and convenient devices for remote dynamic ECG monitoring thanks to the emergence of cutting-edge technologies like the internet, big data, cloud computing, and artificial intelligence. Figure 4 depicts how wearable ECG devices can serve as a crucial carrier and technical means for the new mode of smart medical treatment by providing individualized real-time remote continuous monitoring of ECG data. When used in conjunction with the regional collaborative treatment system, the remote ECG monitoring systems in CPCs significantly shorten the time that patients experience myocardial ischemia.
Typical working principle of wearable ECG device.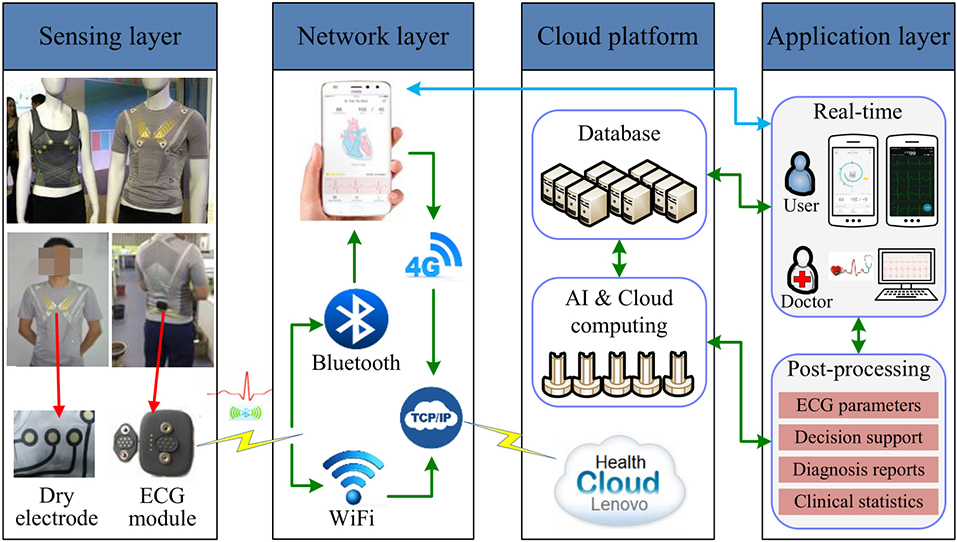
By establishing a three-tiered network with remote ECG monitoring systems, our CPC has drastically decreased the mortality rate of patients with high-risk acute coronary syndrome and STEMI (AMI). It has been shown that this approach can significantly reduce the rate of in-patient serious complications and long-term heart failure, significantly improve patient prognoses, and significantly reduce the overall expenditures incurred by the families of patients and society [20].
Early diagnosis, risk mitigation, surgical care, and disease follow-up are all possible with remote ECG monitoring devices [21]. For this purpose, the patient’s ECG data is transmitted wirelessly across a communication network to a remote ECG diagnosis center, where AI makes a diagnosis and returns the result to the patient and the CPC. The doctors on duty in the CPC can then adopt treatment regimens based on the diagnoses and clinical conditions of the patients.
In our CPC, both pre-hospital transfers and hospital care have been sped up significantly. Successive improvements will aim to speed up patient arrivals. The ECG is interpreted by the AI system, ischemia is promptly identified by the remote ECG monitoring system, and the results are sent to the patient and the CPC. The on-duty physician can thus make timely and accurate diagnoses based on the patients’ symptoms and ECGs. If an ECG suggests STEMI, the system warns the patient and all departments in the CPC and notifies the patient to immediately visit the hospital. Thus, the time from symptom onset to FMC is significantly reduced.
Regardless of time and location, remote ECG systems can provide timely ECG information and real-time analyses thereby ensuring early treatment after onset. The application of remote ECG monitoring systems is beneficial to the improvement of CPC quality control indexes and the timely treatment of patients. The widespread use of this technology can contribute to the early acquisition of initial ECGs after the onset of chest pain, a reduction in treatment time, and an improvement in prognoses. For patients with suspected myocardial infarctions, remote ECG monitoring systems can improve the feasibility of acquiring pre-hospital ECGs and save treatment time. For patients with cardiovascular disorders, wearable home ECG monitoring devices reflect the future trend of remote ECG monitoring development, offering a practical means of self-management that can help alleviate a shortage of medical resources [22]. In the past, a number of studies have reported the clinical application of portable devices for ECG detection, and each study has reported high diagnostic value. Yang et al. researched the clinical diagnostic efficacy, reliability, and accuracy of portable 12-lead ECG Device versus conventional 12-lead ECG device, and proposed that the monitoring results of the portable 12-lead ECG device show good accuracy and reliability, and are similar to the conventional 12-lead ECG device monitoring results [23]. Wang et al. conducted similar research and studied the accuracy of wearable electrocardiogram (ECG) in diagnosis of acute coronary syndrome (ACS) compared with standard 12-lead ECG; they summarized that in qualitative ACS diagnosis, wearable ECG have as high a consistency as standard 12-lead ECG, and have clinical application value [24]. In ACS patients, I, V2, and V4 of the ST-segment have quantitative difference, which, however, have no influence on quantitative diagnosis. Shen et al. reported that application of wearable 12-lead electrocardiogram devices in pre-hospital diagnosis of acute STEMI, and concluded that wearable 12-lead ECG devices can accurately record ECG characteristics of STEMI patients outside the hospital and enable immediate data upload for an early diagnosis [25]. AI-based STEMI diagnoses are largely consistent with those provided by doctors, suggesting that the clinical performance of wearable ECG devices is exceptional.
We selected 290 patients who visited our hospital due to acute chest pain and were diagnosed with STEMI. Statistical measurements included symptom onset-to-wire time, FMC-to-wire time, door-to-wire time, hospital MACE, and maximum TNT. The remote ECG group demonstrated a considerable reduction in symptom onset-to-wire and symptom onset-to-FMC times, as indicated by statistical testing and analysis. The data of the 30-day mortality rate of the two groups suggested that the symptom onset-to-wire time, the symptom onset-to-FMC time, and the maximum c-TNT were independent risk factors for death within 30 days; these time periods must be shortened in the development of the CPC. The maximal value of c-TNT shows the duration and severity of myocardial ischemia; the higher the value, the worse the prognosis for the patient. Therefore, decreasing the duration of cardiac ischemia correlates to a reduction in c-TNT.
With the development of the remote ECG monitoring system, patients can receive ECG monitoring of medical quality prior to admission. Therefore, for patients with high risk of acute coronary syndrome (ACS), a remote ECG monitoring system can be employed to detect acute ischemia episodes in a timely manner, and the ECG data is subsequently communicated to the CPC through the internet. This expedites medical treatment and diagnosis for patients, facilitates faster diagnosis and medical intervention for patients, and eventually meets the goal of improving patient prognosis and reducing the incidence of cardiac events. The results of this study determined that remote ECG monitoring systems can significantly enhance patient prognosis and decrease the 30-day mortality rate by reducing the symptom onset-to-wire time, the symptom onset-to-FMC time, and the c-TNT [26]. Therefore, the application of remote ECG monitoring systems in CPCs needs to be promoted [27].
The limitations of this study included it being primarily a single-center study with a small sample size. In addition, the AI diagnosis of acute myocardial ischemia contained deficiencies. Therefore, it is vital to implement new algorithms to improve the diagnostic precision of AI. The costs of remote ECG monitoring systems should be lowered so that more patients can afford them and benefit from their use. Therefore, remote ECG monitoring technologies may play a greater role in early detection and treatment.
Conclusion and future work
The duration of myocardial ischemia can be reduced with the help of remote real-time dynamic 12-lead ECG monitoring systems, as compared to conventional ECGs. AI in medicine is currently an area of intense exploration, showing potential to even perform tasks beyond human capabilities. Recent AI studies examined cardiac electrophysiology and cardiovascular disease and in the future AI technologies can be performed into clinical practice of PCI. Online AI-based systems can diagnose acute ischemia in real-time based on the ECG, and can immediately alert all relevant CPC departments by phone or online. This results in fewer possible cardiac events and a better prognosis by decreasing the symptom onset-to-wire time. To improve patient prognosis, CPCs should advocate for the deployment of remote real-time dynamic 12-lead ECG monitoring systems. Therefore, we advocate the widespread use of remote real-time dynamic 12-lead ECG monitoring systems in CPCs to improve the 30-day in-patient mortality of patients with high-risk chest pain. With remote real-time dynamic 12-lead ECG monitoring equipment, myocardial ischemia can be treated more quickly, leading to fewer possible cardiac events and a better prognosis.
Funding
The study was supported by the Shanghai Key Clinical Specialty Project (No. shslczdzk06202), the Top-level Clinical Discipline Project of Shanghai Pudong District Grant (Award no. PWYgf 2021-01), the Jiangxi Province Municipal Health Commission Science Technology Grant (No. 202312370), and the Science Foundation of Shanghai Pudong Municipal Health Commission (No. PW2022A-06).
Ethics statement
This study was approved by the Ethics Committee of Shanghai East Hospital (Approval no. 2019072) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The authors would like to acknowledge the hard and dedicated work of all staff that implemented the intervention and evaluation components of the study.
Conflict of interest
The authors declare that they have no competing interests.