
Abstract
BACKGROUND:
Chronic obstructive pulmonary disease (COPD) is a common chronic respiratory disease worsening airflow limitation.
OBJECTIVE:
To explore pulmonary function rehabilitation, life quality and prognosis in patients with severe COPD.
METHODS:
Between February 2018 and August 2021, 150 patients with severe COPD cured in our hospital were arbitrarily assigned into the control group (
RESULTS:
There was no remarkable difference in BODE score before treatment (
CONCLUSION:
The application of multidisciplinary diagnosis and treatment model can promote the rehabilitation of pulmonary function of patients with severe COPD, improve their prognosis, slow down the development of the disease and enhance their life quality.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic respiratory disease worsening airflow limitation due to chronic airway exposure to noxious particles or gases can result in airway and/or alveolar abnormalities [1]. As a systemic disease, COPD not only directly affects the respiratory system, but also influences the circulatory system, skeletal muscle system, and mental and psychological aspects. Chronic hypoxia eventually leads to higher-than-normal pulmonary arterial pressure, and the right heart gradually thickens and expands to adapt to the changes, eventually leading to systemic cardiac insufficiency [2]. COPD is poisoning patients in many ways, daily activities and social activities are seriously limited, COPD has become a global public health problem. A survey in China in 2018 showed that there were 99.9 million COPD patients in China, with a prevalence rate of 13.7% in people over 40 years old and over 27% in people over 60 years old, and the number continued to rise [3, 4]. There is a high morbidity, disability rate, and mortality rate associated with COPD. As a result, the medical expenses incurred by patients in the treatment of COPD often exceed their affordability. Some studies conducted a systematic review of the financial burden of COPD patients in the United States, Europe and Asia. The results showed that the annual hospitalization cost of COPD patients in the United States is $6852 per person, while that in China is $1477 per person, and the medical cost in Europe is even higher. $8203 per person in Italy and as high as $11787 per person in Norway [6]. In the United States, modeling of the economic burden of COPD patients estimates direct medical costs from COPD to be $800.9 billion in 2038 and COPD-related deaths to reach 9.42 million [7]. The World Health Organization (WHO) predicts that COPD will become the third leading cause of death in the world by 2030, and the diagnosis and treatment of COPD is becoming an important global research topic [8].
In 2021, the Global Initiative for COPD clearly pointed out that the management of COPD includes drug intervention and non-drug intervention. Drug intervention is mainly the use of bronchodilators, antibiotics/bacteriostasis, glucocorticoid and other drugs, while non-drug intervention includes oxygen therapy and lung rehabilitation [9, 10]. To date, drug therapy is still the main treatment of COPD patients. However, repeated and long-term use of glucocorticoids, bactericides or antimicrobials can easily cause opportunistic infections, including bacterial, fungal, viral and special pathogens such as Mycoplasma pneumoniae and Mycobacterium tuberculosis. With the extension of the history of COPD patients, the drug resistance of pulmonary pathogens gradually increases, which brings further challenges to clinical diagnosis and treatment. In recent years, scholars and experts at home and abroad have been devoted to exploring more optimal treatment options for COPD patients. With the deepening of research, the multidisciplinary diagnosis and treatment model has attracted more and more attention as a simple and economical treatment method [11]. The multidisciplinary care model is patient-centered. The person in charge organizes experts from relevant departments to analyze and discuss the patient’s condition and data on a regular basis, and jointly formulate the most suitable treatment strategy for the patient. It is then up to the specialist to implement a treatment plan to help patients achieve better outcomes and live better lives [12]. This model originated from the United Kingdom in the 1960s and 1970s, and was applied to many fields under the promotion of the United Kingdom in the 1990s and developed around the world [13, 14, 15]. At present, although the multidisciplinary diagnosis and treatment model has been widely used in the treatment of severe COPD patients, previous studies have limitations such as few test samples and incomplete observations, resulting in insufficient convincing test results. In this context, it is necessary to carry out further relevant research to fully demonstrate the application value of the multidisciplinary diagnosis and treatment model for severe COPD patients. Based on this, the current study conducted a retrospective cohort study to explore the effect of using a multidisciplinary diagnosis and treatment model on pulmonary function recovery, life quality and prognosis in patients with severe COPD.
Patients and methods
General information
Between February 2018 and August 2021, 150 patients with severe COPD treated in our hospital were arbitrarily assigned into the control group (
The pulmonary function classification requirements are a set of criteria used to classify the severity of lung disease based on the results of pulmonary function tests. Different classification systems, such as GOLD, ATS, ERS, and GLI, utilize various combinations of spirometry measurements, including FEV1, FVC, and their ratio, to categorize the severity of lung disease into different stages. The severity of lung disease is usually classified as mild, moderate, severe, or very severe. It is important to note that while these classification systems provide useful information about lung function, they should be used alongside other clinical information when making treatment decisions for individual patients.
Inclusion criteria: (1) patients met the relevant diagnostic criteria for COPD in the “Guidelines for the Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease (2013 Revision)” [16], and met the severe criteria according to the pulmonary function classification requirements (FEV1%pred
Exclusion criteria: (1) patients with other respiratory diseases affecting pulmonary function, such as pulmonary tuberculosis, bronchial asthma, interstitial pneumonia, bronchiectasis; (2) heart, liver, and kidney failure; (3) severe cardiovascular and cerebrovascular diseases, severe systemic infection, malignant tumors, and mental diseases; (4) elevated blood eosinophils; (5) glaucoma and urinary retention.
Treatment methods
The control group accepted routine treatment, and was cured with anticholinergic drugs, inhaled
Multidisciplinary diagnosis and treatment for COPD patients involves a team of healthcare professionals working collaboratively to provide comprehensive care to individuals with COPD. This approach encompasses accurate diagnosis, smoking cessation, appropriate medication, pulmonary rehabilitation, oxygen therapy, and surgery, if necessary. A multidisciplinary team ensures that each patient receives individualized care that meets their unique needs, based on factors such as disease severity, symptoms, and other medical conditions. This approach aims to improve patient outcomes and overall quality of life. The research group would accept a multi-disciplinary diagnosis and treatment model, and following are specific measures.
1) Health education: nurses in the respiratory department gave health education to patients, including explaining the risk factors of COPD to patients and their families. The patients were encouraged to maintain regular work and rest and stay away from harmful gases and dust. Through pictures, educational manuals, one-on-one, and oral education, patients learn the basic knowledge of COPD, including commonly used drugs for COPD, special treatment methods, self-disease control skills, self-disease monitoring and treatment timing.
2) Limb exercise: cardiopulmonary exercise tests were performed by respiratory doctors; exercise programs were made according to the patient’s individual maximum exercise power (Wmax). The limb exercises were carried out under the guidance of rehabilitation therapists. Lower limb exercise indicated power bicycle endurance exercise, 30 min/times, 3 times per week. The initial exercise was to achieve the low-intensity exercise of individual Wmax 35%–40%. The final exercise goal was to achieve individual Wmax 50%–85%. Upper body training used unsupported weight-bearing exercises. The patient sat in a sitting position, with the knees vertical and the back against the chair back, doing 5 sets of movements each time, and each movement was repeated 5 times; the initial weight was 0.5 kg and the weight could be gradually increased.
3) Respiratory training: respiratory muscle functional exercise was carried out under the guidance of rehabilitation therapists, including respiratory gymnastics, abdominal breathing, lip contraction breathing, 15 min/times, 3 times per week. Abdominal breathing: the patient stood to relax the muscles of the whole body, the left hand was placed in front of the chest, the right hand was placed on the upper abdomen. The abdomen expanded when inhaling, the right hand was raised, the right hand was flat when the exhalation sank, and the right hand pressed the back and chest. The left hand remained motionless in the process of breathing, and the ratio of exhalation to inhalation was 2:1. Lip contraction breathing: inhale through the nostrils, exhale the lips, so that the gas naturally exhaled from the lips, the ratio of exhalation to inspiratory time was 2:1. The patients skillfully mastered abdominal breathing and lip contraction breathing and then applied them to daily life to form a natural breathing style. Abdominal breathing, also called diaphragmatic breathing, involves using the diaphragm muscle to draw air deep into the lungs. This technique is characterized by the expansion of the abdomen during inhalation. Abdominal breathing is frequently used in relaxation exercises like yoga and meditation to induce calm and relaxation. On the other hand, pursed-lip breathing, also known as lip contraction breathing, is a technique used primarily by people with lung diseases like COPD to alleviate breathing difficulties. Pursed-lip breathing is performed by inhaling through the nose and exhaling through pursed lips, as though blowing out a candle. Pursed-lip breathing can also slow down the respiratory rate, lower anxiety levels, and increase oxygen saturation in the blood. It is often utilized in pulmonary rehabilitation programs for people with lung diseases.
4) Nutrition guidance: nutritionists would evaluate the nutrition of the patients, comprehensively consider their body needs, disorders and eating habits, formulate a diet plan for three meals a day, and adjust in time in accordance with the changes of the patient’s condition in order to reduce the incidence of malnutrition.
5) Medication guidance: the patients were guided by clinical pharmacists according to the patient’s condition and the use of drugs, and implemented safety supervision to reduce the occurrence of drug side effects.
6) Psychological support: in the process of receiving treatment, psychiatrists were followed up regularly to evaluate the psychological status of patients, timely find patients with anxiety, depression and other psychological problems, and give early treatment. Patients with family and life difficulties should be given necessary help by workers of relevant social institutions to reduce the pressure of the patients as much as possible.
Observation index
Body weight – Body mass index, airflow obstruction, dyspnea and exercise (BODE) index
The BODE index includes the following items [17]: 1) BMI:
Pulmonary function
The German JAEGER pulmonary function tester was used to test the pulmonary function when the patient’s condition was stable. Before the examination, the patient had a quiet rest for 15 minutes. They then were measured his height and weight, informed the patient of the necessity. Pulmonary function tests were performed with the patient sitting with the airway straight. The technician will do 1–2 demonstrations of inhalation and blowing, and instruct the patient to bite and tighten the mouth as tightly as possible to ensure that there is no air leakage during the test. The patient inhales calmly, exhales several times, then inhales quickly and forcefully, exhales at maximum intensity and speed, and exhales continuously for 6–10 seconds to reach the expiratory plateau or until no more air is expelled from the lungs. Record the patient’s forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), forced expiratory volume in one second/Forced Vital Capacity (FEV1/FVC), and forced expiratory volume in 1 second.
Statistics of the number of acute attacks
The patients were followed up for 6 months, and the number of acute episodes was recorded.
6-minute walking distance (6MWD) experiment
The 6MWD package was adopted to assess the patient’s exercise endurance. The test was carried out on the marked distance, straight, barrier-free corridor in the hospital department (every 5 meters marked, a total of 30 meters). Patients needed loose clothing and sneakers, rest for 10 minutes before the test and avoid strenuous exercise. The patients were informed of the purpose and method of the test, and told to walk back and forth as quickly as possible during the test. 30 m is a circle. The patient did his best to walk within six minutes. If the patient felt shortness of breath and discomfort, the breathing and walking speed can be adjusted and the doctor should be informed promptly. Before the test, the patient’s oxygen saturation, heart rate, blood pressure, and Borg score were recorded. During the test, the patient minimized the doctor-patient dialogue, and the doctor reminded the patient of the remaining time every 1 minute. If the patient needs to stop and rest during the test, adjust the breathing, and continue walking until the end of 6 minutes, and the final walking distance was recorded. In addition to the evaluation before treatment, two months later and six months later, patients were also evaluated after treatment.
Borg score
Borg scale is used for the degree of dyspnea felt by patients during exercise [18], and is often used in the 6MWD. The score included 0, 0.5, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10 points. 0 was seen as no dyspnea after exercise, and 10 was seen as the most severe dyspnea. In addition to the evaluation before treatment, two months later and six months later, patients were also evaluated after treatment.
Life quality
The life quality was investigated and evaluated with St. George’s Respiratory questionnaire (SGRQ) [19], which was assigned into three functional scores. The activities included limitation of clothing, climbing and housework, and influence scores including insecurity, anxiety, disappointment, social activity and so on. Patients filled in the questionnaire independently and calculate the score of each function and the total score of the questionnaire. The lower the score, the better the life quality. A pre- and post-treatment evaluation was conducted on the patients.
Statistical analysis
In the analysis and processing of all experimental data, SPSS21.0 software was used, and count data were expressed as [
Results
BODE score comparison
In the absence of treatment, there was no noticeable difference in BODE scores (
BODE scores between the two groups [
s, points]
BODE scores between the two groups [
The pulmonary function between the two groups [
The FVE1%pred, FEV1, and FEV1/FVC in the study group were higher (
The number of acute attacks
The number of acute attacks in the study group was lower (
6MWD comparison
6MWD comparison, before treatment, there exhibited no remarkable difference (
The 6MWD between the two groups [
s, m]
The 6MWD between the two groups [
Borg scores between the two groups [
Comparison of the number of acute attacks.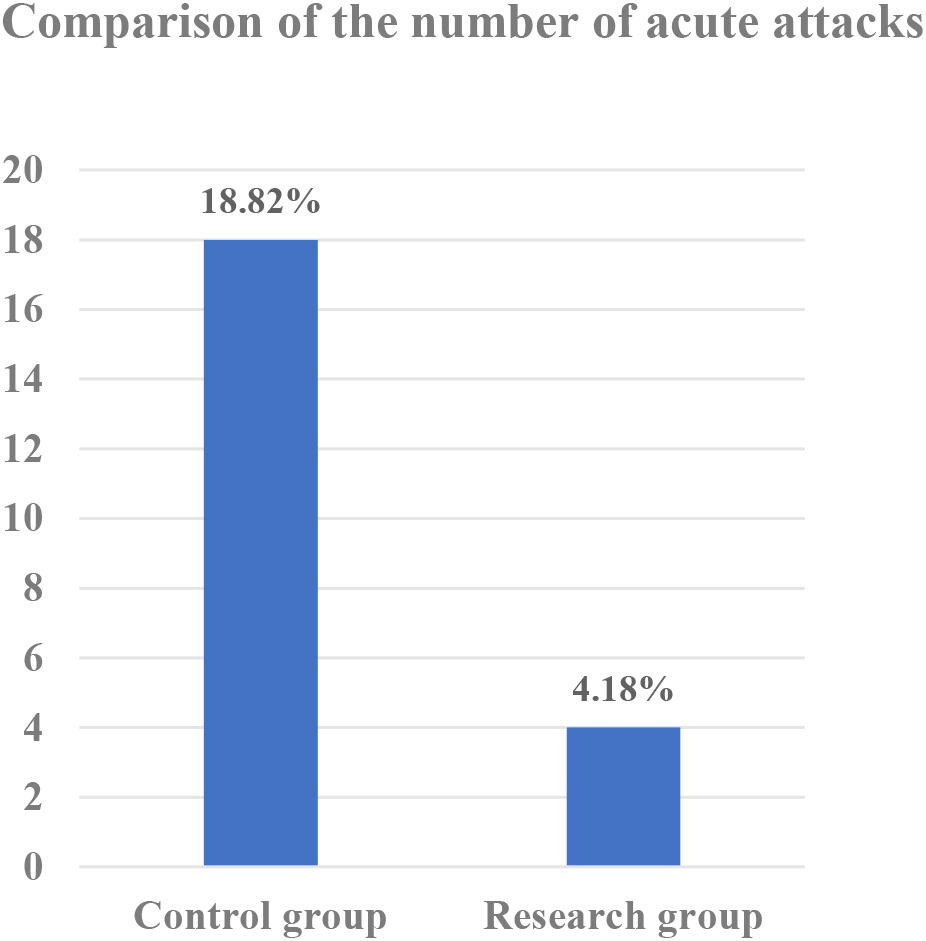
Before treatment, there exhibited no difference in Borg score (
The life quality scores between the two groups [
s, points]
The life quality scores between the two groups [
Note:
There exhibited no remarkable difference in the score of life quality before treatment (
Discussion
COPD is an increasingly prevalent respiratory disease and is expected to become the third most common and fatal disease globally by 2030 [20], placing a heavy medical burden on society. COPD is the lung disease with irreversible disease progression, and its current treatment strategies are aimed at relieving symptoms, enhancing exercise tolerance, promoting health status, preventing disease, and managing disease exacerbation. With the progress and the continuous updating of non-drug treatment approaches, the current multi-disciplinary comprehensive intervention treatment program can better improve the efficacy, especially the application of lung rehabilitation therapy. The GOLD guidelines clearly point out that pulmonary rehabilitation training can alleviate patients’ respiratory symptoms, improve exercise tolerance and life quality, and reduce acute exacerbations of the disease, thereby effectively slowing the development of COPD [21, 22, 23]. Clinically, the dose-effect relationship between the duration of lung rehabilitation and the effect of lung rehabilitation in patients with severe COPD is not clear. Moreover, the relationship between stable COPD patients with different severity and the effect of lung rehabilitation still needs further study [24].
Most patients with COPD have persistent respiratory symptoms and limited ventilation function. The most common symptoms include dyspnea, obvious cough and expectoration. These symptoms persist for a long time and may worsen periodically. At the same time, COPD affects all systems of the patient’s body, and patients often have skeletal muscle system dysfunction. This can lead to muscle atrophy, weakness and severe respiratory muscle dysfunction, resulting in increased dyspnea, reduced activity endurance and life quality, and reduced life expectancy [25, 26]. In the treatment of COPD, we should pay attention to the following: (1) Avoiding risk factors: quitting smoking is a potent way to reduce the risk of COPD and delay the decline of pulmonary function. Smokers should be urged to quit smoking and should be told to avoid second-hand smoke inhalation as much as possible. In addition, the inhalation of hazardous substances in the work environment is minimized or controlled, and measures are taken to reduce or avoid indoor and outdoor air pollution [27]. (2) Drug therapy: drug therapy can reduce clinical discomfort, improve exercise tolerance, improve general condition and reduce disease deterioration, which is the key measure for the treatment of COPD [28, 29, 30, 31]. Common therapeutic drugs consists of bronchodilators, glucocorticoids, antibiotics, expectorant and so on. Bronchodilator is the most commonly used drug in the treatment of COPD. According to different mechanisms of action, drugs for the treatment of COPD can be assigned into three categories, including
Non-drug therapy is also a key component of the treatment of COPD. As an adjuvant therapy of drug therapy, non-drug therapy can cooperate with drug therapy to reduce subjective symptoms such as shortness of breath, improve lung function and improve life quality. It mainly includes lung rehabilitation, vaccination, medical intervention and surgical intervention. Lung rehabilitation (PR) is an indispensable part of non-drug treatment for COPD patients. GOLD guidelines have clearly pointed out that lung rehabilitation can improve clinical symptoms, exercise tolerance, overall life quality and emotional state of COPD patients. Lung rehabilitation can also relieve the pressure of health care expenditure on the disease by reducing the number of acute exacerbations and the length of hospital stay.
Although the best drug treatment is given to patients with severe COPD, there is no drug to change the progressive decline of lung function, some patients will still feel dyspnea and daily activities will be disturbed. Nowadays, the benefits of multidisciplinary diagnosis and treatment model in COPD patients has been widely recognized. Scholars have carried out various forms of research on the multidisciplinary diagnosis and treatment model of severe COPD patients [38, 39, 40]. Foreign scholars have found that regardless of the degree of airflow obstruction, a 6-week multidisciplinary diagnosis and treatment model for severe COPD patients can improve exercise tolerance, lung function, and life quality [41]. In addition, patients who maintain a multidisciplinary diagnosis and treatment model for a long time can maintain this benefit. By observing a 5-year cohort study aimed at evaluating the effectiveness of a multidisciplinary diagnosis and treatment model for patients with COPD, foreign scholars have found that in the first 6MWD and health-related life quality scores at 4 years and MRC scores at 5 years showed a remarkable benefit, and 5-year survival rates were higher than in patients who did not maintain a multidisciplinary care model [42].
COPD patients may suffer from loss of appetite, respiratory dysfunction, peripheral muscle atrophy, and negative psychology during long-term treatment, resulting in decreased life quality [43]. The traditional diagnosis and treatment model is relatively simple, and it is difficult to achieve the purpose of comprehensive treatment. In this study, the traditional medical model was used as the control group to analyze the feasibility of applying the multidisciplinary diagnosis and treatment model to the treatment of COPD. Some scholars have compared and analyzed 64 patients, of which 32 patients in the observation group received the intervention of a multidisciplinary cooperative team composed of respiratory physicians, nurses, rehabilitation doctors, nutritionists and psychological consultants. The results showed that the group paid attention to exercise tolerance at various stages after discharge. The improvement of pulmonary function indexes and symptoms were better compared to the control group [44]. It has shown that the multidisciplinary cooperation model has definite effect in improving the patient’s condition and promoting the patient’s recovery. In this study, elderly patients with COPD were treated with a multidisciplinary diagnosis and treatment model. After treatment, the BODE score of the study group was lower at 2 months and 6 months after treatment. The number of acute attacks in the study group was lower. 6MWD of the study group at 2 months and 6 months after treatment was higher. The Borg score of the study group at 2 and 6 months after treatment was lower. The results were consistent with the above reports. Another study pointed out that multidisciplinary cooperation can not only promote the improvement of symptoms, but also have a positive impact on the nutritional status, emotional status, and compliance of patients, and is of great significance in enhancing the life quality of patients [45]. The above indicators in the study group were better, which could better improve the patient’s condition and prognosis. Because in the multidisciplinary diagnosis and treatment model, doctors can intervene in all aspects of the disease. Through physical exercise, health education, breathing training, nutritional guidance, medication guidance and other measures, patients gradually improve their symptoms, signs and physiological indicators. In this study, in order to further confirm the improvement effect of the multidisciplinary diagnosis and treatment model on the life quality of patients with COPD, the SGRQ scale was used to comprehensively evaluate the patients’ social activities, psychological status, illness, daily life and other aspects. The pred FEV1, FEV1/FVC were higher compared to the control group. The lung function indexes of the patients in the study group were remarkably improved. Under the multidisciplinary diagnosis and treatment mode, various interventions such as limb exercise and breathing training are used to improve their respiratory function, thereby promoting the gradual improvement of lung function. The pulmonary function index is an important reference for the improvement of the condition of COPD patients. The pulmonary function index of the patients in the research group improved remarkably, indicating that their condition is developing in a better way. Comparison of quality-of-life scores, the symptom score, activity score, influence score and total score of the study group were lower. It is suggested that the cardiopulmonary function and daily living ability of patients can be gradually improved through rehabilitation treatment. Regular intervention of psychotherapists can also reduce the psychological burden of patients. The improvement of physical and mental state can help to further improve the life quality of patients and make them return to normal life as soon as possible. Some scholars have believed that multidisciplinary cooperation can save medical resources, strengthen the cooperation of various specialties, and avoid the limitations of a single discipline [46, 47, 48, 49].
Conclusion
The applications of multi-disciplinary diagnosis and treatment model can promote the rehabilitation of pulmonary function in patients with severe COPD, improve their prognosis, slow down the development of COPD, and enhance their life quality. Multidisciplinary diagnosis and treatment of COPD has also certain limitations, because the study is retrospective and the study is conducted in a single center, which limits the generalizability of the findings. Further, the follow-up period of the patients is very less. So, in future we would like to analyze the study using multiple centres with maximum follow-up time period.
Footnotes
Conflict of interest
None to report.