
Abstract
BACKGROUND:
Situation, Background, Assessment, and Recommendation (SBAR) is a structured method for communicating critical information that requires immediate attention and action.
OBJECTIVE:
To study the effects of empathy nursing combined with the SBAR communication system on the negative emotions and nursing quality of children undergoing tracheotomy.
METHODS:
This is a clinical observational study. A total of 100 tracheotomy patients who were cared for in the pediatric intensive care unit (subsequent treatment in the tracheotomy clinic or otolaryngology ward) of our hospital from September 2021 to June 2022 were recruited and assigned at a ratio of 1:1 either into a control group (empathic care) or an observation group (empathic care combined with SBAR) using a randomized method. Further, the postoperative anxiety self-rating scale scores, negative emotions, hope index, and nursing quality were compared between the two groups.
RESULTS:
After nursing, the psychological resilience scale score of the observation group was higher than that of the control group, whereas the anxiety self-rating scale score was significantly lower than that of the control group (all
CONCLUSION:
Empathy nursing combined with the SBAR communication system considerably improves postoperative negative emotions and enhances the quality of nursing care for patients undergoing tracheotomy.
Background
Tracheotomy is an emergency procedure to ventilate the patient by incising the anterior wall of the cervical trachea and inserting a tracheal tube, including routine, emergency, and permanent tracheotomies [1]. Tracheotomy is widely used to treat various diseases, but its postoperative complications pose a serious threat to the lives of patients [2]. There are three types of complications after tracheotomy: immediate, early, and late. The most common complications are bleeding, incisional infection, pneumothorax, cannula blockage, decannulation, and ventricular rest [3]. Complications vary in definition, degree, technique, and surgical experience, leading to inconsistent complication rates [4, 5, 6]. Although good post-tracheotomy care substantially prevents complications, the quality of such care lags behind that of other fields of medicine [7].
These symptoms in tracheotomy patients are mostly caused by mechanical injuries, such as intubation before incision, prolonged mechanical ventilation after incision, and air sac compression. Patients not only suffer from airway narrowing symptoms such as dyspnea, but also from pain caused by tracheotomy, which reduces their quality of life. Prolonged poor ventilation and pain stress also increases patients’ psychological burden and affects their psychological comfort. The clinical process of Continuous airway humidification can alleviate patient discomfort, promote sputum expulsion, and prevent infections. However, integrating nursing measures is necessary to boost patient comfort during humidification. Therefore, improving the quality of post-tracheotomy care has garnered extensive interest from researchers.
With the advancement in nursing technology, conventional nursing cannot satisfy clinical requirements. Furthermore, empathic nursing is proposed as a new nursing model, which mainly focuses on the human spirit, in which psychological nursing is combined with affectionate nursing for regulating patients’ emotions, improving sleep quality, and quality of life. The nurse in this model empathically reverberates through real experiences or imagining the patient’s emotions, including emotions, cognition, and feelings [8]. The use of empathic nursing is typified by the fact that nurses can proactively put themselves the patient’s perspective, correctly and rationally perceive the patient’s emotions, and then accurately assess the patient’s emotions, overall physical and psychological condition, among others [9]. Accordingly, nurses should meet the physical and psychological needs of their patients as much as possible [10].
Effective communication, cooperation, and teamwork have been identified as the key determinants of patient safety. Situation, Background, Assessment and Recommendation (SBAR) is a structured method for communicating critical information that requires immediate attention and action. This contributes to effective escalation of management and increased patient safety. In a root-cause analysis of nationally reported cases of infant death and permanent disability in the USA, communication issues among team members was identified as the most important factors. Faulty or delayed communication was considered the primary cause of adverse events in 72% of the cases. The WHO Collaborating Center on Patient Safety Solutions suggested a standardized approach for handover communication between staff, proposing the use of the SBAR technique [11].
Methods
Participants
One hundred patients who underwent tracheotomy and were cared for in the pediatric intensive care unit (subsequent treatment in the tracheotomy clinic or otolaryngology ward) of our hospital between September 2021 and June 2022 were recruited and randomly assigned to the control and observation groups using a randomization calculator (
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) patients aged 2–14 years who underwent tracheotomy; (2) patients with written and verbal skills and clear consciousness; or (3) the patient’s guardian can take the patient’s place of clear expression. The exclusion criteria were as follows: (1) non-tracheotomy; (2) patients who did not provide informed consent; (3) patients with severe mental illness; and (4) patients with congenital, developmental, chronic organ diseases, and severe liver and kidney diseases caused by various other traumas.
Empathic nursing care
Information care: (1) Nurses should explain the patient’s condition, care measures, and treatment plan to the patient and their family so that they can understand the overall situation of the patient’s hospitalization. (2) When the patient shows symptoms such as deterioration and requires resuscitation, the family should be notified immediately, and the treatment and resuscitation plan should be confirmed. (3) The nurse should introduce the environment, facilities, and monitoring equipment of the pediatric intensive care unit (PICU), tracheotomy clinic and otolaryngology ward to the patient and family members and open a 24-hour duty phone to help family members understand the patient’s condition at any time.
Emotional care [14]: Nurses should communicate with patients and families to understand the reasons for their negative emotions. When such emotions arise because of concerns about the patient’s condition, the doctor can discuss the treatment plan with the family and reassure them that the medical staff will do their best. When negative emotions arise because of the cost, they can help to make donations using crowdfunding tools. Most family members have difficulty accepting the patient’s condition. Medical and nursing staff should use professional knowledge, kind words, and gestures to make the patient and family members trust, rely on, cooperate with, and support the medical and nursing staff in their care. The nurse should relieve the psychological pressure of the family in a timely manner, show understanding and sympathy for the family, answer their questions, use transfer and other ways to provide psychological support, and improve the family’s support for the patient. The above nursing measures should be communicated and exchanged with the family if the patient has impaired consciousness or does not understand it. The creation of a comfortable environment: serious and solemn atmosphere as well as noisy environment can further increase the strangeness of the child, and inculcate a sense of fear and resistance, further inducing a series of physiological discomfort. The nursing staff should carefully arrange the child’s treatment environment, so that it is more warm and comfortable, without security risks, and is quiet. Additionally, nurses can post many interesting and cute pictures in the ward, which can be cartoon characters familiar to the children, or a rich expression pattern, or the children’s favorite toys, provide interesting and vivid comic books, or play video animation to the children before the surgery to relieve the negative emotions of tension and fear. Furthermore, nurses can adjust the ward and the operating room to reach the human comfort level, with the humidity controlled at 50%–60%, temperature controlled at 22–26
SBAR communication system care model
Establish SBAR communication channels: (1) Nurses should strengthen nursing management training for nurses with different qualifications and education in the department and change the nurses’ concept of risk management for tracheotomy. In this study, after the nurse communicated with the patient to establish a public WeChat (it means that this wechat number shared by the nurse on duty) number, all the patients’ family members were added to the WeChat account, and the WeChat account was changed to the patient’s name. The nurse marked the basic information of the patient and posted emergency procedures and plans on the WeChat so that the patient’s family had a basic understanding of the emergency diagnosis process and the results achieved. (2) Through the PICU WeChat, telephone follow-up, internet nursing consultation clinic, offline tracheotomy nursing clinic and et al., nurses should update knowledge and information regularly, nursing backbones in the department should be organized to disseminate knowledge to families personally on a regular basis and answer questions for patients and families in the process. (3) Nurses should regularly send the emergency and related information of the department and report their daily work to the WeChat account, so that nurses in the department can fully understand the information related to patients’ diseases. Nurses should help patients establish correct awareness of tracheotomy, change their lifestyle, eliminate negative emotions such as anxiety and tension caused by the disease, motivate patients to face the disease, and actively cooperate with treatment with a positive attitude. (4) Nurse-nurse communication: Nurses should discuss and solve unexpected events together through relevant cooperation and communication between nurses, such as sudden loss of consciousness in children, in addition to promptly informing the doctor; they should also promptly communicate with superior nurses in the same department to determine disposal measures.
Observed indicators
All patients’ follow-up was conducted for 1 month without shedding and withdrawal and assessed using the anxiety self-rating scale score, psychological resilience scale, negative emotion, hope index, and quality of care before and 1 month after nursing care. (1) The anxiety self-assessment scale (SAS) assesses anxiety changes in both groups, which contains 20 items with scores from 0 to 100, and the lower the score, the less anxious the patient. (2) The Connor-Davidson Resilience Scale (CD-RISC-10) [14] is a 10-item unidimensional scale that was used for the participants to self-rate their resilience. This scale was used in previous studies to assess physical activity and resilience. It measures the ability to recover from obstacles. Example questions included “I am able to handle unpleasant or painful feelings like sadness, fear, and anger,” and “I tend to bounce back after illness, injury or other hardships.” Participants were asked to rate the degree to which the statements felt true to them and respond to each question using a 5-point Likert scale ranging from not true at all (0) to true nearly all the time (4). Based on the implementation instructions, scores were summed, with higher scores indicating greater resilience and lower scores indicating lower resilience. The scores range from 40 (most resilient) to 0 (least resilient). Cronbach’s alpha was 0.84, 0.90, and 0.86 at pre-test, post-test, and follow-up, respectively. (3) The Depression Self-Rating Scale for Children (DSRSC) [15]. The DSRSC was developed by Professor Zhou of East China Normal University and consists of 8 subscales and 1 validity scale with 100 items. The eight subscales were learning anxiety, anxiety about others, impulsivity, phobia, physical symptoms, allergy, self-blame, and loneliness. A score of 1 was assigned to each item for “yes” and 0 for “no.” If the validity score was
Quality control
The field survey team comprised trained professional and technical personnel, with one investigator in each classroom for on-site guidance and quality control. To improve the completeness and accuracy of the questionnaire, the students were asked to correct any missing items or logical errors found at the survey site.
Sample Size Calculation
PASS V.11 software (NCSS, Kaysville, UT, USA) was used to calculate that, based on 80% power to detect a significant difference (
Statistical methods
Analyses were performed using IBM SPSS statistics 24.0 and Stata 16. Numerical variables are described as means, medians, standard deviations, and ranges. Categorical variables are described as frequencies, and between-group differences were compared using chi-square tests. Normality of the continuous variables was checked using the Kolmogorov-Smirnov test. Between-group comparisons of normally distributed variables were performed using
Results
Baseline data comparison
There were no statistically significant differences between the two groups in the comparison of general data such as gender, mean age, PaO
Comparison of general information between two groups of patients [
, (
)]
Comparison of general information between two groups of patients [
Before nursing, there were no significant differences in the scores on the anxiety and psychological resilience scales between the two groups (
Correlation score comparison.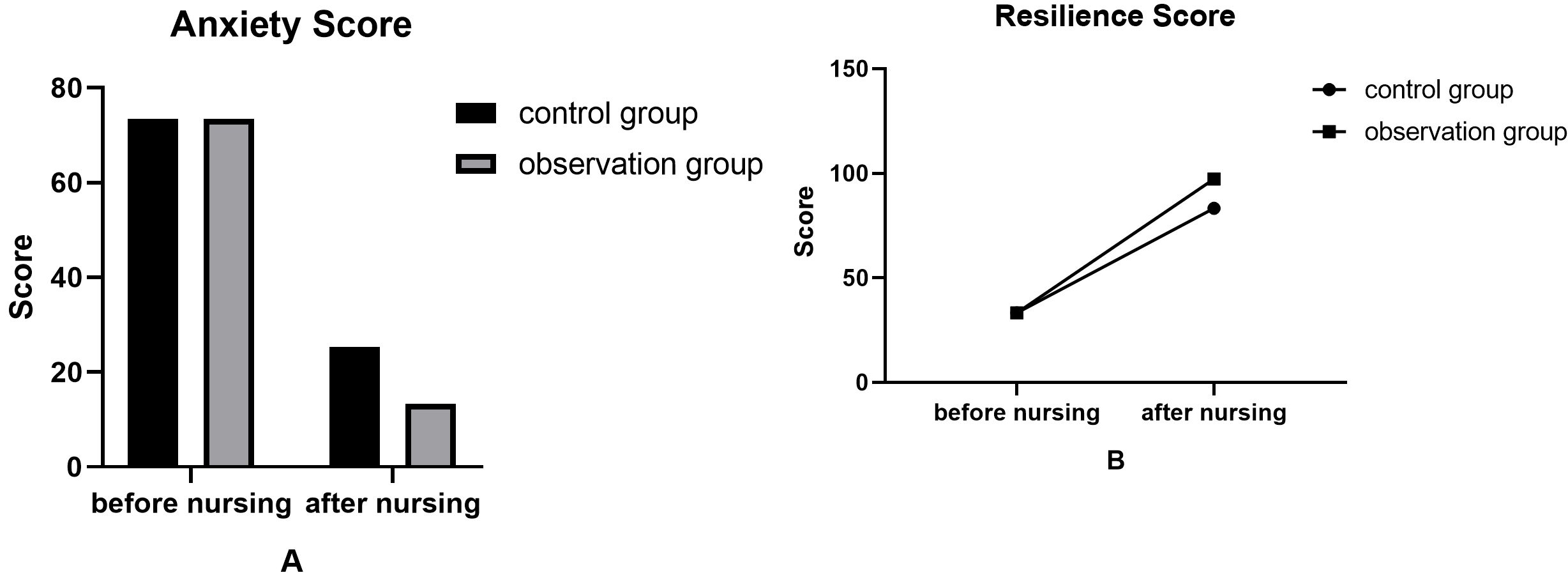
Comparison of negative sentiment and hope index.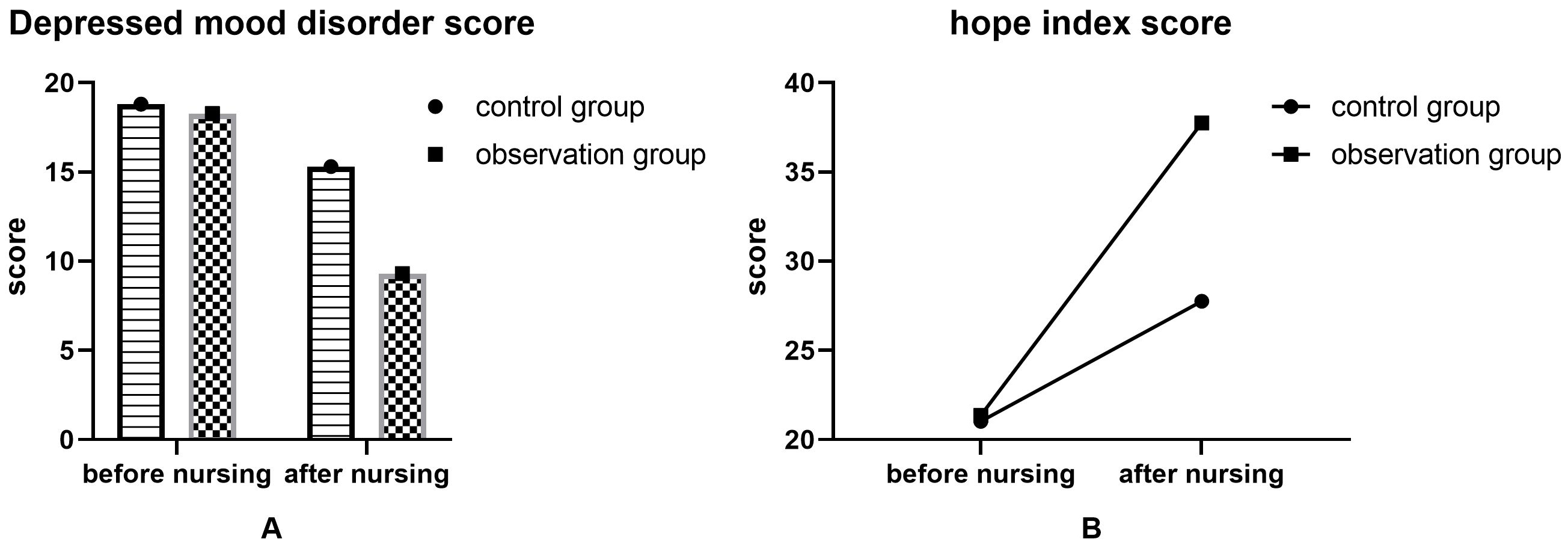
Analysis of quality of care.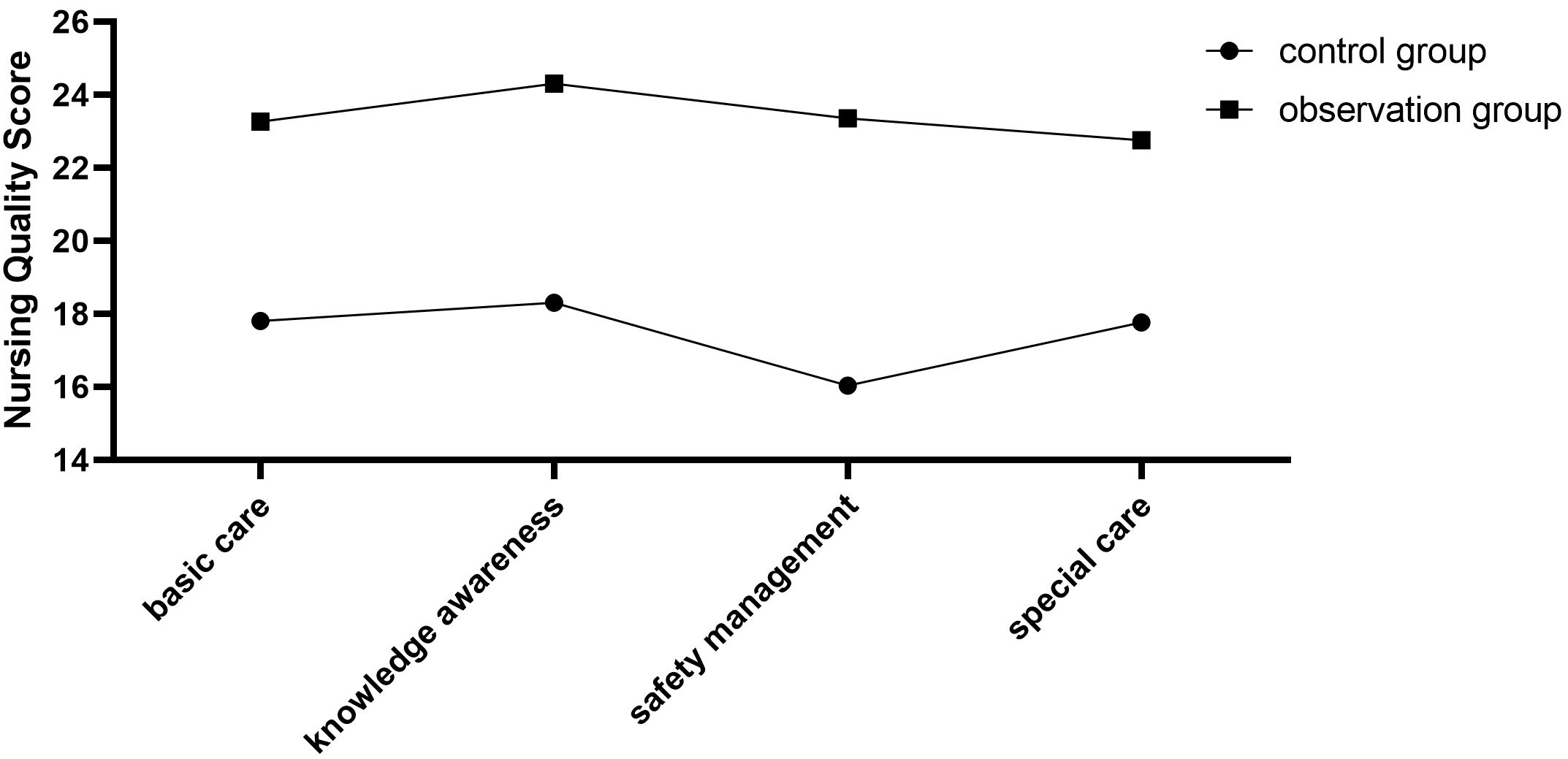
Before nursing, there were no significant differences in depression, mood disorder, and hope index scores between the two groups (
Nursing quality analysis
The basic and special nursing, knowledge awareness, and safety management of the two groups of patients were significantly improved, and the score of the observation group was significantly higher than the control group, and the difference was statistically significant (
Discussion
As healthcare costs and patient demand for care continue to rise, the health system environment must evolve to address new challenges [17]. With the transformation of the healthcare model, the nursing model has gradually changed to person-centered and patient-centered care models, and a new nursing concept of empathic care has been proposed [18]. The concept of empathic nursing is truly embodied by the emphasis on systematic and comprehensive psychological and social care in the nursing process to reduce anxiety, improve negative postoperative emotions, and improve the physical and mental quality of care for patients. Empathic nursing means that nurses can consider a patient’s thoughts and problems from the patient’s perspective [19]. Based on this, a SBAR communication system nursing service was developed [20]. Taking harmonious relationships as a starting point, nurses fully understand the patient, gain the trust of the patient and their family members, and care for patients according to their interests, hobbies, and personality characteristics. Communication among nurses, patients, and parents can be accurately felt and expressed to achieve effective interaction, so that the patient’s family can fully appreciate the nurse’s dedication and pave the way for the development of future treatments and care.
Our study explored the application of empathic care combined with the SBAR communication system care for patients undergoing tracheotomy, and the results showed a promising prospect of empathic care combined with the SBAR communication system that helps reduce the anxiety of tracheotomy patients and improve the negative emotions of postoperative patients. Basic and special care, knowledge awareness, and safety management of patients in both groups significantly improved, and the observation group scored significantly higher than the control group, suggesting that the quality of empathic care combined with the SBAR communication system was better. Furthermore, empathic nursing combined with SBAR communication systems advocates understanding each other’s emotions through verbal or nonverbal expressions; that is, focusing on nurses’ understanding of patients’ thoughts, predicting and correcting their behavior by understanding their intentions and thoughts, and paying attention to patients’ true emotional states is the basis of empathic nursing [11, 15]. Related studies have shown that empathic nursing helps relieve patients’ psychological stress and unhealthy emotions, improves nurse-patient relationships, and enhances the quality of care [3, 8, 9].
Pediatric patients are still young and immature in psychological and physical development, and their pain tolerance and endurance are far lower than those of adults; therefore, they need affectionate, high-quality, and attentive nursing care. Empathic care combined with the SBAR communication system provides emotional support to children, implements effective psychological interventions, and pays careful attention to behavioral and emotional changes in children to minimize the incidence of serious resistance to treatment. Empathic care combined with the SBAR communication system reduces or eliminates the child’s surgical fears and controls negative emotions, which in turn ensures a smooth operation. Empathic nursing refers to the nurses’ ability to think about what a patient thinks, consider the patient’s situation from the patient’s perspective, and develop an affectionate nursing service based on this. The implementation of affectionate nursing care should start with the establishment of nurse-patient relationships, taking harmonious relationships as the starting point. Nursing staff should fully understand patients, try to gain the trust of patients and their families, provide humanized psychological interventions to different patients according to their interests, hobbies, and personality characteristics, and narrate successful treatment cases to reduce psychological fear and enhance confidence in the surgical treatment [17].
At present, there are many studies on compassionate nursing, but few have observed children, especially those who underwent tracheotomy and are in the ICU. This study not only effectively alleviates the common anxiety and irritability of parents of high-risk children through empathic nursing, but also guides parents to establish a positive and optimistic attitude that plays a positive role in children’s behavioral development and intellectual growth [21]. Establishing a relationship between trust and dependence between the two sides provides convenience for follow-up, timely solving of problems in the care process of high-risk children, and improvement of the quality of life of high-risk children. The SBAR model was also incorporated to provide more comprehensive care for children to ensure quality of recovery [22].
Our study has some limitations. First, the selected samples were all from patients treated or cared for in our hospital; therefore, the selection of patients was subjective to the inclusion and exclusion criteria, and the study results may not be representative. Second, the trial design of our study did not include a blank control group but only two groups of empathic care and empathic care combined with the SBAR communication system care model, which may easily lead to biased results. Finally, the recovery of patients who underwent tracheotomy in the PICU, tracheotomy clinic and otolaryngology ward has not been studied in depth and has not been observed for a long time. In addition, the observation period was insufficient. In future studies, the case source and sample size can be further expanded, more meaningful relevant indicators, such as safety indicators, can be designed, and the observation period can be extended to secure more reliable data to validate the findings of the present study.
Conclusion
Empathic care combined with the SBAR communication system can effectively reduce tracheotomy-related anxiety, improve negative postoperative emotions, improve the quality of care, and provide a reference for clinical tracheotomy care.
Competing interests
The authors declare that they have no competing interests.
Funding
No external funding was received to conduct this study.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The authors would like to acknowledge the hard and dedicated work of all staff that implemented the intervention and evaluation components of the study.