
Abstract
Selective dorsal rhizotomy (SDR) was used to treat lower extremity spasticity in an ambulatory 7-year-old girl with a history of a T10 spinal lipoma. The spasticity was the result of an AIS D spinal cord injury (SCI) suffered during untethering surgery at age 2 years. After SDR and a course of intensive inpatient rehabilitation, the patient’s gait improved markedly. To the authors’ knowledge, this is the first published case of SDR as a treatment for spasticity in a patient with a spinal lipomatous malformation.
Introduction
Spasticity of the lower extremities typically occurs as a result of an injury to the central nervous system. It is frequently seen in cerebral palsy (CP) and spinal cord injury (SCI). Severe spasticity can negatively impact gait and function, both directly and by causing contractures, thereby worsening independence and quality of life.
Selective dorsal rhizotomy is a surgical intervention that treats muscle spasticity by sectioning abnormal sensory nerve rootlets that innervate the lower extremities. Abnormal sensory rootlets are chosen for sectioning using intraoperative electromyography (EMG) (Fig. 1). It is a well-described treatment for appropriate candidates with CP, and it also has been described as a treatment in patients with SCI, usually of traumatic origin [1–3]. However, to the best of the authors’ knowledge, its use has not been previously described in patients with spasticity resulting from spinal lipomatous malformations or SCI sustained during operations thereon. In this report, the case of a young girl who underwent SDR for spasticity resulting from surgery for a spinal lipoma is described.
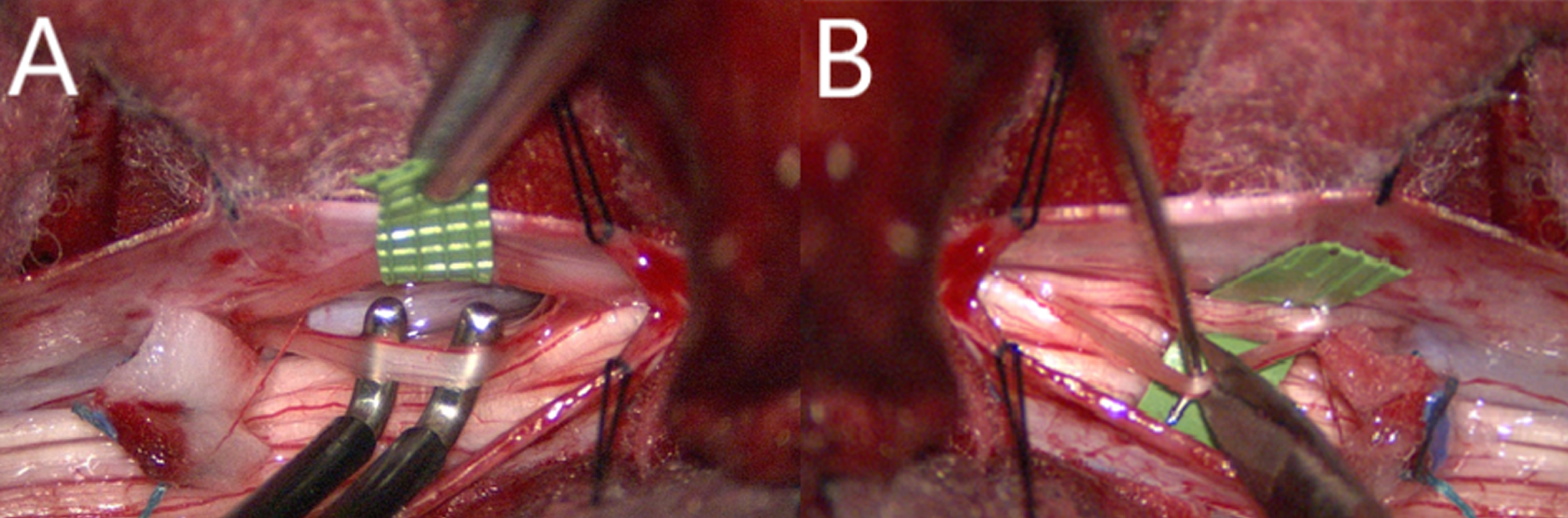
Intraoperative photos. (A) Selectively stimulating nerve root. (B) Sectioning nerve root.
A 7-year-old girl presented to the rhizotomy clinic with lower extremity weakness, spasticity, and gait disturbance. Although she only started to walk with assistance at approximately 18 months of age, her weakness and spasticity first truly became evident after spinal cord untethering and surgical debulking of a T10 lipoma at two years of age at a different institution (a postoperative MRI is shown in Fig. 2). After surgery, she needed intensive physical therapy and was not able to stand again for six months. Onabotulinum toxin A injections to her gastrocnemius muscles and phenol injections to her hamstrings were initially helpful but more recently made little difference. At the time of presentation to the rhizotomy clinic, she had no history of orthopedic surgeries. She continued to take 5 mg oral baclofen at bedtime, received regular physical therapy, was ambulatory with carbon fiber ankle-foot orthoses (AFOs), and required no assistive devices. Also, she had difficulty with higher level motor skills such as running and jumping. She was continent of bladder and bowel, although she had longstanding constipation.
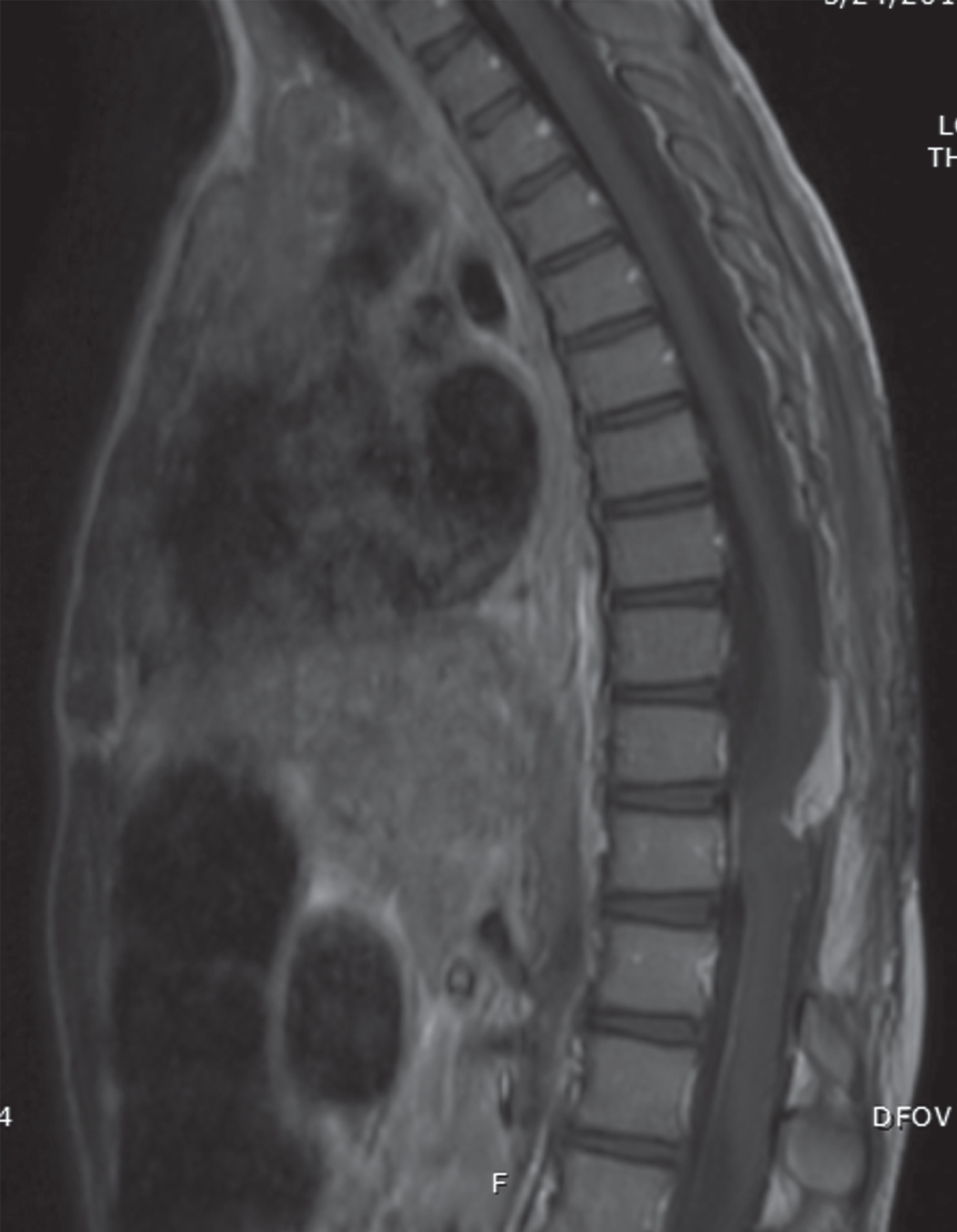
MRI depicting the patient’s residual T10 spinal cord lipoma.
On exam, she had bilateral weakness and spasticity of her lower extremities. Muscle strength was generally 3-4/5 in the iliopsoas and other muscles of her lower extremities (L2 AIS level D) (AIS = American Spinal Cord Injury Association Impairment Scale) (Table 1). Her bilateral patellar and left Achilles reflexes were 3+; she had sustained clonus at her right ankle and had asymmetric sensation in the feet with decreased light touch, temperature, vibration, and joint position sense on the right. She walked with a spastic diparetic gait: crouched with marked scissoring, but only slightly toe-to-toe with minimal internal foot progression angle. Modified Ashworth scores (MAS) were 2 on the left and 1+ on the right in her quadriceps, 3 in her hamstrings bilaterally, and 2 on the left and 3 on the right in her gastrocnemii. She had bilateral mild knee flexion and plantar flexion contractures. Subjective and objective preoperative and postoperative measures can be found in Tables 2 3.
Scale used to grade muscle strength in tested muscle groups [15]
Preoperative and 13-month postoperative gait study subjective assessments
Preoperative and 13-month postoperative gait study objective measures
Partial gait analysis at the Children’s Colorado Center for Gait and Movement Analysis (CGMA) demonstrated bilateral mid-foot strike and spasticity on electromyography (EMG) throughout the gait cycle in all major lower extremity muscles (Fig. 3a; EMG not shown). Barefoot, her self-selected gait speed was 40 m/min. With AFOs, her speed was 54 m/min. A full preoperative or postoperative gait analysis was never performed due to insurance denial; therefore, kinematic and kinetic data were never obtained.
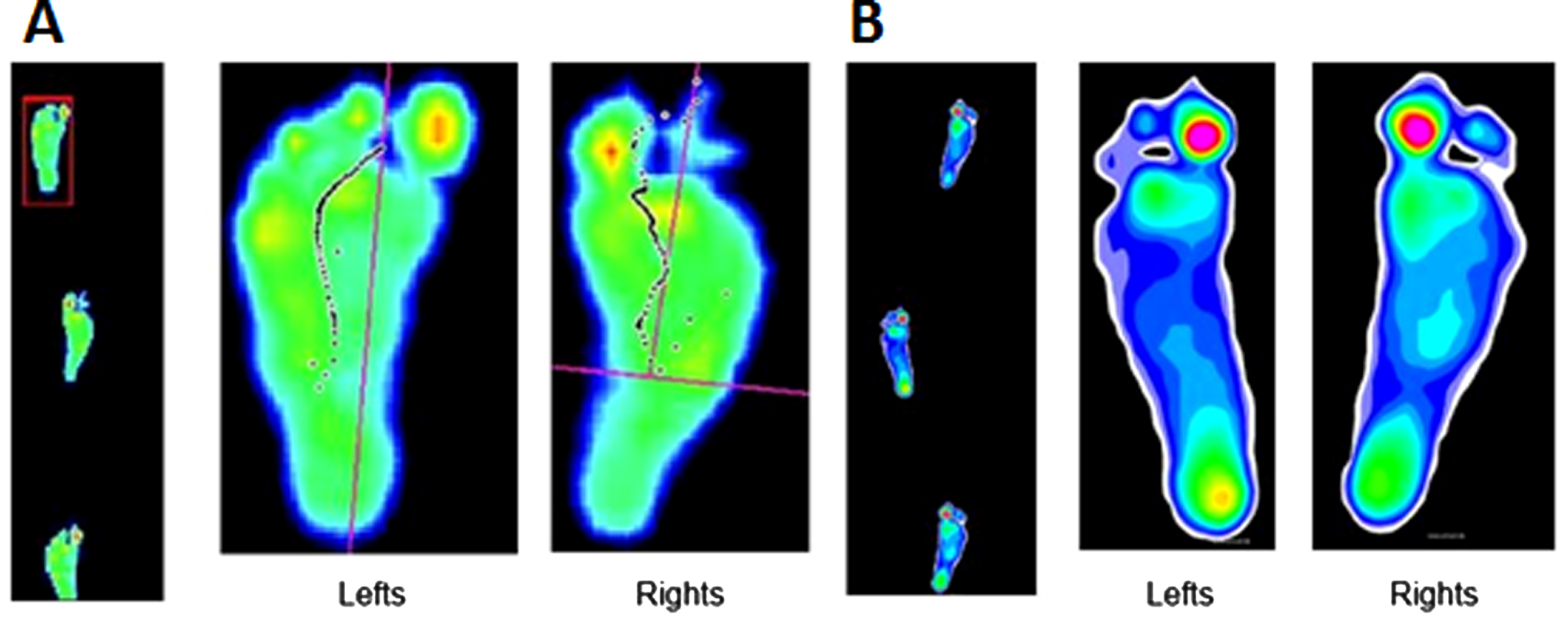
Ambulatory plantar pressure recordings. (A) Preoperative recordings demonstrate bilateral midfoot strike. (B) 13-month postoperative recordings demonstrate bilateral heel strike, more notable on the left.
Due to concerns that her lower extremities might not be strong enough to support her after SDR, the patient underwent an intrathecal baclofen (ITB) test dose and returned to the CGMA for a post-ITB observational video. After the ITB test dose, her lower extremity spasticity decreased, and her strength was maintained. The video showed improved gait after ITB. It was decided to proceed with SDR.
She underwent L1-L5 osteoplastic laminectomy (Fig. 1), replacing the elevated laminae and spinous processes, at the end of the case. After differentiating motor from sensory roots anatomically and by their stimulation threshold and EMG latency, sensory roots were divided into 3–6 rootlets. A suprathreshold 50 Hz stimulus was then applied for 1s. She underwent bilateral sectioning of 40–60% of the dorsal L2-S1 rootlets, sectioning those that produced the most abnormal responses using a combination of Park’s grading system of EMG spread and Peacock’s descriptions of abnormal EMG waveform morphology [4, 5]. Her spasticity was much improved after surgery. There were no complications, including changes in bowel or bladder function. She successfully underwent 5 weeks of postoperative intensive inpatient rehabilitation.
Six months after surgery, she had persistent gastrocnemius tightness and underwent onabotulinum toxin A injections to her bilateral gastrocnemii, followed by serial ankle casting.
Fifteen months post-SDR, her gait was substantially improved with new ability to achieve full knee extension and heel strike bilaterally, and no scissoring or internal foot progression angle. Her balance had improved considerably with new ability to step over objects. She was able to negotiate stairs without holding on to the railing, had improved ability to run and jump, and her endurance was better. Her gait pattern was overall less stiff with reduced circumduction. MAS had improved to 0 in the quadriceps, hamstrings, and gastrocnemii. She had moderate hamstring tightness with popliteal angles of 45 degrees, bilateral full knee extension, and improved ankle dorsiflexion. Her baclofen had been discontinued. She continued to have asymmetric sensation in the feet.
Repeat partial gait analysis at 13 months post-surgery confirmed an improved gait pattern. She had bilateral heel strike, better on the left (Fig. 3b). Gait speed both barefoot and in her AFOs had improved, in her AFOs to 66 m/min. EMG data was not acquired for this analysis due to insurance denial. Tables 2 3 compare preoperative and postoperative gait study subjective and objective measures.
SDR is a well-established procedure for treating lower extremity spasticity in children with CP [6–8]. However, it may also be considered for management of lower extremity spasticity caused by SCI. In reported cases, children with SCI and lower extremity spasticity have experienced significant improvements in their spasticity and motor function [3, 6].
Gump et al. performed SDR on 35 patients with SCI [3]. The authors found a direct relationship between percentage of dorsal root fascicles transected and improvement of symptoms. All 35 patients experienced significant improvement in their gait and quality of life post-SDR. Reynolds et al. reported 3 cases in which patients’ families declined ITB therapy or other treatments for various reasons. SDR led to significantly decreased spasticity in 2 out of the 3 cases. The 3rd patient experienced initial relief but needed other therapies to supplement the SDR [6]. SDR has also been used to treat spasticity caused by other spinal pathologies, such as myelomeningocele [9] and transverse myelitis [10].
This case is the first described in which SDR was used in a patient with a history of spinal lipomatous malformation. It was not clear if her weakness and spasticity were the result of just the surgery to debulk the lipoma or were partially caused by the lipoma itself. However, the fact that it took her half a year to stand again after surgery when she had been walking with assistance before surgery implies that there was injury to the spinal cord as a result of the surgery.
Performing SDR in ambulatory children with substantial lower extremity weakness who rely partially on their tone for support may worsen their ambulatory ability. In such children with CP, often Gross Motor Function Classification System III, a preoperative gait video after ITB injection may be performed. If their tone diminishes while their abilities to ambulate and support themselves remain, it is safer to proceed with SDR. The baclofen is usually injected in the morning under short-acting inhaled anesthesia. A gait video is performed approximately 4 hours after injection. Most patients will have already had a full gait study, with EMG and kinematics, and the full gait study is not repeated. Since the video does not take as long as a full gait study, the Gait Center is able to be flexible in the exact timing of the video and can delay it for an hour or two if the patient is, for instance, too loose at the scheduled video hour. In general, most patients who undergo baclofen test injections receive 40, 50, 60, or 75 mcg, based loosely on weight. Lower doses, 40 or 50 mcg, are more commonly given to patients who will be undergoing gait videos.
SDR is often performed through a shorter osteoplastic laminectomy and stimulate and section nerve rootlets just below the conus medullaris. In this case, a longer osteoplastic laminectomy was chosen to stimulate and section the rootlets just before they exited dura. There was concern about possible asymptomatic recurrent tethering at T10 and thought a lower laminectomy with no manipulation of a potentially tethered conus would be safer.
The patient had no short-term complications of SDR. However, it is unclear whether she has elevated long-term risk of scoliosis, due to her surgery [11]. In patients with CP at least, this risk has never been satisfactorily shown to be higher than the risk in patients who have not undergone SDR [12]. There is a higher-than-expected risk of postoperative spondylolisthesis after SDR [12]. Normally, spine x-rays are obtained one, two, and five years after surgery. The patient has so far had no clinical or radiologic (not shown) evidence of postoperative scoliosis or spondylolisthesis, or recurrent spasticity. While this data is limited by the relatively short follow-up period of 15-months, it is hoped that her ambulatory improvements will be long-lasting. SDR has been shown to lead to durable improvements in gait [13]. While long-term studies are scarce for patients with SCI, SDR has demonstrated a reduction in gross motor decline for adults who had the procedure in childhood, without increasing pain or fatigue [14].
Current issues with SDR include incomplete knowledge about which children with CP-related spasticity do best after SDR and about how well children with spasticity associated with other etiologies respond to SDR. Further research is required to determine the optimal candidates for the procedure. This case is a reminder that SDR can be a viable option for the treatment of severe lower extremity spasticity in patients with SCI due to various causes, including surgery for spinal lipomatous malformations and other entities.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical considerations
Signed informed consent was obtained from the parents and approved by the authors’ Institutional Review Board.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.