
Abstract
BACKGROUND:
After stroke, gait training is a key component of rehabilitation, and most individuals use a variety of walking aids depending on their physical condition and environment.
OBJECTIVE:
This study aimed to investigate the potential effect of a one-arm motorized gait device for gait assist of chronic hemiplegic stroke survivors through comparison with traditional gait devices (parallel bar and hemi-walker).
METHODS:
This study was conducted on 14 chronic hemiplegic stroke survivors. The participants were asked to walk under three conditions using different gait devices, and their gait parameters during walking were collected and analyzed. The first condition involved walking on parallel bars; second condition, walking using hemi-walkers; and third condition, walking using one-arm motorized gait devices. With the use of a gait analysis system, the spatio-temporal gait parameters in each condition were collected, such as gait velocity, cadence, step length, stride length, single support time, and double support time.
RESULTS:
In the results by repeated-measures ANOVA or the Friedman test, a significant difference was found in the gait parameters among all three conditions (
CONCLUSION:
The results of this study suggest that one-arm motorized gait devices developed for hemiplegic stroke survivors may be more effective potentially than parallel bars and hemi-walkers in gait assistance of chronic hemiplegic stroke survivors.
Keywords
Introduction
Stroke is a major cause of permanent disability and death [1], and many survivors with stroke experience limitations in performing activities of daily living along with hemiplegia [2]. It has also been reported that balance and gait abilities decrease in 88% of survivors with stroke [3]. Gait ability, in particular, is highly relevant to independent daily living, and its improvement is one of the important goals of rehabilitation for stroke survivors [4].
Gait devices have long been used in individuals with various dysfunctions, such as stroke, to help them achieve independent gait [5]. In clinical settings, the most commonly used gait devices might be parallel bars, canes, crutches, and hemi-walkers. These devices not only serve as structures that enhance stability and balance and increase muscle activities but can also be used together as gait training devices [6]. The main role of gait devices in gait training is to support the stroke survivor’s stability and balance. Stroke survivors with movement difficulties will have improved stability and balance from the use of gait devices, which is also helpful for inducing purposeful physical movement, such as walking [5, 7]. Walking is a very important factor in determining the range of activities of daily living performed; this indicates that it plays a crucial role in evaluating the survivor’s quality of life. Thus, the appropriate use of gait devices affects many aspects from stability, balance, and gait to independent daily living [5, 7].
Gait training is a key component of rehabilitation for many individuals with gait abnormalities. Most stroke patients use a variety of gait assistive devices depending on their physical condition and environment. In particular, they perform gait training with assistive devices in the following order according to the degree of recovery: parallel bars, hemi-walkers, and canes [7]. Parallel bars are the safest devices that can provide the most stability and balance during gait training. They are gait devices used in most survivors at the beginning of rehabilitation [7]. Survivors with hemiplegic stroke often use hemi-walkers or canes. Hemi-walkers and canes have the advantages of being light in weight and convenient to use while on the move. In addition, they allow walking with partial weight support by pressing the gait device with one hand [5]. However, stroke survivors using walkers and canes must have some level of walking ability. The method of supporting weight by holding a device requires a hand pressing direction from top to bottom at an appropriate angle. If users accidentally lift the handle up or press it in a horizontal direction while holding on to the handle, there is a risk of rollover or fall owing to too little weight support [7]. Moreover, unlike parallel bars, walkers and canes are limited in the angle of pressing the handle to support weight, which makes it difficult for users to obtain the desired amount of weight support [7]. Therefore, the parallel bar can be the best gait training equipment that enables safe weight support for stroke survivors who lack gait ability. However, it is not possible to outdoors gait with equipment, and this is limited in that the movable area is too small, which also limits the continuity of walking [7].
With the development of robotic technology, various robotic devices are being used for gait of stroke patients [8]. The exoskeleton gait rehabilitation robot based on a treadmill controls the joints of the lower extremities electrically, and is known to induce improvement in walking ability through repetitive gait pattern training on the treadmill [9]. In addition, the end-effector gait rehabilitation robot makes the gait pattern through the control of the foot rest, the various degrees of freedom allowed for the lower extremity joints induces active movements control in multiple directions of the lower extremity [10]. However, because these robotic devices are bulky and fixed, overground walking required for community walking is difficult.
Recently, a gait device (one-arm motorized gait device) that supplements the limitations of traditional gait assistive and robotic devices has been developed [11, 12]. One-arm motorized gait device features a round bar-shaped handle similar to a parallel bar with an adjustable height. This round bar allows survivors to practice gait training as in parallel bars. In addition, one-arm motorized gait device is driven by an electric motor on the non-paralyzed side of the user, so there is no driving distance limit, and overground walking is possible [11, 12]. However, in the previous studies, although the one-arm motorized device was that being modeled on the parallel bars capable of full weight support, no comparative studies were conducted with parallel bars. Thus, this study aimed to investigate the recommendable potential of a one-arm motorized gait device for the gait assist of chronic hemiplegic stroke survivors through comparison with traditional gait devices (parallel bar and hemi-walker).
Methods
Participants
This cross-sectional study was conducted in survivors with chronic hemiplegic stroke. Volunteers were recruited through an announcement on the public bulletin board of G Rehabilitation Hospital. A total of 15 volunteers were recruited. The participants were screened using the following criteria: 1) interval to stroke onset of
Characteristics of the participants (
14)
Characteristics of the participants (
The spatiotemporal gait parameters were collected during walking using three different gait devices (A: parallel bars, B: wheelless hemi-walker, C: one-arm motorized gait device).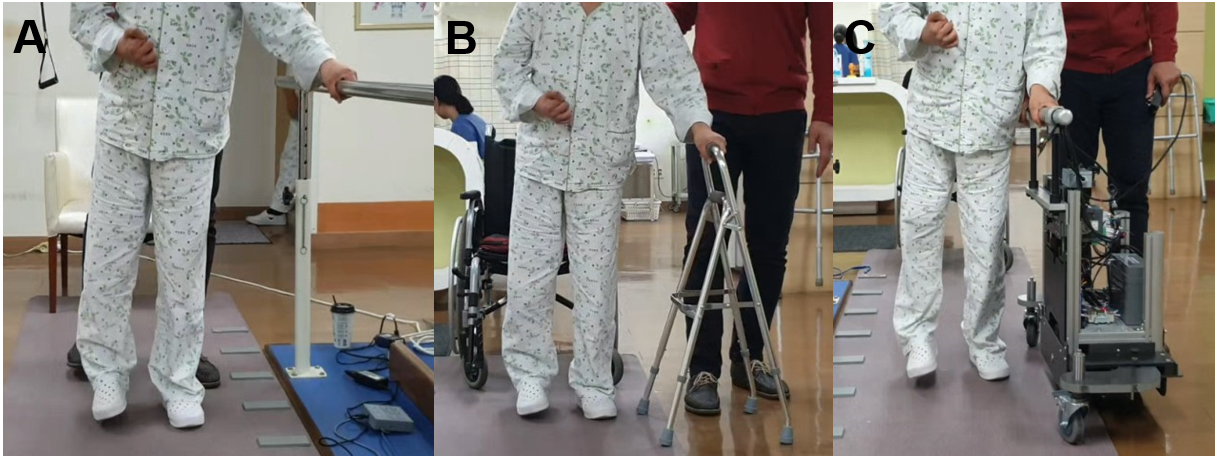
Before starting the experiment, a research assistant collected information on the participants, such as gender, age, height, weight, paralysis side, etiology, disease duration, and functional ambulation categories, through a simple interview or review of medical records. Then, the research assistant demonstrated how to use three different gait devices including parallel bars, hemi-walker, and one-arm motorized gait device, and the participants practiced using the devices enough to be able to use the device. In particular, in the case of a one-arm motorized gait device, the participants practiced until they were able to operate more than 10 meters by themselves. To prevent falls due to inexperienced manipulation, a physical therapist with 10 years of experience conducted a supervision with an emergency remote control during they were walking using the devise. The participants were asked to walk using three different gait devices, and spatio-temporal gait parameters collected during walking. The gait devices were selected in random order, to avoid any potential learning effect or influence of fatigue on results. In the present study, parallel bars (Fig. 1A) that manufactured with height-adjustable bars on both sides, a hemi-walker (Fig. 1B), and a one-arm motorized gait device (Fig. 1C) [11, 12] were used as gait assistive device. The participants were instructed to walk on a gait mat (GAITRite Electronic Walkway) at their usual comfortable gait velocity using the three gait devices. Also, they were instructed to walk using a three-point gait pattern, moving the gait assistive devices first, followed by the affected leg and the nonaffected side leg. Spatio-temporal gait parameters were automatically recorded while participants walked on the gait mat. Walking using each gait assistive devices was measured three times, and the average value was used for statistical analysis. All participants had a 10-min break between each trial. In addition, when switching from one device to another, a break time of 30 minutes or more was provided.
Outcome measures
Gait analysis was performed using a gait mat (GAITRite Electronic Walkway; CIR Systems, Inc., NY, USA). The GAITRite has a length of 4.8 m and width of 0.9 m. It is an electronic walkway that contains sensors arranged in a pattern to measure the pressure exerted by the feet on the contact surface. The equipment acquires data, which are transmitted via connections to a laptop; an application software within the computer processes patterns from the soles of the feet. In the present study, parameters, such as gait velocity, cadence, step length, stride length, single support time, and double support time, were collected [13].
Data analyses
Statistical analyses were performed using SPSS 18.0 (IBM Corporation, NY, USA). The general characteristics of the participants were analyzed using descriptive statistics. All data were tested for normality using the Kolmogorov-Smirnov method. Repeated-measures ANOVA or the Friedman test was performed to compare the gait parameters among the conditions. The Bonferroni method or Wilcoxon signed-rank test was used for post-hoc analysis. The significance level (
Results
The results of the comparison of the spatio-temporal gait parameters when walking using parallel bars, hemi-walkers, and one-arm motorized gait devices are shown in Table 2. In addition, the major changes are shown in Fig. 2. There was a significant difference in all spatio-temporal gait parameters among three conditions (
The change of spatio-temporal gait parameters according to the use of three different gait devices (
14)
The change of spatio-temporal gait parameters according to the use of three different gait devices (
Values are presented as Mean
The major changes of spatio-temporal gait parameters according to the use of three different gait devices (parallel bar, hemi-walker, and one arm motorized walker).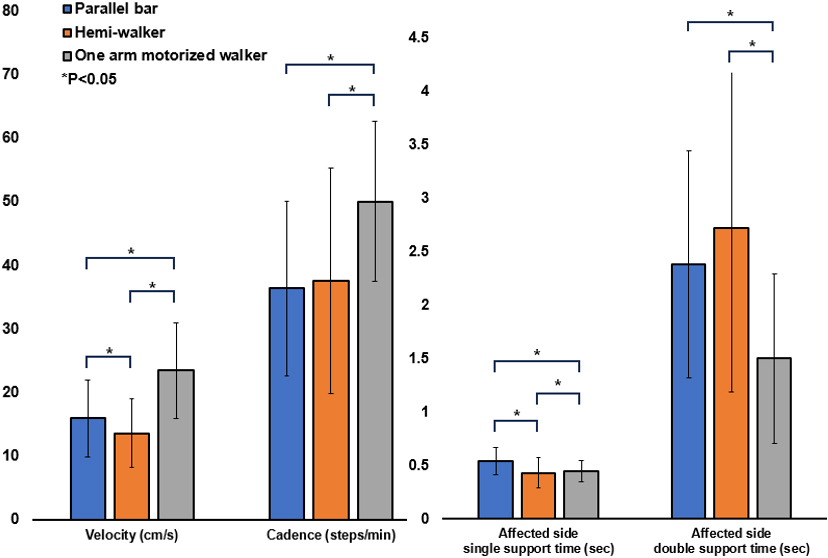
In the post-hoc analysis of the parallel bars and hemi-walkers, there were significant changes in the gait velocity, stride length, and single support time of the affected side and in the step length and stride length of the non-affected side during walking using parallel bar than hemi-walker (
In the post-hoc analysis of the parallel bars and one-arm motorized gait device, there were significant changes in the gait velocity, cadence, single support time, and double support time of the affected side and in the stride length and double support time of the non-affected side during walking using one-arm motorized gait device than parallel bar (
In the post-hoc analysis between the hemi-walkers and one-arm motorized gait device, there were significant changes in the gait velocity, cadence, step length, stride length, single support time, and double support time of the affected side and in the step length, stride length, single support time, and double support time of the non-affected side during walking using one-arm motorized gait device than hemi-walker (
Decreased walking ability are common sequelae in diseases such as stroke. It is very important to develop and utilize devices that can help survivors with these sequelae engage in gait training and perform activities of daily living [5]. The development of new gait device is becoming more important because of the effects gait device have on walking [5]. The one-arm motorized gait device used in this study may be an efficient device that offers both the stability of parallel bars and the mobility of canes [11, 12]. The results indicate that the one-arm motorized gait device may be used as an efficient device for walking training and assistance.
In clinical settings, parallel bars are used in the initial gait training during rehabilitation [5, 7]. The one-arm motorized gait device developed in this study may be used in gait training, replacing the role of parallel bars. Adopting the stability of parallel bars, this device has a low-centered design, in which the battery and the motor are concentrated at the lower part to prevent overturn [11, 12]. In addition, the gait velocity were 23.48 cm/s, 15.96 cm/s, and 13.62 cm/s for the one-arm motorized gait device, parallel bars, and hemi-walker, respectively. These results show that the device offers gait assistance at a faster gait velocity than parallel bars or hemi-walkers during initial rehabilitation. Absolutely, 23.48 cm/s is slower than normal walking speed. However, it is very important for successful rehabilitation to have experience speed as fast as possible to get close to normal walking speed for the stroke survivors [13]. Therefore, the use of one-arm motorized gait devices in the stages of rehabilitation may be helpful for survivors to experience near-normal gait velocity than the use of other gait devices; hence, it may consequently improve gait ability [13]. After the onset of stroke, near-normal gait experience can increase sensory motor feedbacks and feedforwards that promote brain plasticity, increasing recovery of gait ability [14].
And, the present study showed that the step length and stride length significantly increased with the use of the one-arm motorized gait assist device compared with the use of hemi-walkers or parallel bars. Furthermore, single support time and double support time significantly decreased with the use of the one-arm motorized gait assist device. Thus, the one-arm motorized gait assist device used in this study may have had a positive effect on improving spatial gait parameters, stability, and balance ability. In the present study, the temporal gait parameters, i.e., gait velocity and cadence, significantly increased with the use of the one-arm motorized gait assist device compared with the use of the other two gait assist devices. It seems that the increase in the temporal parameters resulted from the difference in the walking method. In general, patients with hemiplegia perform a three-point gait, moving the cane or hemi-walker first, followed by the affected leg and the healthy side leg. In this process, patients have to lift up the assist device to move when using existing canes or hemi-walkers. However, with the one-arm motorized gait assist device, there is no need to shift the hand or lift the gait assist device to move. The process that can interrupt walking or influence balance during walking is omitted, which results in continuous walking. This aspect seemed to have had a positive effect on the temporal parameters, such as gait velocity.
If motor function remains during rehabilitation, it encourages people to move on their own without resorting to gait devices as much as possible [15]. However, the devices used in recent gait rehabilitation are worn by the user as slings or exoskeleton devices to support the user’s weight bearing and to create passive gait with the power of an electric motor [16]. These devices can be effective in restoring balance and gait ability by allowing repeat artificial gait [17]. The application of the technical motor system can increase sensory feedback and stimulate recovery as much as possible by stimulating the potential associated with plasticity [18]. However, according to a systematic review by Swinnen et al. [19], it is not clear whether robot rehabilitation using exoskeleton devices developed and applied recently is effective in recovery of balance and gait abilities after stroke. For stroke survivors, the use of suspension or automated exoskeleton devices is likely to limit their neuroplastic activity due to different retraction information provided in actual walking and environment [17]. Of course, survivors who have difficulty walking can benefit from supporting weight support and the use of automatic walking programs [20, 21]. However, for stroke survivors who can at least maintain a standing posture, floor walking using one-arm motorized gait device for physiological sensation and motor feedback on the paraplegic side can be maximized [20, 21].
Limitations
Through the present study, the one-arm motorized gait device was found to be more effective than the hemi-walker and parallel bars in their walking. However, this study has some limitations. First, it may be difficult to generalize the results as only a small number of participants with chronic stages of the disease were involved in the study. Second, the muscle activation while using the one-arm motorized gait device was not analyzed. Third, although there were significant improvements in the spatio-temporal gait parameters with the one-arm motorized device, some of the compensations might be exerted when walking using the device. Additional kinematics using 3D motion analysis study will be needed. Lastly, the effect of using the device for a long period through gait training was not investigated. Therefore, the effectiveness of these devices should be investigated in high-quality clinical studies such as randomized controlled trials.
Conclusion
Through the present study, it was found that the one-arm motorized gait device was more effective for gait assistance in terms of spatio-temporal gait characteristics compared to traditional gait assistance devices. Therefore, one-arm motorized gait devices may be suggested as effective gait assistive devices for survivors with chronic hemiplegic stroke who have a difficulty in walking independently owing to decreased gait ability.
Ethics statement
The study purpose and procedure were fully explained to all subjects before obtaining their written consent for participating in the study. The study protocol was approved by the Institutional Review Board of Kyungnam University.
Funding
This study was supported by the Translational Research Program for Rehabilitation Robots (NRC TR-EX18007), National Rehabilitation Center, Ministry of Health and Welfare, Korea.
Footnotes
Conflict of interest
The authors have no conflict of interest to declare.