
Abstract
BACKGROUND:
The global community is faced with aging societies, which will result in increased health care costs. we have been introducing our International Organization for Standardization (ISO)-certified health education system in Thailand and Indonesia.
OBJECTIVE:
The purpose of this study was to collect data on the effects of this ISO-certified health education system, to extend the healthy life expectancy and to study the feasibility of implementing this program and in new social contexts.
METHODS:
We implemented the health education program recruiting 43, 114 and 119 participants, respectively, in Japan, Thailand and Indonesia. The participants’ conditions before and after the program were determined through anthropometry, physical fitness tests, blood chemistry tests, brain function tests and pedometry.
RESULTS:
Regarding pedometry, the Japanese participants took the highest number of daily steps on average, followed by the Indonesian and Thai participants. In the 10-m obstacle walk, the Thai and Indonesian participants had significantly increased times. Furthermore, the differentiation reaction time, reverse differentiation reaction time, total number of “misses”, total number of “mistakes” and total number of errors significantly improved.
CONCLUSION:
It is possible to implement a program of an ISO-certified health education system, but how to develop exercise habits is important.
Background
In 1978, the World Health Organization defined and advocated for “primary health care,” which concerns health care provided in communities with a focus on prevention and treatment [1]. In 1986, this concept was redefined as “health promotion,” which involves enabling people to increase their control over their health [2]. Sustained physical activity reduces the risk of lifestyle-related diseases [3]; however, there are situations in which it is difficult to maintain physical activity [4].
Since 1988, we have incorporated dementia prevention activities into our systematic health education programs, targeting young older adults in five areas of Nagano Prefecture. Through these programs, we have administered comprehensive social capital-oriented health education based on fostering empathy and cooperation. In 2014, these health education systems were awarded International Organization for Standardization (ISO) 9001; QC14J0022 certification, which is an international standard [5, 6, 7, 8].
In Thailand, in 2005, the percentage of the population over 65 years of age was 7%, and this percentage is expected to rise to 14% by 2025; meanwhile, in Indonesia, this percentage is projected to reach 7% by 2020 and 14% by 2045. Thus, in addition to Japan, several other Asian countries are also facing challenges regarding their aging populations [9]. Consequently, implementing an ISO-certified health education system such as the one that we have developed to promote dementia prevention activities can play an important role in this region, contributing to extending the population’s life expectancy and controlling medical expenses [10, 11, 12, 13]. Since 2013, in cooperation with Mahidol University, Thailand, and Udayana University, Indonesia, we have introduced our ISO-certified health education system into the areas surrounding both universities [14, 15, 16, 17].
The purpose of this study was to collect data on the effects of an ISO-certified health education system and to study the feasibility of this program in new social contexts.
Methods
General methods
For this research, the ISO 9001; QC14J0022-certified health education system was introduced into the Nikhom Phatthana District, Rayong Province, central Thailand, and Denpasar City and Tabanan Regency, Bali, Indonesia (Fig. 1). The ISO is a non-governmental organization headquartered in Geneva, Switzerland, and its main activity is to establish internationally accepted standards [18]. Our ISO-certified health education system collects anthropometry, blood pressure, blood chemistry, physical fitness, and brain function data before and after the health education program. These data are collected in the same way in all countries (Fig. 2).
ISO health education flowchart.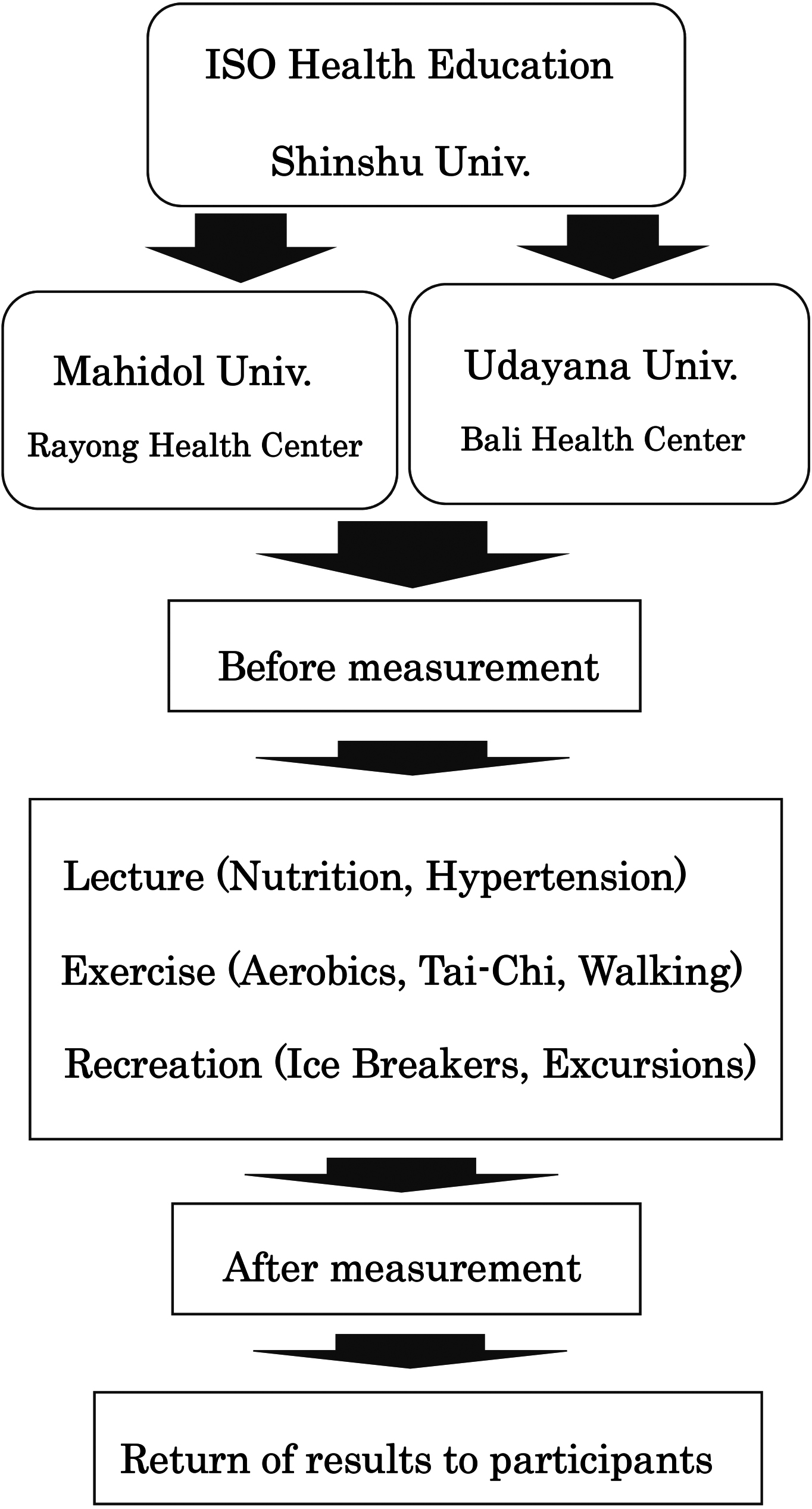
All participants were healthy, middle-aged to older adults (42–86 years) with no history of cardiovascular or pulmonary diseases. They provided written informed consent and were enrolled in the health education programs in their communities in Thailand, Indonesia, and Japan. Participants were informed of the safety of participation in this study. Participation in this study is voluntary and should not be adversely affected by non-participation. Even if they agree to participate once, they can withdraw at any time. The programs were offered by the health centers in each country. The participants agreed to participate in this research as volunteers after receiving a detailed explanation of the ISO-certified health program.
In Thailand, we implemented a six-month health education program from August 2013 to January 2014; in Indonesia, we implemented a seven-month program from February to August 2014; and in Japan, we implemented a six-month program from June to November 2013. Before and after the implementation of the health education program, we conducted physical fitness, blood chemistry, and brain function tests. The control participants were not given pedometers. There were 114 Thai participants (aged 60.5
Program contents of the health education in Thailand, Indonesia, and Japan
ISO 9001 health education services implementation status.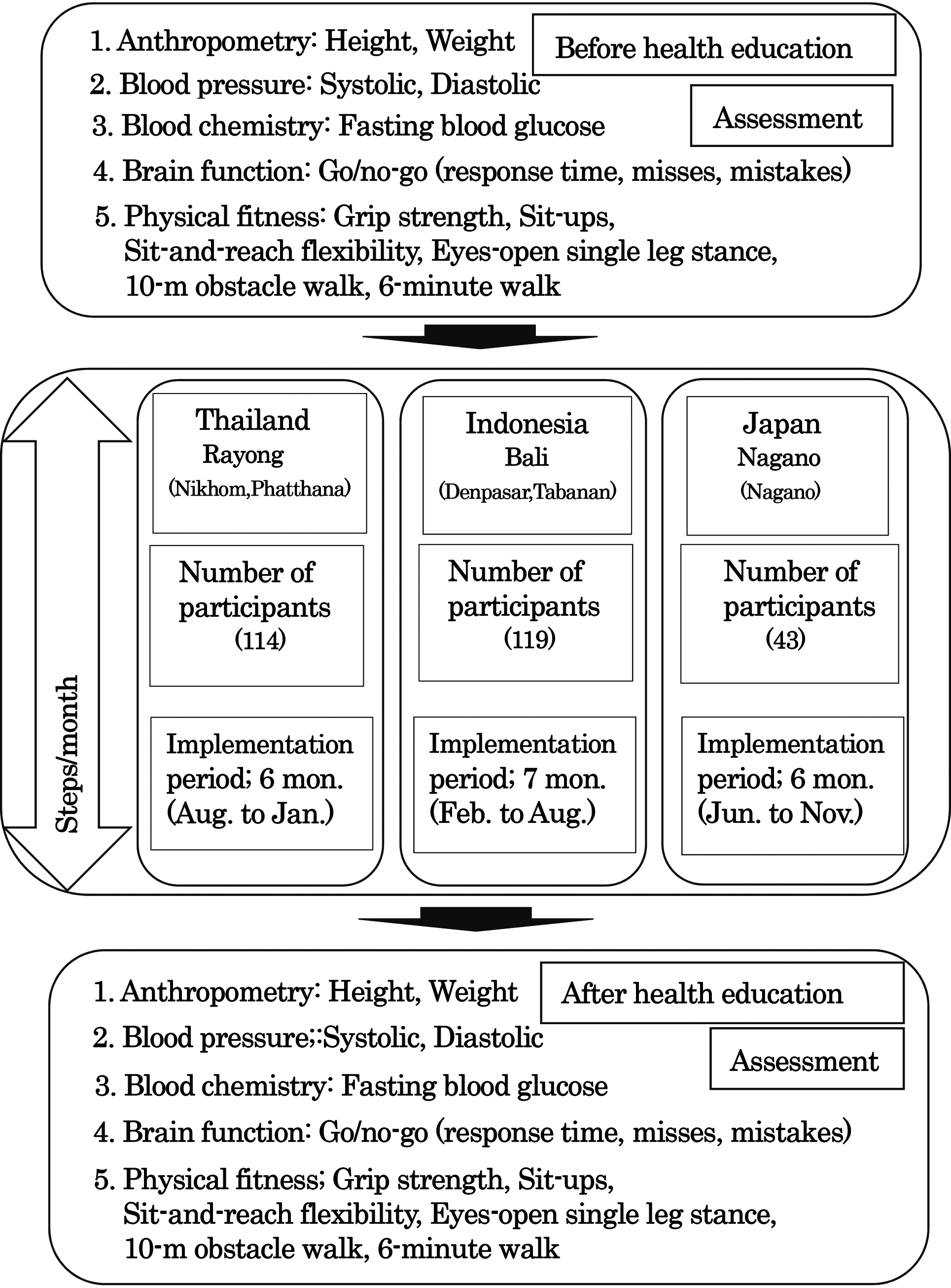
This research was approved by the institutional ethics committees of Mahidol University (no. 01-58-10) and Shinshu University (no. UMIN000009309) and in accordance with the code of ethics of the World Medical Association. Written informed consent was obtained from all participants.
The number of steps taken each day and energy expenditure were measured using a pedometer (Acos Co. Ltd., Japan; JP800). Daily total steps were divided into “exercise-related” steps (steps exceeding four metabolic equivalents [METs]) and “normal” steps (less than four METs). For all groups, steps were measured throughout the program period.
Anthropometry, blood chemistry measurements and blood pressure measurements
These measurements and the blood chemistry measurements were taken when the participants were in a fasted state (
Physical fitness tests
The administered physical fitness test was approved by the Japanese Ministry of Education, Culture, Sports, Science and Technology [19]. This test (target age: 65–79 years) features six physical assessments: hand-grip strength, sit-ups, sit-and-reach flexibility, an eyes-open single-leg stance, a 10-m obstacle walk, and a six-minute walk test. The participants’ physical ability was assessed before and after the health program.
Brain function tests
The go/no-go task [20, 21, 22] was used to estimate the inhibitory decision-making process, and this task consisted of three experimental stages: formation, differentiation, and reverse differentiation. First, in the formation stage, which consisted of five trials, the participants were instructed to squeeze a rubber ball in response to the illumination of a red light, which occurred at random intervals. Second, during the differentiation stage, the participants squeezed the rubber ball in response to the red light but refrained from doing so when the yellow light was illuminated. Third, during the reverse differentiation stage, the participants squeezed the rubber ball in response to the yellow light but not the red light. The differentiation and reverse differentiation stages consisted of 20 trials each; in both, the red and yellow lights were randomly illuminated 10 times each.
Statistical analyses
One-way analysis of variance (ANOVA) was performed to compare the step counts of the three groups, and when a significant difference was observed, Tukey-Kramer post hoc comparisons were performed. Two-way repeated-measures ANOVA was employed to compare the results before and after the health education program. When significant interactions were found, one-way ANOVA was conducted; then, Tukey-Kramer post hoc comparisons were performed if ANOVA showed significant results. Additionally, a paired-samples
Results
Pedometry
Figure 1 shows the average daily number of total (normal steps
Pedometry comparison of the steps in Thailand, Indonesia, and Japan
Pedometry comparison of the steps in Thailand, Indonesia, and Japan
T: Thailand (
The average daily number of total and exercise-related steps taken each month by the Thai, Indonesian, and Japanese participants. M; month, T; total steps, E; exercise-related steps.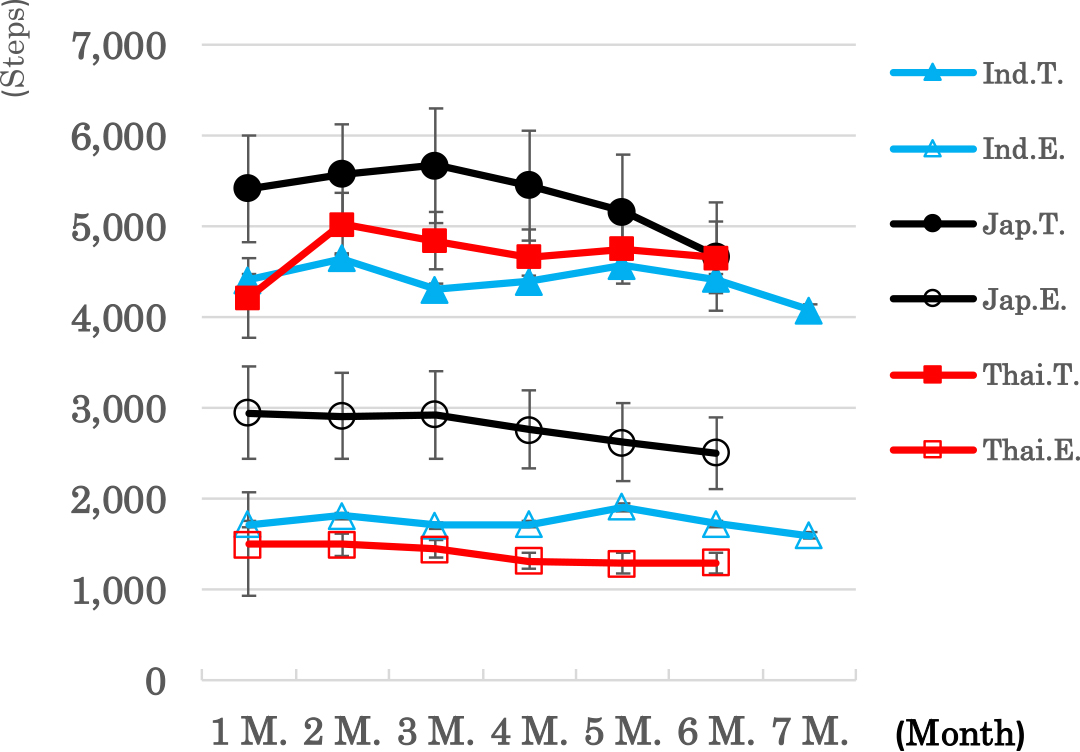
The Thai participants’ weight significantly increased after the program. For the Indonesian participants, their systolic blood pressure was significantly different. The interaction of the minimum blood pressure in two-way ANOVA significantly differed; consequently, one-way ANOVA was used to interpret the before and after results of all groups; this analysis showed no significant difference (Table 3).
Comparison of before and after health program in Thailand, Indonesia, Japan, and Japan’s control group
Comparison of before and after health program in Thailand, Indonesia, Japan, and Japan’s control group
B/A: main effect of before and after, T/I/J/C main effect of Thailand (
For the Thai participants, hand-grip strength and sit-and-reach flexibility significantly increased; in contrast, performance on the eyes-open single-leg stance significantly worsened. For the Indonesian participants, performance on the 10-m obstacle walk significantly improved; however, the number of sit-ups significantly decreased. For the Japanese participants, the number of sit-ups significantly increased. The interaction of sit-and-reach flexibility, the eyes-open single-leg stance, and the 10-m obstacle walk in two-way ANOVA was significant; thus, one-way ANOVA was used to interpret the before and after results of all groups. The results for sit-and-reach flexibility and the eyes-open single-leg stance showed no significant differences; however, among the Indonesian participants, performance on the 10-m obstacle walk significantly improved (Table 3).
Brain function measurements
For the Thai participants, the average differentiation reaction times, reverse differentiation reaction times, and total reaction times significantly increased after the program. Meanwhile, the total number of “misses”, “mistakes”, and errors significantly decreased after the program. The interaction of the total number of “misses” and errors was significant. The total number of “misses” among the Thai participants and the total number of errors among the Thai and Indonesian participants significant decreased.
Discussion
Regarding exercise-related steps, the Thai, Indonesia and Japan participants respectively, took 1,395 (30% of the number of total steps), 1,744 (40% of the number of total steps), and 2,782 (55% of the number of total steps) daily steps. In the future, it will be necessary to make an effort to increase the number of exercise-related steps. It has been reported that such walking is effective at preventing dementia; forty minutes of active walking a week over the course of a year results in a 2% increase in the hippocampal volume and improves memory [23].
The Thai participants’ weight increased significantly after the health education program. Conversely, the other participants lost weight, but the difference was not statistically significant. The participants’ BMI values did not significantly change in any group. In previous studies, significant improvements in body weight, BMI, blood pressure, and blood chemistry were found when the subjects incorporated walking and exercising into their lifestyle [3, 24, 25, 26]. Thus, increasing the average number of total steps may help the participants in the present study improve in this regard.
Among the Thai participants, hand-grip strength and sit-and-reach flexibility significantly increased; in contrast, performance on the eyes-open single-leg stance test significantly worsened. For the Indonesian participants, performance on the 10-m obstacle walk significantly improved, while the number of sit-ups significantly decreased. For the Japanese participants, the number of sit-ups significantly increased. However, there are few improvement items for physical fitness in Thailand, Indonesia, and Japan. If the average number of total steps taken by participants is 7,000 or more, the improvement rate of physical fitness measurement items will significantly increase [5, 6, 7, 8].
Go/no-go tasks are frequently used to investigate response inhibition, which is an essential executive function performed by the prefrontal cortex, as well as a variety of other cognitive components [20, 21, 22, 27, 28]. In the present study, the interaction between the total number of “misses” and “mistakes” was significant for all groups. The Thai and Indonesian groups had significantly fewer total “misses” and errors after the program. Previous go/no-go task studies suggest that a health program could improve brain function [5, 6, 7, 8]. In the first stage of the go/no-go task, the reaction time is short and the number of errors is large. Participants performed regular exercises in the second stage, and the go/no-go task reaction times increase and the number of error responses decreased. In the third stage, the go/no-go task reaction times decreased significantly, and the number of error responses decreased significantly. In the Thai participants, the go/no-go results for the first stage improved.
Since pedometers were not given to the control group in Japan, there are no data on the number of steps taken by this group. However, in another study [29], control group members were 5,220. In this survey, the target value of 7,000, and also the target value of 7,000 steps by 2022 established by the Ministry of Health, Labor and Welfare of Japan by people aged 65 and over [30]. The target value of 7,000 steps was not achieved in all areas; only a few measurement items of anthropometry, blood pressure, blood chemistry, physical fitness, and brain function showed improvement, and some even showed a significant decrease as the participants aged. Therefore, it is important for participants to encourage and sympathize with each other and continue their health education program with the aim of achieving more than 7,000 steps without dropping out.
Limitations
In this study, our ISO 9001 program was provided for six months in both Japan and Thailand; however, in Indonesia, it was provided for seven months. The reason is that in Indonesia, the schedule for the ISO staff was not set; thus, the assessment was postponed by one month. Japanese participants were from Nagano City, Nagano Prefecture, Japan, and a control group composed of senior citizens, also in Nagano, was created. There were only seven participants in the control group since 17 participants dropped out; therefore, a control group was created only for the Japanese participants.
Conclusions
The purpose of this study was to collect data on the effects of an ISO-certified health education system and to study the feasibility of this program in new social contexts. To that end, we implemented the health program in Thailand and Japan, recruiting 114 and 43 participants, respectively, and in Indonesia, recruiting 119 participants. The participants’ conditions before and after the program were determined through anthropometry, physical fitness, blood chemistry, and brain function tests and pedometry. The Japanese participants in our study took 5,330 daily steps, the Thai participants took 4,696 daily steps, and the Indonesian participants took 4,406 daily steps. The target value of 7,000 steps was not achieved in all areas; only a few measurement items of anthropometry, blood pressure, blood chemistry, physical fitness, and brain function showed improvement, and some even showed a significant decrease as the participants aged. Therefore, it is important for participants to encourage and sympathize with each other and continue their health education program with the aim of achieving more than 7,000 steps without dropping out.
Author contributions
KT, AG, AN, SM, SK, TW, NT, RU and KA planned the experiment and collected the data. FS, MO, KK, HK and HT performed the data analysis. MK, TF, TN, KT and HT composed the article. All authors read and approved the final manuscript.
Availability of data and material
The data and materials are available.
Funding
Koji Terasawa is supported by grants-in-aid for scientific research (Kiban A: 16H02713) from the Ministry of Education, Culture, Sports, Science and Technology of Japan. The funder had no involvement in study design, the collection, analysis and interpretation of data, the writing of the report, or the decision to submit the article for publication.
Footnotes
Acknowledgments
The authors would like to thank all individuals who participated in this study.
Conflict of interest
The authors have no conflicts of interest to report.