
Abstract
PURPOSE:
The purpose of this study was to evaluate the effectiveness of intrathecal morphine following selective dorsal rhizotomy in pediatric patients previously diagnosed with cerebral palsy.
METHODS:
This was a retrospective, cohort analysis over the course of four years. The analysis consisted of a treatment group which received intrathecal morphine (5 mcg/kg) injection and a control group that did not receive the injection prior to dural closure. All patients underwent multilevel laminectomies for selective dorsal rhizotomy at Akron Children’s Hospital. The effectiveness of the treatment was measured by total dose of hydromorphone administered on patient-controlled analgesia (PCA), number of days on oral narcotics, and cumulative dose of oral narcotic.
RESULTS:
Of the analyzed 15 pediatric patients, seven patients received intrathecal morphine injection while the other eight did not receive the treatment prior to dural closure. There was a difference of 1135 mcg in total PCA dose between the study group (3243 mcg) and the control group (4378 mcg). The total PCA dose based on weight was lower in the study group (163 mcg/kg) than in the control group (171 mcg/kg).
CONCLUSION:
Based on these findings, the administration of intrathecal morphine clinically reduces the opiate need in the first 96 hours post-operatively.
Introduction
Cerebral palsy (CP) is a neuromotor disorder that disrupts normal motor and postural development in children. The prevalence of CP is 1.5 to 3 per 1,000 live births, and it is associated with pre- and post-neonatal causes. Pre-neonatal causes of CP include prematurity, low birthweight, and maternal infections whereas post-neonatal causes include traumatic brain injury or meningitis [1]. The improper development of or damage to the developing brain impacts the child’s ability to perform precise and effective motor functions. Based on clinical findings, CP is generally classified as spastic, dyskinetic, ataxic, or mixed. The severity of symptoms differ on a patient-basis as does the treatment for the condition.
The current treatment for CP includes physical therapy and rehabilitation, orthotic devices, and surgery. Selective dorsal rhizotomy (SDR) is a neurosurgical procedure that treats the spasticity associated with CP. SDR involves separating the dorsal and ventral roots, stimulating the dorsal nerve roots, and monitoring the response from target muscles. The dorsal sensory roots that contribute to pathologic spasticity are severed to reduce muscle tightness/spasticity and increase the chance of ambulation [2]. Studies have shown that the benefits of SDR remain through early adulthood and lower the need for adjunct procedures such as orthopedic surgeries, Botox injections, and physical therapy [3].
Early studies on SDR in children have proven that epidural administration of morphine in the post-operative period allows for better pain control as compared to oral pain medications [4–6]. The more recent use of intrathecal morphine has now allowed for prolonged periods of pain control and less use of narcotics in the immediate post-operative period. Children who undergo SDR experience severe pain post-operatively due to the invasive procedure and nerve root destruction. Traditional postoperative pain control for SDR includes continuous opioid analgesic administration. While patient-controlled analgesia (PCA) has been on the rise since the 1980 s, some studies suggest there is no significant difference in recovery times compared to the traditional nurse-controlled analgesia (NCA) in adult studies [7]. However, PCA has been linked to greater patient satisfaction and less post-operative complications than NCA [8]. Both NCA and PCA are carefully regulated processes and commonly used as post-operative pain control regimes. However, post-operative opioids are associated with nausea, vomiting, central nervous system (CNS) depression, addiction, and misuse [9].
With the ongoing opioid epidemic and efforts to lower post-operative opioid use, physicians have been tasked with finding alternative methods for pain control. In addition to this, there is a growing trend in protocolizing multimodal avenues of enhancing the recovery process after surgery (ERAS). Previous research suggests that intrathecal morphine administration can improve post-operative pain outcomes compared to the standard regimen. In various spinal and orthopedic surgeries, intrathecal morphine administration is associated with less post-operative oral opioid use, shorter duration of hospital stays, and fewer recurrent visits for pain control [10–12]. One study found that post-operative epidural analgesia lowered pain scores more than systemic analgesia for patients who underwent a partial dorsal rhizotomy procedure [13]. Thus far, little research has been performed to identify pain outcomes in pediatric patients undergoing dorsal rhizotomy who have received intrathecal morphine intraoperatively.
In an effort to reduce post-operative intravenous and oral narcotic pain usage, this study followed the transition to using intraoperative intrathecal morphine, modeled after the spinal fusion pathway. This retrospective study evaluated the post-operative narcotic usage in patients who underwent a multi-level laminectomy for SDR in those who received intrathecal morphine intraoperatively compared to those who did not. These data were collected over a four-year period.
Methods
Patient selection
This was a retrospective review of patients who underwent multilevel laminectomies for SDR at a single institution, performed by a single surgeon during the study period of June 1, 2015, and June 30, 2019 (n = 15). Institutional Review Board approval was obtained prior to chart mining and data collection processes. The control group consisted of patients who did not receive intrathecal morphine. Study patients received a dose of 5 mcg/kg of intrathecal morphine given by the surgeon at the time of dural closure.
Data collection
Demographic information was collected by the study investigators through the electronic medical records of all patients who underwent SDR during the study period. These patients were initially captured by a search from Current Procedural Technology (CPT) codes for this procedure (63185, 63190, 63295) through the medical record throughout the specified time period. Once patients were identified, length of stay (LOS, which is expressed by the time on neurosurgery service prior to transition to the inpatient rehabilitation service), days on PCA, number of doses administered, doses of oral narcotic administered during the hospital stay, and doses of other oral narcotics administered while in inpatient rehabilitation were reviewed.
Study variables
Demographic variables, including age, weight, and gender, were collected to test for any significance in differences between the two groups. The variables included in the analysis were time in operating room, extent of surgical exploration (based on level and percentage of roots cut and total amount of narcotic used post-operatively at 96 hours as measured by total dose of hydromorphone administered on PCA), number of days on PCA, cumulative dose of oral narcotics (oxycodone), number of days on oral narcotics, and number of doses taken. Other pain medication including gabapentin, diazepam, and ketorolac that was received within the 96-hour post-operative period was also included within the analysis.
Statistical analysis
To identify any statistical difference between the demographics of the two groups, non- parametric descriptive statistics were used in the analysis. Wilcoxon Rank Sum tests were conducted for age and weight, and Fisher’s exact test was conducted to assess any association with gender.
For the variable analysis, the Wilcoxon Rank Sum test was used to compare outcomes between the study group and the control group by incorporating the variables identified. A p-value<0.05 was used to note any significant difference in variables between the groups.
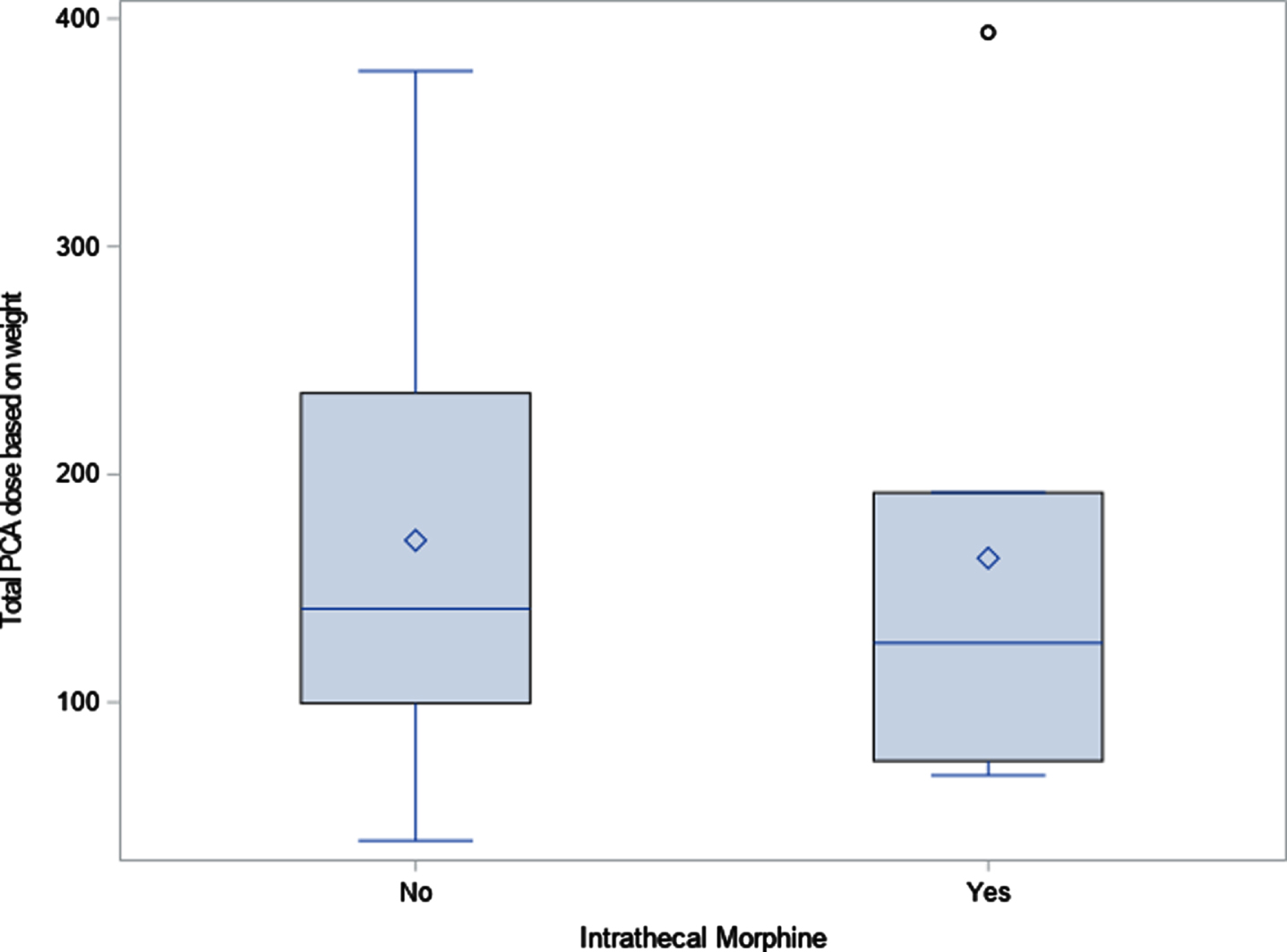
PCA dose based on weight. Diamond indicates mean; line indicates median. PCA: patient-controlled analgesia.
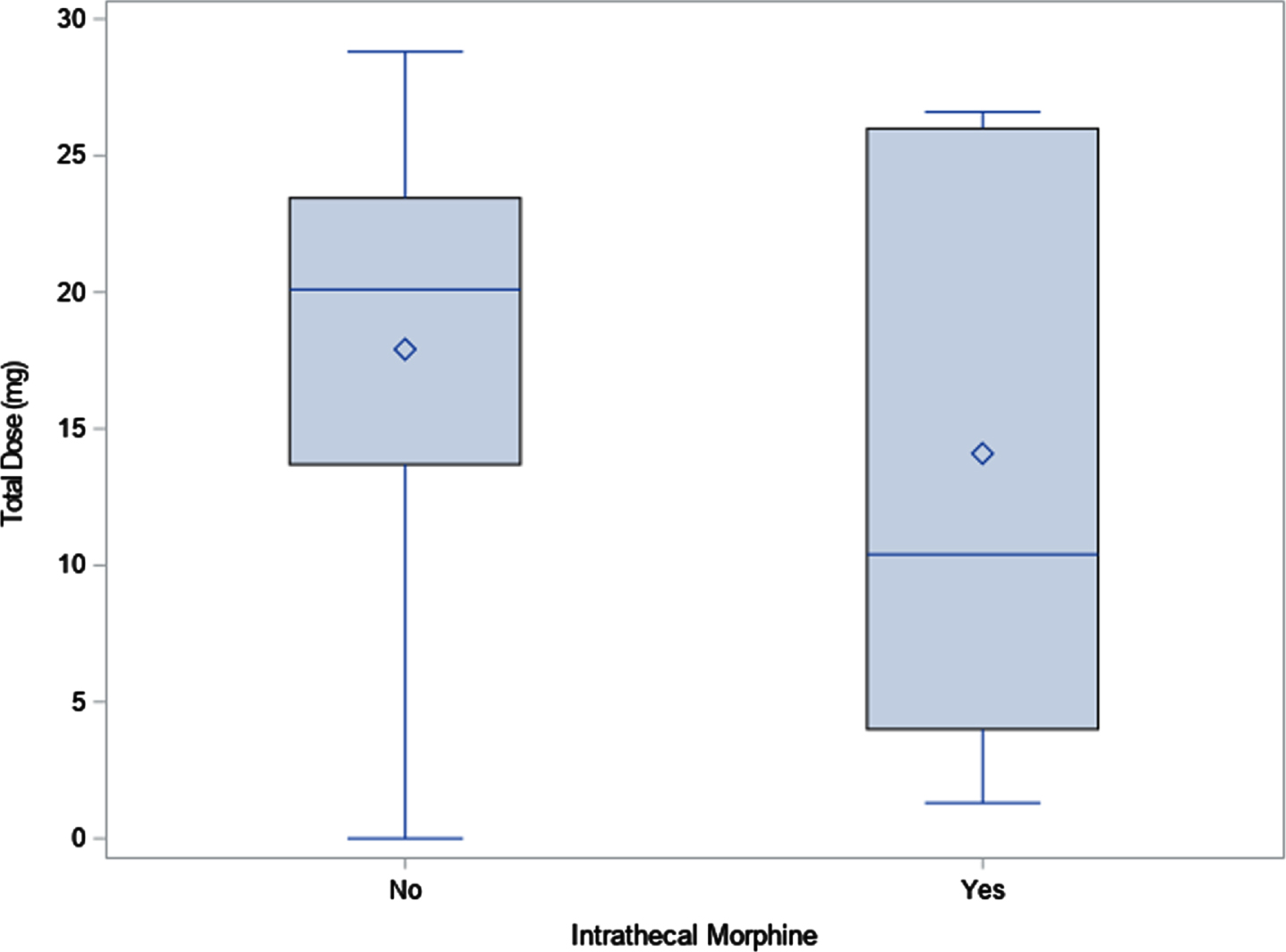
Total dose of narcotic. Diamond indicates mean; line indicates median.
The surgical technique used at the institution follows the Peacock technique using multilevel laminectomy for bony exposure, typically levels L2–L5 [14]. All patients underwent the same technique performed by the same surgeon at a single institution. Laminectomies were performed from L2–L5 using an ultrasonic bone scalpel. Using intraoperative neuromonitoring and concurrent functional exam, each level from L2 through S1 was worked through systematically. Sensory nerve rootlets were selected and isolated while motor nerves were protected. If there was an abnormal electrical or motor response, the rootlet was cut. Per side, 20–40% of rootlets per level were targeted. For the cohort group, intrathecal morphine at 5 mcg/kg was injected into the subarachnoid space just prior to tying the last dural stitch. Patients were then kept flat for 48 hours, allowing for prone, supine, or lateral positioning. On post-operative day two, patients were allowed to sit up and start to mobilize with the help of physical therapy.
Results
Fifteen patients were identified between the study period of June 2015 through July 2019 who met the inclusion criteria. Seven patients received intrathecal morphine, and eight patients did not receive intrathecal morphine intraoperatively. The group demographics between the study group and the control group did not show any statistical significance with regard to gender, age at time of surgery, or weight at time of surgery. Incidentally, 75% of the control group were female as compared to only 29% of the study group (Table 1).
Baseline demographics
Baseline demographics
Total PCA dose (and weight-based dose) over 96 hours was used to maintain consistency across all patients in the study as all patients remained on either the neurosurgery service or inpatient rehabilitation service during the time period and data were accessible. Although the patient might have changed services prior to 96 hours, they remained in the same bed and on the same unit with the same providers, so protocols remained consistent throughout the study period. While results did not achieve statistical significance, a trend of less narcotic use in total was noted in the cohort group when compared to the control group. As an example, the total PCA dose for the study group was 3243 mcg while the total for the control group was 4378 mcg, a difference of 1135 mcg. The same tendency was seen in weight-based dosing as well: 163 mcg/kg in the study group vs. 171 mcg/kg in the control group. Although the mean total number of days on oral narcotics was greater in the study group (2.6) vs. the control group (1.8), the total oral narcotic dose was greater in the control group (17.9 mg) vs. the study group (14.1 mg). An even greater difference was seen when examining the median value for this measure, with 20.1 mg in the control group and 10.4 mg in the study group (Table 2).
Outcomes: Ordered observations by intrathecal morphine groups
OR: operating room; PCA: patient-controlled analgesia.
At the study institution, ketorolac is commonly given after 12 hours from surgery, barring any contraindication. The median amount of ketorolac given during the first 96 hours post-operatively was 34.4 mg in the control group and 14.4 mg in the study group. Another measure that revealed an inverse relationship was the total dose of gabapentin within the first 96 hours post-operatively with 605.6 mg in the control group and 804.3 mg in the study group.
Based on the data, it was shown that the use of intrathecal morphine intraoperatively clinically reduced the opiate need in the first 96 hours post-operatively. Although the data did not show statistical significance amongst the variables selected, there did appear to be a tendency to have less overall narcotic use when intrathecal morphine was given in the operating room. This confirmed data from prior studies showing that the use of intrathecal morphine lessens the need for post-operative narcotics in the immediate post-operative period [15, 16]. Other positive outcomes from this study included less total dose of oral narcotics, less total dose of diazepam, and less total dose of ketorolac in the immediate post-operative period.
The inclusion of gabapentin, started the day of surgery as part of the ERAS effort, may have also contributed to this trend. A study by Pao et al. found that the use of gabapentin along with non-steroidal anti-inflammatory drugs in the perioperative period showed similar pain scores in the post-operative period as compared with patients treated with opioids [17]. Therefore, it cannot be concluded that the decrease in narcotic usage was solely based on the use of intrathecal morphine. It is also recognized that there are modifications to the surgical method that decrease incision length, exposure, and time in the operating room. The single or double laminectomy procedure for SDR is now performed by a partner surgeon, with greater success in post-operative pain management. Further study into the narcotic usage of these patients is yet to be determined at the time of this manuscript.
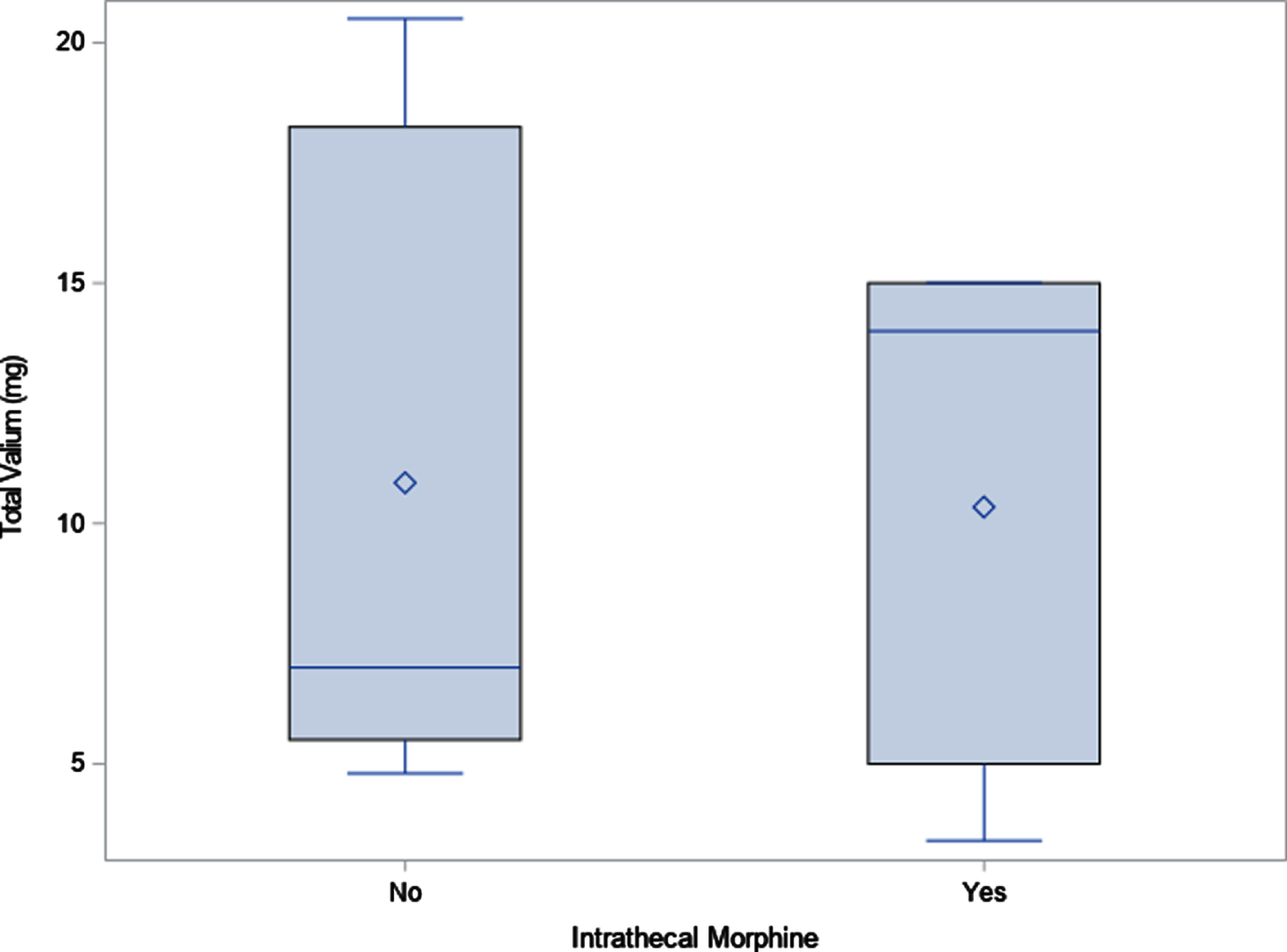
Total valium dose. Diamond indicates mean; line indicates median.
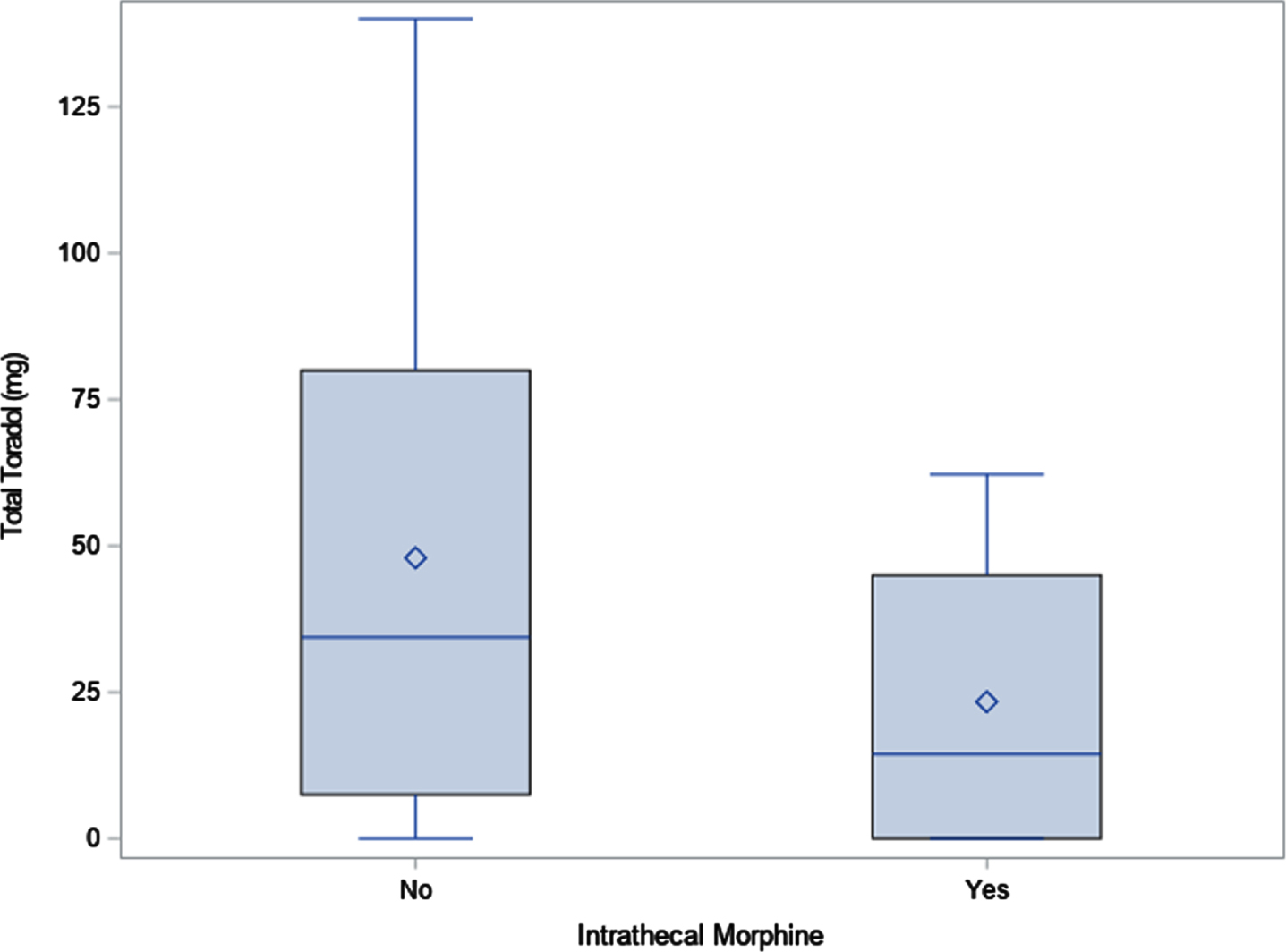
Total ketorolac dose. Diamond indicates mean; line indicates median.
Other limitations include that this was a retrospective cohort analysis with a small population size. The cohort groups were not randomized as the decision to begin using intrathecal morphine on all patients was decided halfway through the study period based on the growing body of literature and success of this procedure. Furthermore, differing measures of pain validation could be used in the future to assess post-operative pain status. These measures could not be used in this study as the data in the chart were not easily accessible for each patient. There were a total of 19 patients who underwent SDR surgery within the study period; however, two were performed by a different surgeon and another two did not have adequate documentation in the medical record to allow for analysis of all outcome variables, so they were not included in the study.
At the study institution, the use of intrathecal morphine has shown some benefits in terms of post-operative pain control for patients undergoing multi-level laminectomy for SDR. Moving forward, a prospective randomized study of SDR patients utilizing the single level laminectomy technique and pre-operative gabapentin, with the protocolized post-operative pathway may show clinically significant results. In the spirit of reducing post-operative narcotic use and enhancing recovery after surgery, the community should consider the utilization of “unconventional” ideas such as long-lasting local anesthetic, nerve blocks, or subcutaneous anesthetic medication administration.
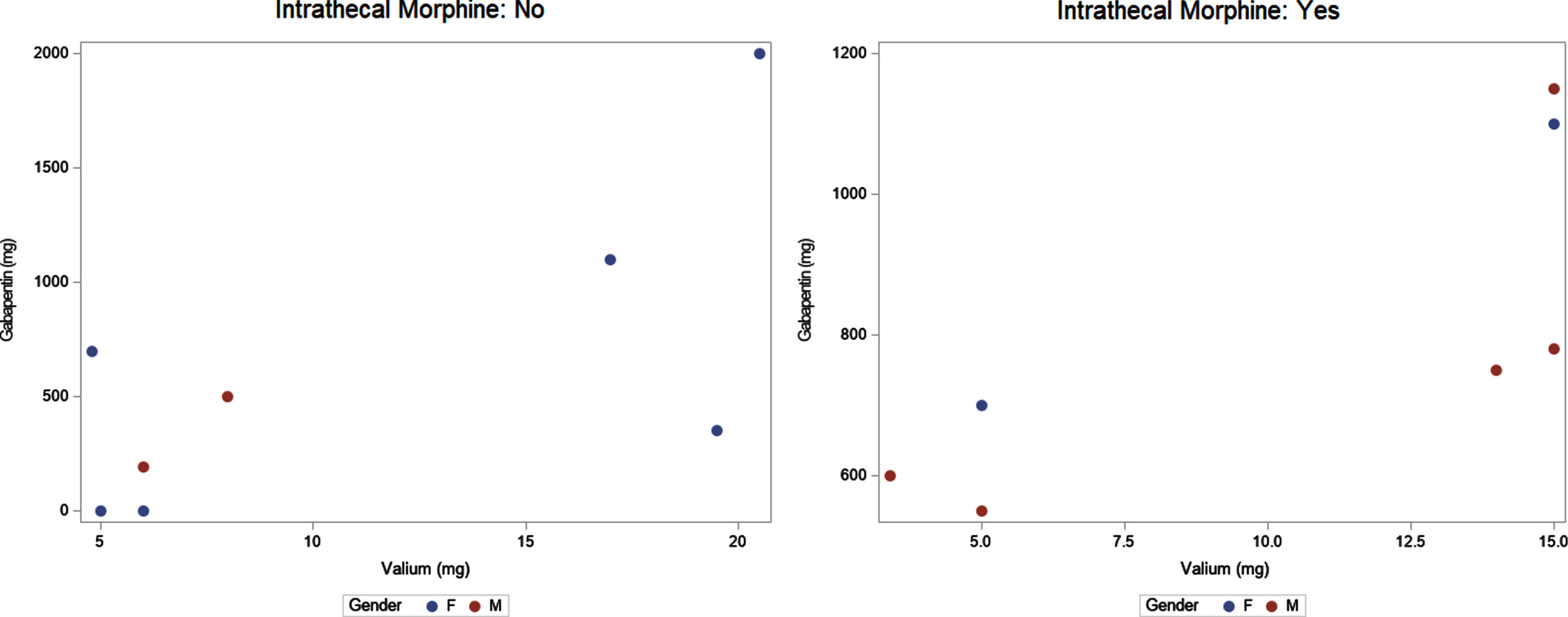
Gabapentin (mg) vs. Valium (mg) by intrathecal morphine and gender.
Conflict of interest
No funding was secured for this research and there are no conflicts of interest for any of the authors.