
Abstract
Parkinson’s disease (PD) is a common neurodegenerative disease that manifests as a various movement disorders: tremor, rigidity and postural instability. These dysfunctions can significantly impact the individual’s quality of life, leading to a decline in overall well-being. However, recent innovations in medical devices field promise additional methods to alleviate PD symptoms. The VILIM Ball is a local hand-arm stimulation device that generates mechanical vibrations within the frequency range of 8–18 Hz. It was shown in this study that Parkinson’s disease patients (PD) may experience enhanced upper limb functionality and reduction in tremor power through physiotherapy in conjunction to therapy with VILIM Ball device. A total of 24 participants were recruited and divided into two groups: the control group (
Introduction
Parkinson’s disease (PD) is a common neurodegenerative disease of the central nervous system (CNS) with a possible genetic predisposition that results from the loss of dopaminergic cells in the black matter of the brain [1], and manifests as movement disorders: tremor, rigidity, bradykinesia, and postural instability. These dysfunctions can significantly impact the individual’s quality of life, leading to a decline in overall well-being [2, 3, 4, 5, 6, 7].
Tremor is an unintentional rhythmic movement of any part of the body. Shaking or trembling hands is a typical hand tremor symptom. Tremors are usually caused by problems with areas of the brain that control movements.
The two main diseases that cause chronic hand tremor are Essential Tremor (ET) and Parkinson’s Disease (PD). The problem exacerbates when patients try to do something, including simple tasks such as drinking from a glass, eating or tying shoelaces. For this reason, even if tremor is not a life treating disease, it has a great impact on the patient’s life quality, especially considering that ET symptoms typically worsens over time. Unfortunately, for some patients the intensity of the disease can be as severe as an invalidating condition.
Traditional treatment options for tremors, including medication and neurosurgical interventions, are not adequate for many patients. The use of drugs has historically been the primary treatment approach, but it often fails to produce the desired therapeutic response. This is due to the complex interactions between different drugs and the intolerable side effects experienced when using high doses to control tremors. In the case of Parkinson’s disease (PD), there is no medication that consistently alleviates the resting tremor. Dopaminergic drugs are frequenctly used as a mean of treatment but there is a significant fraction of patients whose tremor does not respond [16, 17]. On average both Levadopa and dopamine agonists reduce tremor only by 30% to 50% in the Unified Parkinson’s Disease Rating Scale (UPDRS) subtest for rest tremor [22].
Research on tremor pathophysiology shows that electrical stimulation of the peripheral nerves, mechanical perturbation of the limb, or transcranial magnetic stimulation of the motor cortex can alleviate tremor symptoms [18]. For individuals with severe and medically-resistant tremors, invasive procedures like deep brain stimulation (DBS) [19] or magnetic resonance-guided focused ultrasound (MRgFUS) may be considered. Also, electrical stimulation of muscles has been proposed for patients with less severe forms of PD tremor [20]. Transcutaneous afferent patterned stimulation (TAPS) of the median and radial nerves at the wrist, is the only peripheral electrical stimulation (PES) therapy currently approved by the United States Food and Drug Administration (FDA) for the clinical management of the Essential tremor and Parkinson’s disease symptoms [8, 15]. Such therapy involves tens of minutes of noninvasive electrical stimulation that alternates between the median and radial nerves at the wrist at a patient’s tremor frequency. In one related study, 40 PD patients with postural tremor were enrolled in a remote, prospective, single-arm, open-label study with 4 weeks of TAPS. Improvements among other variables were also calculated in a change in postural tremor power using accelerometer data. It was concluded that TAPS reduced postural tremor power by a median of 66% (
These options, even if proven efective for a lot of paitents, have drawbacks such as high costs, significant risks, potential for irreversible neurological damage, and consequently, varying acceptance rates among patients. Therefore, there is a pressing need for a safe and dependable first-line therapy that can effectively manage PD symptoms without causing the adverse effects associated with pharmacotherapy or the risks associated with invasive procedures [1, 8].
Rehabilitative therapy, such as occupational therapy and exercise complement pharmacologic treatments [1, 9]. Physical therapy is proven to slow down the progression of PD [10]. Another alternative is vibration therapy. It can be especially helpful in addition to physiotherapy. Applying vibration to the whole body or the upper extremities improves proprioception and relieves the symptoms of astigmatism and tremor. Still, it should be noted that vibration-induced effects provide only short-term improvement [1, 9, 11, 12].
The VILIM Ball is a therapeutic device designed to reduce hand tremors in ET patients. It delivers low-frequency vibratory stimulation to the upper extremities, aiming to alleviate symptoms in the period following treatment. It was shown that some ET and PD patients can experience improvements in tremor symptoms and function after using the device. A prospective, single-arm, pragmatic study involving 17 ET patients was conducted. Accelerometery was used to measure Patient’s tremor power 1 minute before and after the 5-minute-long hand stimulation using the VILIM ball. Study concluded a significant reduction in tremor power from the mean of 0.106
The safety and effectiveness of the VILIM ball were evaluated in a retrospective cross-sectional safety study involving 51 patients (31 ET, 20 PD). The main measure of effectiveness was based on a patient-reported outcome obtained through a non-validated telephone questionnaire. Safety evaluations were descriptive and conducted by the attending physician. The treating physician determined the necessity of physical examinations, monitoring vital signs, electrocardiography, and laboratory tests (including hematology, chemistry, and urinalysis) to assess safety. 48 patients reported improvement in tremor symptoms, and 49 reported an improvement in hand function. Average usage time was 7.63 (5.41) months. Thirty-eight patients reported the duration of improved function at an average of 90.79 (68.83) minutes. Two patients reported a lack of efficacy. No serious adverse events were reported.
Although vibrational therapy shows promise, there is still a lack of research, particularly in its application to Parkinsonian tremors and its combination with other forms of treatment. Therefore, this study was conducted to determine whether localized hand-arm vibration therapy can improve the effectiveness of traditional physiotherapy exercises for individuals with PD. Effectives was defined as improvement in functional parameters (grip strength and arm coordination) and tremor power.
Materials and methods
The study was conducted with Parkinson’s patients who were members of the Kaunas Parkinson’s disease society at Kaunas City Polyclinic by physiotherapists, at Kaunas Dainava Polyclinic Youth Center. Research was conducted with the formal approval of the local human subject care committees.
Study selection and exclusion criteria
Inclusion criteria:
Male and female subjects 50–80 years of age at the time of consent; Written informed consent provided by the patient; Patients diagnosed with Parkinson’s disease; Patients with PD that can control the movement of the torso and upper limbs independently.
Exclusion criteria:
Refusal to participate in the study; Non-compliance; Substance-dependence; Uncontrolled medical illness (arterial hypertension, diabetes, severe liver or kidney failure); Other subjects who, in the opinion of the investigator, have any acute or chronic medical or psychiatric condition or laboratory abnormality at the screening that would impair the subject’s capability to follow the study protocol.
VILIM ball device.
Vibrational therapy was performed with VILIM Ball (Fig. 1) device. The VILIM ball is a certified Class IIa medical non-invasive handheld therapeutic device that reduces hand tremor, provides symptomatic relief, and facilitates activities of daily living.
The device incorporates machine learning algorithms that use various sensors to analyse tremor and optimize vibrational therapy and interrupt the neurological loop that causes tremor. The VILIM Ball emits low-frequency mechanical vibrations in the range of 8–18 Hz. It is intended to be used in home and clinical environments. This device is produced by “VILIMED”,a Private Joint Stock Company accessible via
Study conduct
Study subjects were informed about the aims, methods, and the expected results of the research. Also, written informed consent form was obtained. Subjects were then divided into experimental and control groups using the stratified randomization method to control the covariates of sex (2 levels: male, female) and age. The control group (N
Functional assessments
Right hand coordination at baseline and after the intervention in both groups. *Statistically significant difference in comparing the right-hand index in the control group before and after the procedure (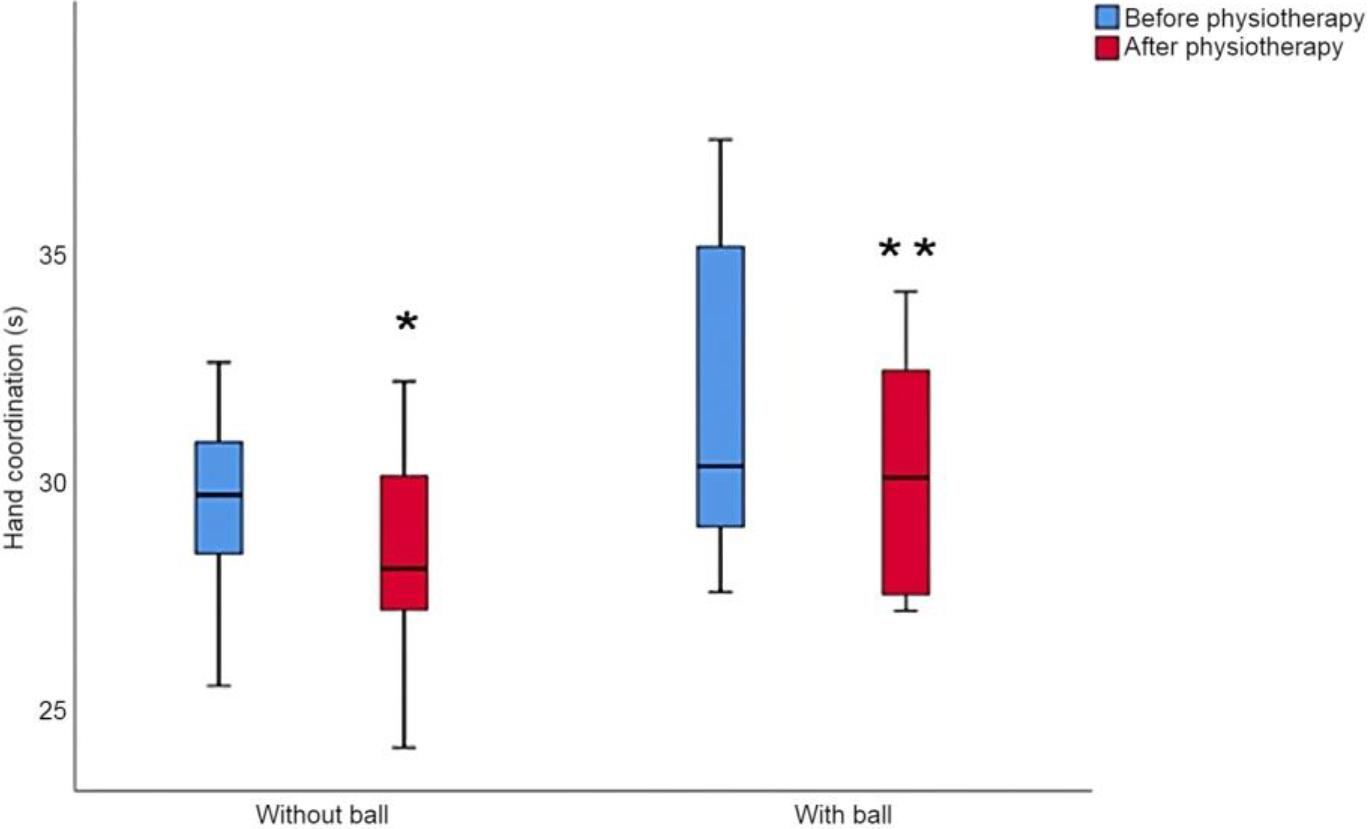
Hand dynamometer (microFET®2) was used to measure the grip strength – maximum gripping force in kilograms (0–90 kg). The subjects were assessed in a sitting position with arms bent at 90∘ through their elbows angled, tucked to the sides, and not placed on the supporting table. Measurements were taken only for the right hand, immediately before and after the interventions. Patients could make three attempts, but only the highest grip strength attempt was noted.
The arm coordination evaluation was performed using Nine-Hole Peg Test (9HPT). Test measures finger dexterity and hand coordination. During the measurement the patients were seated in a chair with their arms rested on a table in front of them with elbows in 90∘ flexion and palms downward. A pegboard with 9 holes was positioned in front of them. The participants were instructed to quickly remove all the pegs from the holes, place them into the container, then take back the pegs from the container, and put them back into the holes on the board. The test scores were based on the time taken to complete the test activity, recorded in seconds with a stopwatch [13]. This evaluation was performed separately for each hand immediately before and after the interventions.
Right hand coordination data
Right hand coordination data
Left hand coordination data
Left hand coordination at baseline and after the interventions. *Statistically significant difference in comparing the left arm index in the control group before and after the procedure (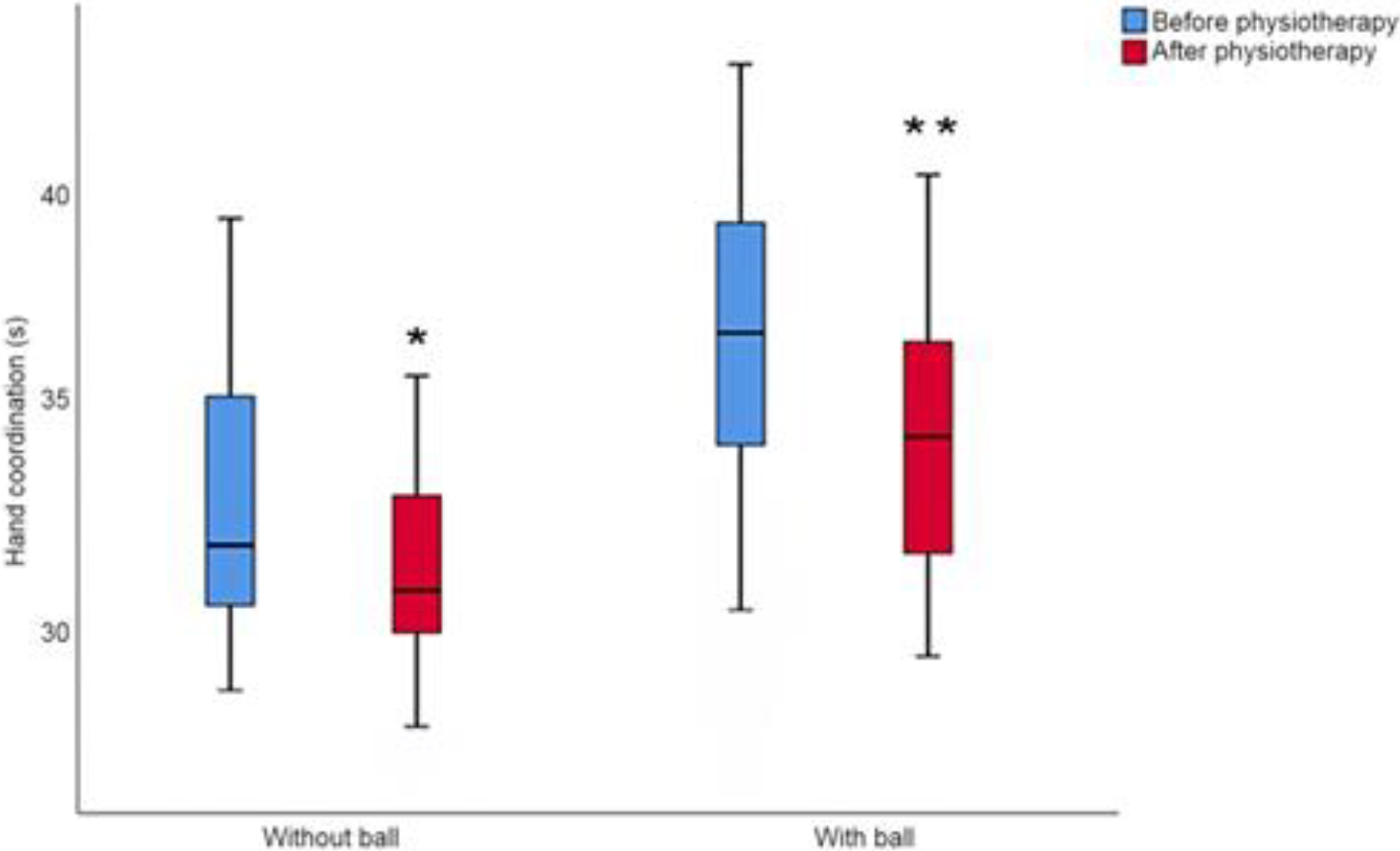
Hand tremor power was calculated using an accelerometer embedded in a mobile phone. This is a common method for rest tremor assessment in PD [23]. Specialized mobile application “Steady Hands” was used for this purpose. The software logs accelerometer data in all three-movement axis and calculates spectral power estimates using a fast Fourier transform – a common method to decode signal into frequency components and their corresponding amplitudes [8, 15, 24]. Acceleration recording time was set to
During the measurements, the subjects were seated, with their hands placed comfortably on the table, and the mobile phones held gently in their palms. Patients were asked not to make any voluntary movements during the data collection. This evaluation was performed separately for each hand immediately before and after the interventions.
Quantitative data were summarized with descriptive statistics: median (Md), minimum value (min), maximum value (max), and mean (A.M.). Mann-Whitney U test was used to compare differences between two independent groups for not normally distributed data. Also, Wilcoxon signed-rank test to compare two sets of scores that come from the same participants for not normally distributed data. In this work statistical significance level of
Results
Assessment of hand coordination
In the control group, the right-hand coordination improved significantly after intervention: Md 29.66 sec at baseline vs. Md 28.05 sec post-intervention. In the experimental group the right-hand coordination improved significantly from Md 30.29 sec at baseline vs. Md 29.54 sec post intervention. There were no significant differences in right-hand coordination between the groups at baseline (U
Right hand tremor power data
Right hand tremor power data
Right-hand tremor power at baseline and after the interventions. *Statistically significant difference in comparing the left arm index in the control group before and after the procedure (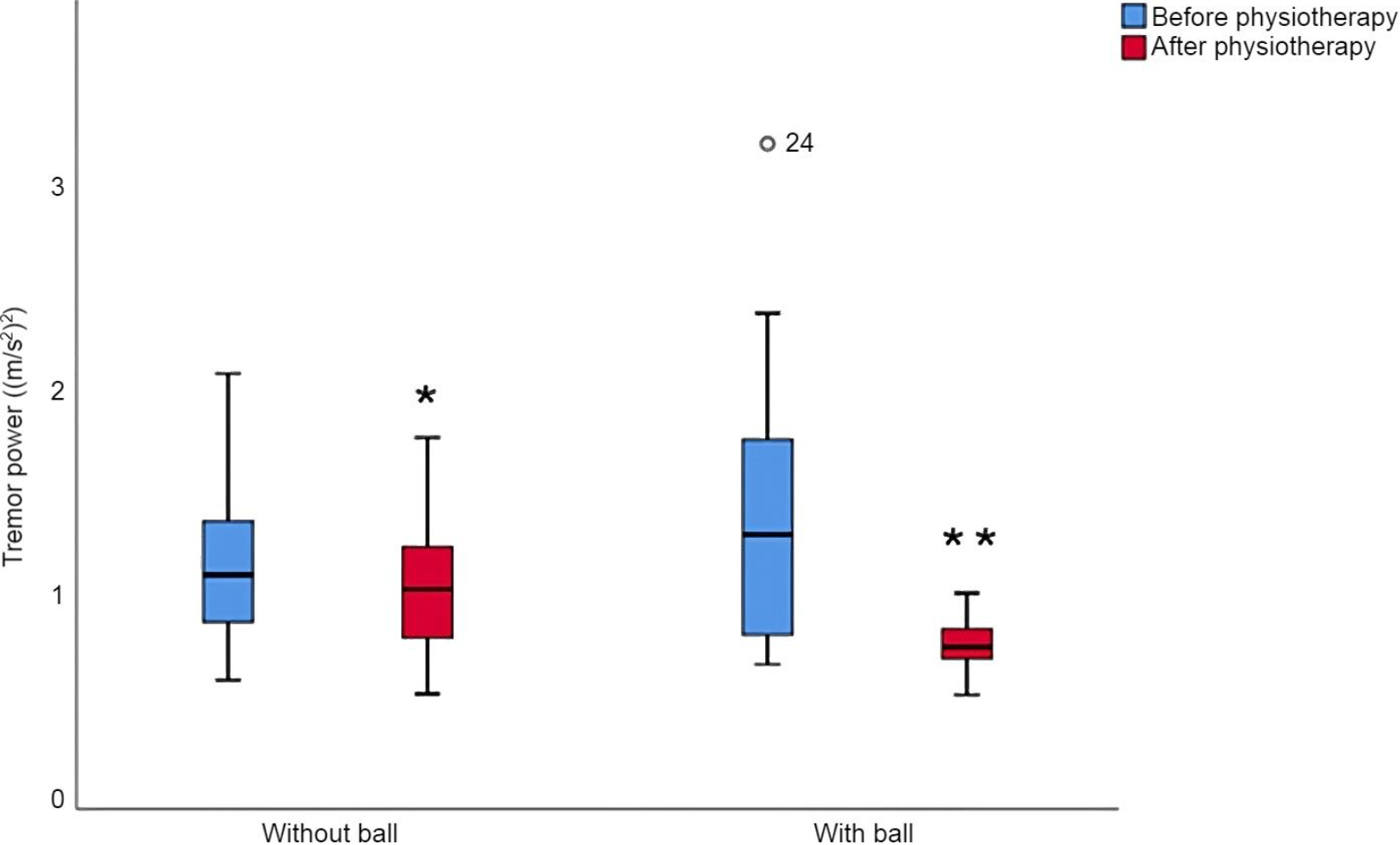
Left hand tremor power before and after physiotherapy. *Statistically significant difference when comparing left hand index in experimental group before and after the procedure (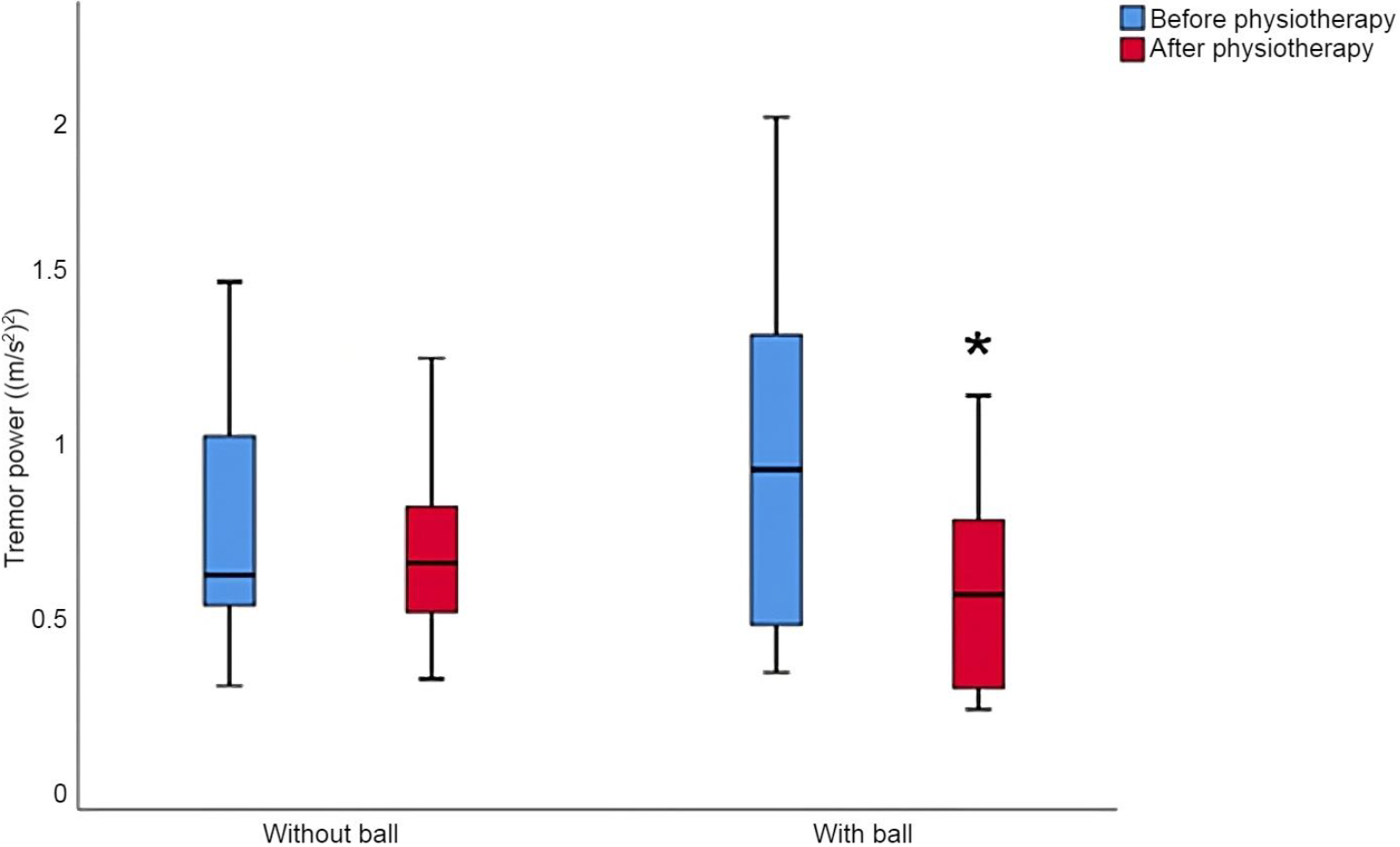
In the control group the left arm coordination improved significantly after intervention: Md 32.29 sec at baseline vs. Md 31.05 sec post intervention. In the experimental group the left arm coordination improved significantly after intervention: Md 36.33 sec at baseline vs. 34.35 sec. after. There were no significant differences in left-hand coordination between the groups at baseline (U
Left hand tremor power data
Right arm muscle strength data
Grip strength in the right hand before and after physiotherapy.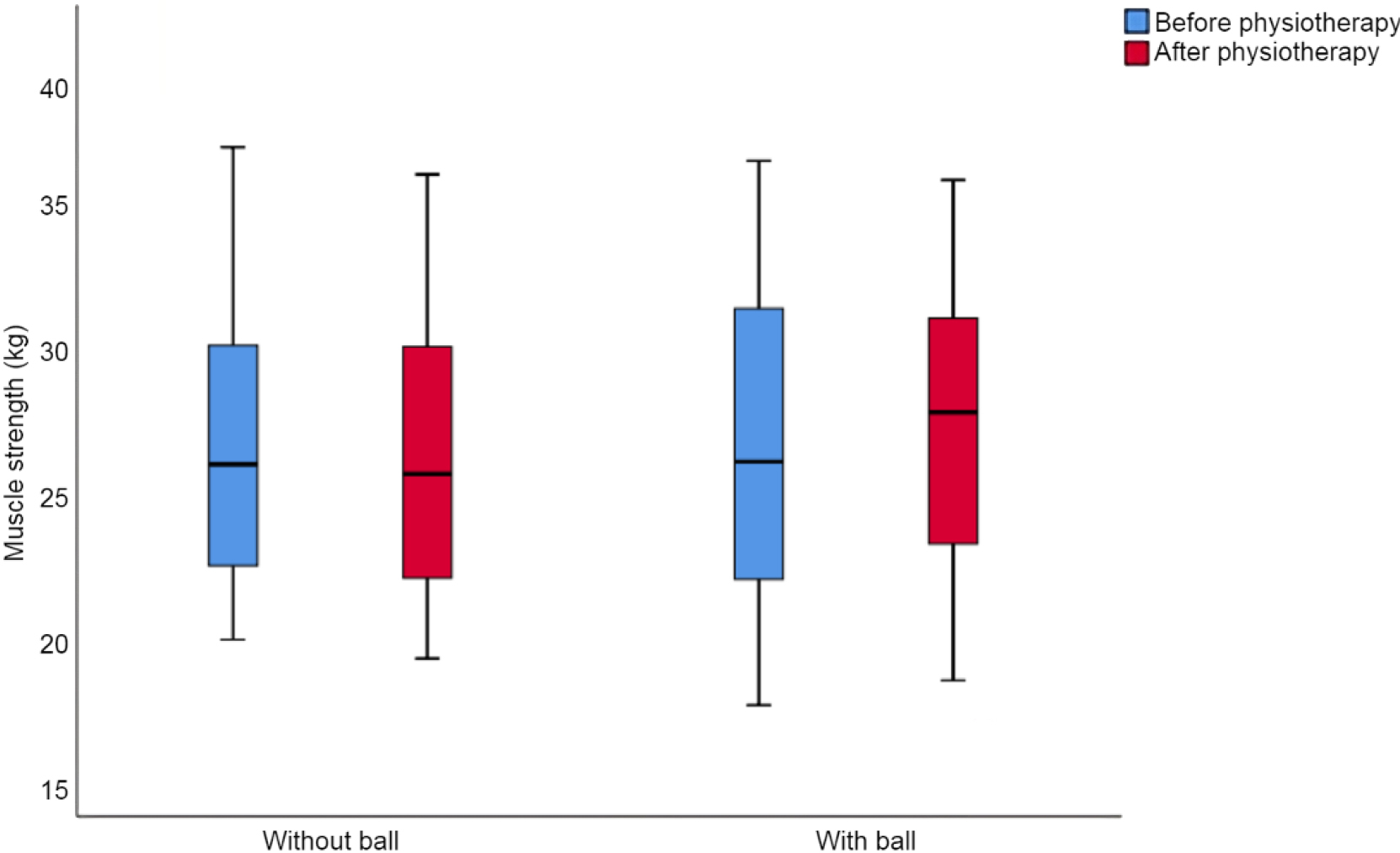
In the control group the right-hand tremor power decreased from Md 1.135 (m/s2)^2 to 1.051 (m/s2)2.
In the experimental group the right-hand tremor power decreased significantly after the intervention from Md 1.372 (m/s2)^2 to Md 0.712 (m/s2)^2. The tremor power did not differ significantly between the groups either before (U
Left-arm tremor power in the “control group was similar before and after the intervention: Md 0.612 (m/s2)^2 at baseline vs. Md 0.635 (m/s2)^2 after. On the other hand, significant decrease in tremor power after the intervention was found in the experimental group”: 0.821 (m/s2)^2 at baseline vs. 0.573 (m/s2)^2 after. There was no statistically significant difference between the groups before (U
Dynamometry
The right-hand grip strength for the control group did not change significantly after intervention: at baseline 27.00 kg (min 20.60; max 38.60; A.M. 27.69) vs. 26.65 kg (min 19.9; 37.6; 27.65) kg after. Also, no change in right-hand grip strength after the intervention was observed in the experimental group: at baseline 27.10 kg (min 18.20, max 38.10, A.M. 27.50) kg vs. 28.90 kg (min 19.10, max 37.40, A.M. 28.12) post-intervention. There were no statistically significant differences between the groups before or post-intervention: U 71.50,
Discussion
The study showed that the VILIM ball local hand-arm vibration therapy in conjunction to physiotherapy can reduce tremor power for PD patients. The experimental group results showed an average tremor power decrease of 48.11% for the right hand and 30.23% decrease for the left hand. At the same time, tremor power in the control group was reduced by 7.38% for the right hand and 3.89% for the left hand. In previous studies it was shown that similarly measured tremor power correlates with traditional tremor rating scales [24]. Therefore, results suggests that patients may benefit more from using physiotherapy and VILIM ball rather than physiotherapy alone. On the other hand, the tremor power between control and experimental groups did not differ significantly before and after the interventions. This may reflect variable response to local arm-hand vibration therapy between patients, and, the need for a larger sample size.
In order to put these results into context, tremor power reduction can be compared to a TAPS study on PD patients hat measured reduction in postural tremor power using accelerometer data. It was concluded that TAPS reduced postural tremor power by a median of 66% (
This study showed that VILIM ball in conjunction to physiotherapy can improve hand coordination. However, the difference of improvement was negligible compared to that of a control group. In the control group, the right-hand coordination improved by 5.74%, left-hand by 3.99%. Meanwhile, experimental group showed 2.54% improvement for the right hand and 5.76% for the left hand. Therefore, study did not provide any evidence that the combination of VILIM ball therapy and physiotherapy provides benefit compared to physiotherapy alone. No significant change in right hand grip strength was detected in neither group.
This study showed that local hand-arm mechanical vibrations generated by the VILIM ball device can be used in combination to physiotherapy to reduce hand tremor power. These findings supplement previous study, where it was concluded that vibrational therapy alleviates symptoms of PD tremor in some patients. Even though the tremor reduction is was shown to be temporary, at some certain cases it may help to improve quality of life [13].
Conclusions
Local hand-arm vibration therapy with VILIM ball in conjunction to physiotherapy can be effectively used to improve hand coordination and reduce tremor power for PD patients. Nevertheless, the study findings did not demonstrate any significant advantages of this treatment in improving grip strength.
Author contributions
Conceptualization, E.L. and E.R..; methodology, E.L., E.R. and M.V.; formal analysis, E.R..; investigation, E.R..; resources, E.L. ,M.V..; data curation, E.L., E.R..; writing – original draft preparation, E.R., A.V..; writing – review and editing, A.T, E.S., S.A..; visualization, E.R..; supervision, M.V., E.LAll authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Ethical statements
The permission from the Bioethics Centre for the research at Kaunas Dainava Polyclinic was obtained (BEC-SR(M)-53).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study.
Data Availability Statement: No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Footnotes
Conflict of interest
Dr. Mantas Venslauskas is the CEO of VILIMED company.