
Abstract
This case report details the complex case of an adolescent patient with chondroblastic osteosarcoma in the setting of Li-Fraumeni syndrome, leading to hemipelvectomy and post-operative complications. International Classification of Functioning principles were used as a roadmap for optimization of functional restoration and transition of care coordination.
Introduction
Li-Fraumeni syndrome (LFS) is a rare inherited autosomal dominant cancer predisposition syndrome secondary to a germline TP53 mutation [1, 2]. Osteosarcoma, soft tissue sarcoma, premenopausal breast cancer, brain tumors, leukemia, and adrenal cortical carcinoma are considered components of LFS cancers [1]. Hemipelvectomy is often considered the treatment of choice for advanced pelvic tumors that cannot be adequately addressed by limb-sparing techniques [3]. Hemipelvectomies often require long-term medical and rehabilitation care before and after amputation. Limb amputation can present with unique functional, emotional, and social challenges, especially in childhood and adolescence due to increased peer pressure [4], family dynamics, and rapidly growing bodies. Recent advances in medical and surgical management of pediatric malignancies including cancerous bone tumors require a transdisciplinary approach in addressing physical, social, and emotional consequences of childhood cancer survivors [5]. However, there is a paucity of literature on the principles of rehabilitative management of adolescents with a rare genetic mutation leading to amputation. In this complex case following hemipelvectomy in an adolescent with LFS, the World Health Organization’s (WHO) International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) principles [5, 6] were applied as a roadmap for optimization of functional restoration and transition of care coordination.
Case history
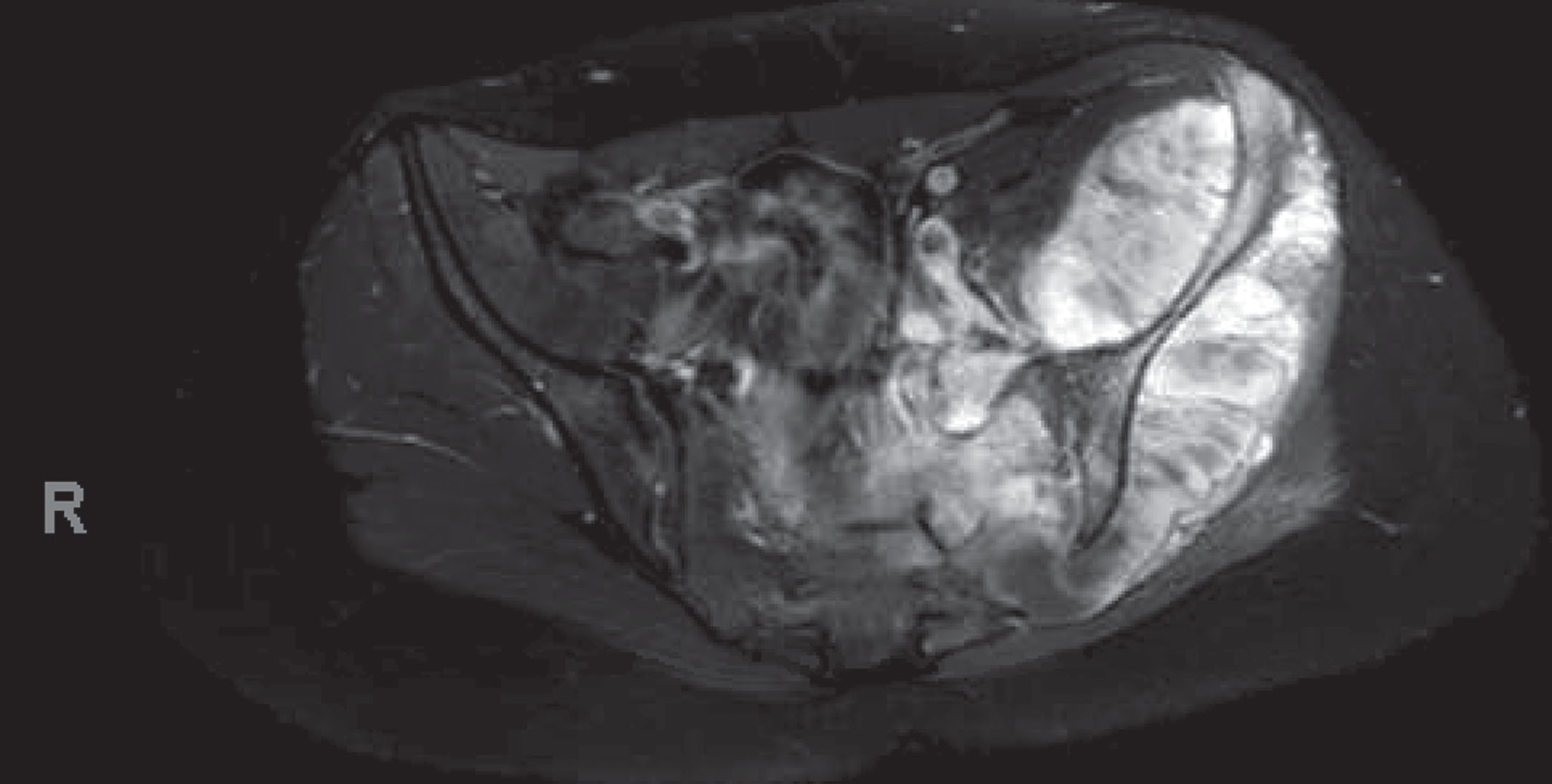
The patient was an 18-year-old adolescent with a history of anxiety and depression who initially presented to an outpatient clinic with progressive low back and left hip pain with ambulation. The pain radiated from buttock to foot and was associated with paresthesia, requiring use of crutches for ambulation. The patient underwent magnetic resonance imaging (MRI) of the pelvis, which showed a mass. Care was delayed due to insurance limitations and a complex psychosocial situation in which she had a difficult relationship with her parents. The patient continued to experience symptoms and eventually presented to the emergency department with intractable pain. A repeat MRI of the pelvis (Image 1) showed a large 15 cm enhancing mass centered around the left iliac wing, sacroiliac joint, and surrounding muscles with extension into the sacrum, left neural foramina, and central canal. The patient underwent image-guided biopsy, demonstrating chondroblastic osteosarcoma with immunohistrochemical (IHC)+for special AT-rich sequence binding protein 2 (SATB2), revealing the disease to be localized to the pelvis and sacrum. Cancer whole exome sequencing also revealed germline p53 mutation, consistent with LFS. Computed tomography imaging demonstrated left common iliac vein thrombosis extending into the external and internal iliac veins. The patient subsequently completed two cycles of cisplatin/doxorubicin followed by treatment with methotrexate without appreciable change in the size of the tumor. During these treatments, the patient had several hospitalizations for symptom control for emesis, pain, depression, and malnutrition. Along the way, she had complex emotional and social incidents, requiring multiple extensive family meetings with the Oncology and Oncologic Orthopedics teams. Eventually, she underwent left hemipelvectomy and sacrectomy for tumor resection with left iliac artery/vein repair, inferior vena cava filter placement, thecal sac transection with exposed L5-S1 and flap closure, and partial right posterior superior iliac spine resection. Post-operatively, the patient exhibited right lower extremity weakness in the setting of lumbopelvic discontinuity. The patient then underwent L3-ilium posterior spinal fusion and pelvic reconstruction with right fibula allograft bone. The post-operative course was further complicated by neurogenic bowel and bladder dysfunction secondary to spinal cord injury caused by necessary sacrifice of all nerve roots below L5. Physiatry was consulted to navigate complex multidisciplinary therapy interventions and care coordination with other specialties including Pediatrics, Neurosurgery, Orthopedic Surgery, Psychiatry, Palliative Care, Pain Management, Infectious Disease, and Oncology to maximize functional independence. However, this only occurred when the patient was three days post-operative. By that point, the patient was limited by uncontrolled left pelvic and phantom limb pain, prolonged immobility of the right lower extremity, and generalized deconditioning in addition to her pre-existing psychosocial difficulties. The patient was able to participate in bedside physical and occupational therapy for generalized strengthening, balance training, and phantom limb pain reduction sensory feedback. This was accomplished with improved pain control through a multimodal approach, including pharmacological treatment by Pain Management and Pediatric Palliative services and psychological support by the Psychiatry service. She was able to perform bed mobility with supervision and transfer bed to chair via pop-over transfer, which uses momentum to pop from one seat to another, with close supervision. The patient was also able to propel a manual wheelchair 1000 ft and demonstrated independence in activities of daily living including management of neurogenic bowel and bladder and after nearly two months was discharged home with family to continue outpatient treatment. She required no new equipment as she already owned a shower chair, rolling walker, and manual wheelchair prior to hospitalization.
Pelvis MRI.
Limb amputation in a setting of surgical intervention falls into two categories: those that are secondary to traumatic injury and those that are due to biological factors, including congenital limb deformity as well as diseases such as cancer [4]. Limb amputation during childhood and adolescence can result in several long-term physical and emotional hurdles while developing socially and physically. From a functional and physical standpoint, limb amputation leads to an irreversible change in the child’s ability to ambulate, touch, play, and interact with their surroundings compared to other unaffected peers [4]. Emotionally, the visible changes after the loss of a limb and the fear of stigmatization from social groups can result in significant stressors in a child’s life as acceptance into peer groups becomes extremely important [4]. Pediatric rehabilitation is an important component in both pre- and post-procedural care in improving functional, emotional, and social outcomes in children and adolescents with limb amputation as part of cancer treatment [4, 7]. In particular, preparatory interventions play a vital role in reducing long-term distress and complications post-operatively, leading to the overall success of adjustment and participation in rehabilitation after the procedure [4]. In this case, the patient and her family were prepared by discussing the surgical plan and necessary post-operative treatment, as well as being assisted with obtaining second opinions at other institutions so they could decide on the plan that returned this patient to her best possible functionality. As an amputation in cancer treatment is not an unanticipated event, the preparation becomes critically important for the medical team [4]. To formulate an overall comprehensive rehabilitation approach achieved by multi- and interdisciplinary teams, adherence to WHO principles [8] can be very helpful to facilitate comprehensive rehabilitation care with input from a multidisciplinary team. These principles are essential when treating medically complex patients such as the patient in this case pre-/post-surgery as well as during all aspects of care delivery [9]. The ICF-CY is designed to provide a common language and framework for human health and function and is organized in two parts, each with two components [9]:
Part 1: Functioning and Disability body functions and structures activities and participation
Part 2: Contextual Factors environmental factors personal factors
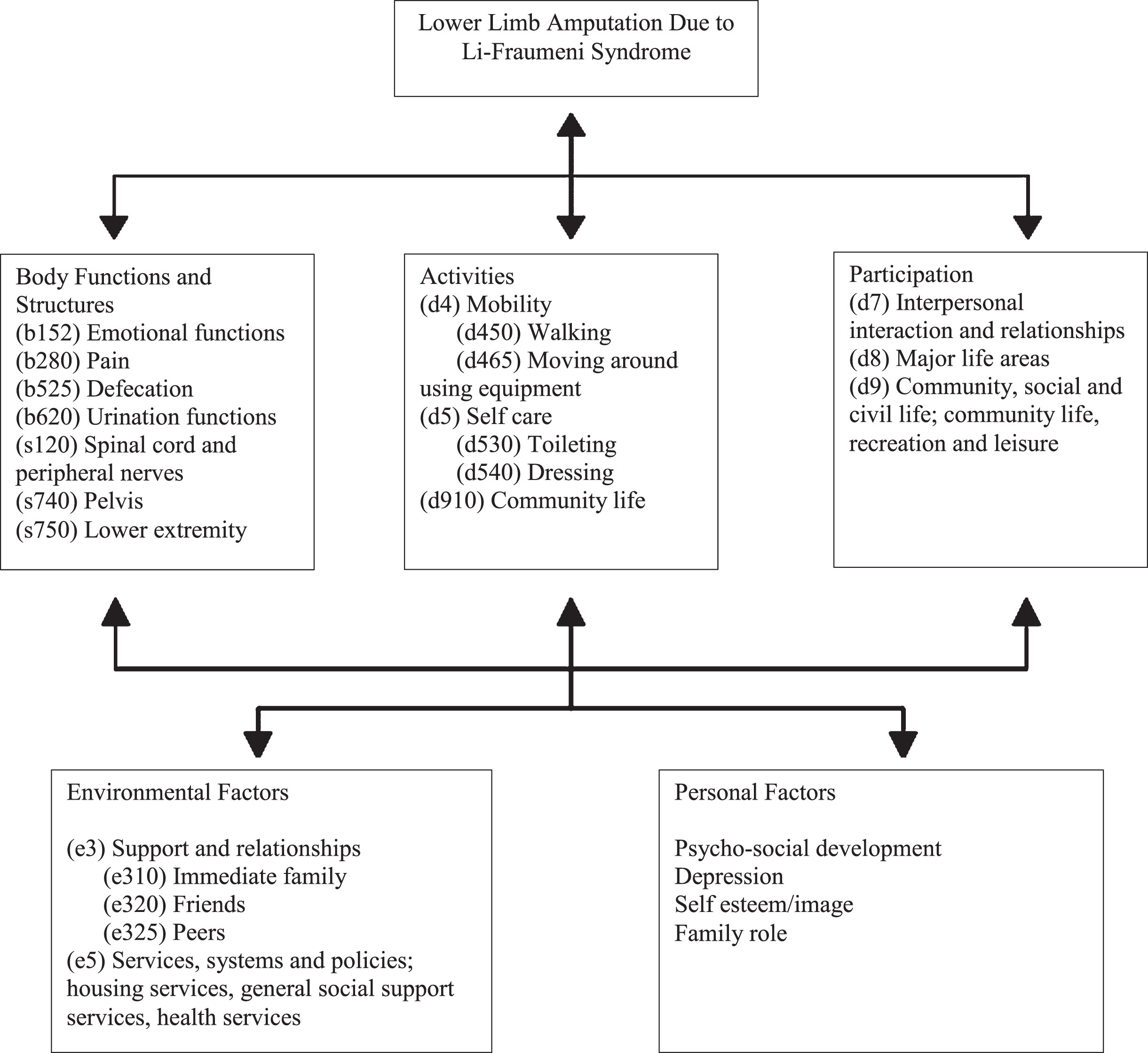
Figure 1, which was specifically developed for this patient case based on WHO principles [8], illustrates the ICF-CY model of functioning and disability of pre- and post-amputation care in an adolescent with a rare cancer predisposing genetic disease. This model allowed the medical team to provide the best care, which is often a dynamic process at various stages of medical care, in timely fashion. For instance, given prolonged hospitalization, the patient was tired of hospitalization and psychologically drained, and most importantly was desperate to be with her family. However, there were significant environmental barriers making discharge unsafe. Thus, the priority was shifted to address environmental and psychological factors, allowing the patient to be discharged home to be with her family in a fully functional way, safely and as quickly as possible.
Model of Functioning and Disability for Lower Limb Amputation Based on the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY).
Acute care teams often focus on the function of the individual body systems that allow compatibility with life. In this patient’s case, her cancer interfered with her life potential, requiring amputation to prolong her life, which inadvertently compromised her functions, including her muscle power/endurance, mobility, and gait pattern. Had physiatry been consulted pre-amputation, these functional areas could have been addressed sooner and with better planning given her complex psychosocial situation. This would have enabled the patient and her family to make a fully educated decision on what life would be in all functional areas after such a drastic amputation and would have better prepared them for the rehabilitation process.
The ICF-CY model allows for a holistic approach that intertwines medical care from each discipline, leading to this dynamic process. The WHO outlines the following five principles of rehabilitation: Body Functions and Structures, Activities, Participation, Environmental Factors, and Personal Factors. The ICF categorizes health and health-related states, therefore requiring the assignment of a series of codes that best describe the profile of the patient’s function. Understanding the usefulness of the ICF will allow clinicians not only to standardize rehabilitation protocols for youth with amputation but also to compare outcomes nationally and globally to provide better patient care.
The number of childhood cancer survivors increases with rapid progress in multimodal cancer therapy. In the United States, approximately 12,400 children and adolescents younger than 20 years old are diagnosed with cancer each year. The current overall survival rate for childhood malignancies is estimated at 79% [10]. However, due to a variety of physical and psychosocial complications from cancer and its treatment, childhood cancer survivors are predisposed to excess morbidity and early mortality compared to the general population [10]. This case highlights the importance of ensuring a smooth transition from pediatric to adult-oriented health care services, not only as a cancer survivor, but also as an amputee with great rehabilitation needs, which can largely depend on a successful pre-transition plan. More importantly, it is essential to keep ongoing two-way conversations among multidisciplinary teams to benefit the patient’s longevity and improve the quality of medical care and rehabilitation interventions during transition of care from inpatient to outpatient settings and from pediatric to adult services. This patient’s transition from pediatric to adult rehabilitation was arranged so that the attending pediatric physiatry consult would continue to follow her and provide assistance during her inpatient adult rehabilitation stay. Unfortunately, the patient preferred to be discharged home, so the transition never occurred.
Comprehensive and consistent use of ICF principles is essential for medical and rehabilitative care, providing a fundamental framework and point of reference for interdisciplinary healthcare practitioners as well as patients and their family members to speak in a common language at the time of complex care delivery and transition from pediatric to adult care. The use of ICF-CY principles for the rehabilitation process allows a multidisciplinary rehabilitation team to structure a complete rehabilitation program to benefit patients, and thus should be implemented in all stages of medical and rehabilitation care of these patients.
Pediatric physiatrists should be consulted as early as possible even in the pre-surgical planning stage, as with any elective amputation, for the purpose of the initiation of ICF principles. This permits multidisciplinary teams treating an adolescent with complex medical conditions including rare forms of bone cancers to establish a common language in reference to functional abilities, to optimize functional restoration, and to coordinate transitions of care. While a physiatrist may be the team member most equipped to introduce, incorporate, and possibly lead this process, ICF principles should be adapted and applied by the whole medial team for better patient care. A goal-oriented approach with the whole person is the ideal treatment option for these complex patients, as illustrated by this case.
Footnotes
Acknowledgments
We thank the patient’s pediatric rehabilitation team for their dedicated care of this adolescent.
Conflict of interest
Competing interests – None; Funding or grants or equipment provided for the project from any source – None; Financial benefits to the authors – None; Details of any previous presentation of the research, manuscript, or abstract in any form – None.
Ethical considerations
This report, as a case report, is exempt from Institutional Review Board approval. Informed consent, however, was obtained from the next of kin.