
Abstract
PURPOSE:
The purpose of this study was to examine the relationship between early mobility (EM) of pediatric patients mechanically ventilated and functional outcomes in rehabilitation using WeeFIM scores, as well as hospital length of stay (LOS), ICU LOS, and rehabilitation LOS.
METHODS:
A retrospective chart review of 189 patients was completed to compare those who received EM interventions to those who did not in the ICU. Data extracted from the years 2015-2019 included: all patients who were between zero and 21 years, were mechanically ventilated via endotracheal tube (ETT) for > 48 hours, and then transferred to the comprehensive inpatient rehabilitation unit (IRU).
RESULTS:
For respiratory patients, the EM group had higher WeeFIM scores in all categories at admission to IRU compared to the comparison group. Neurosurgery patients had higher cognition and total WeeFIM scores in the EM group at admission to IRU. All diagnoses demonstrated shorter hospital, ICU, and IRU LOS for the comparison group versus the EM group.
CONCLUSION:
EM of mechanically ventilated pediatric patients with a primary respiratory diagnosis demonstrated improved function at admission to IRU compared to those who did not participate in EM. Prospective research needs to be done to examine this relationship further.
Keywords
Introduction
Critically ill patients who are mechanical ventilated in an intensive care unit (ICU) are in a fragile state. Traditionally, standard practice included keeping them on strict bed rest and fully sedated to improve patient comfort, minimize pain, agitation, and anxiety [1]. It has been well established that prolonged bed rest may lead to increased hospital length of stay (LOS) and multiple co-morbidities, including disuse muscle atrophy, joint contractures, ICU acquired weakness [2–4]. The “ICU Liberation” campaign was initiated in 2013 by the Society for Critical Care Medicine and encompasses an ABCDEF bundle, which is a multi-disciplinary effort to improve patient outcomes by optimizing modifiable aspects of their care and environment [5–10]. ABCDEF includes A- Assess and manage pain; B- Breathing; C- Choice of analgesia and sedation; D- Delirium; E- Early mobility (EM); and F- Family engagement [6]. A prospective, multi-center cohort study of over 15,000 adults in an ICU found implementation of the ABCDEF bundle showed significant and clinically meaningful outcomes [11].
Critical care adult studies have demonstrated a positive association of EM with decreased hospital and ICU LOS, decreased ICU-acquired weakness, and improved functional status [12–14]. Compared to the adult body of work, there are fewer studies in the pediatric literature demonstrating benefits of EM in the pediatric intensive care unit (PICU). While authors have concluded that EM in the PICU can be feasible and safe, more research needs to be done to demonstrate a relationship between EM and improved clinical and financial outcomes [15–17]. In two pediatric studies, an association between EM and shorter hospital and PICU LOS was reported [18, 19]. Of note, none of the published pediatric studies looked specifically at the benefits of EM while being mechanically ventilated (MV) in improving functional outcomes such as independence with self-care, bed mobility, walking, etc. Patients who are MV have a perceived increased risk of unplanned extubation while being mobilized because of the insecurity of their airway with an endotracheal tube (ETT). Additionally, developmental level plays an important role in EM in the pediatric population, as the lack of cognitive understanding of younger children to maintain a safe airway when they are awake and moving is a challenge [20].
The purpose of this study was to examine the relationship between EM and hospital LOS, ICU LOS, rehabilitation LOS, and functional outcomes in rehabilitation using WeeFIM scores. It was hypothesized that those who received EM interventions would have a decreased inpatient rehabilitation unit (IRU) LOS, a decreased PICU LOS, and increased WeeFIM scores at admission to the IRU compared to those who did not receive EM interventions.
Methods
Setting and patient sample
This retrospective study was completed in the PICU of Children’s Healthcare of Atlanta, Egleston campus, an academic quaternary care level I trauma medical-surgical unit with more than 3500 admissions per year. Children’s Healthcare of Atlanta has a 28-bed IRU with approximately 400 admissions per year that provides intensive physical, occupational, and speech therapy prior to discharge home.
Data was extracted by the researchers from the electronic medical record from the dates January 1, 2015 to December 31, 2019. Inclusion criteria included: age (zero to 21 years), all genders, race and ethnicity, and MV via ETT for > 48 hours in the PICU, and once stabilized, discharged to IRU. Patients who had a tracheostomy were excluded from this study.
Patients were divided by those who received EM while intubated and those who did not. To be included in the EM group, patients received level 2 or 3 EM interventions by a Physical Therapist (PT) and/or Occupational Therapist (OT) while they were intubated. Levels of mobility were defined as follows: 1) Level 1 was any therapy intervention for a patient in a supine position, including positioning, passive & active range of motion, and splinting; 2) Level 2 was mobilizing a patient to a ring sitting or long sitting position in the bed or sitting at the edge of the bed; 3) Level 3 was mobilizing a patient out of bed, including transfers to a chair (wheelchair, feeder seat, infant swing), walking, or transferring to a caregiver’s arms (see Fig. 1). The comparison group included anyone who was eligible for level 2 or 3 EM while intubated, but did not receive it, based on retrospective chart review. Eligibility criteria was created by the EM task force to prioritize patient safety due to the higher risk of hemodynamic instability of these patients and included: positive end expiratory pressure (PEEP) of less than 10 mmHg or mean airway pressure of less than 18 mmHg, hemodynamic stability for > 12 hours, and an appropriate level of wakefulness to participate in the EM session. Patients were considered ineligible for EM if they had spinal precautions, were considered a “difficult airway,” had orthopedic restrictions, elevated intracranial pressures, or were within the first 72 hours of severe traumatic brain injury management. All in the comparison group received level 1 interventions while intubated, and once extubated, advanced to levels 2 and 3 when medically ready.
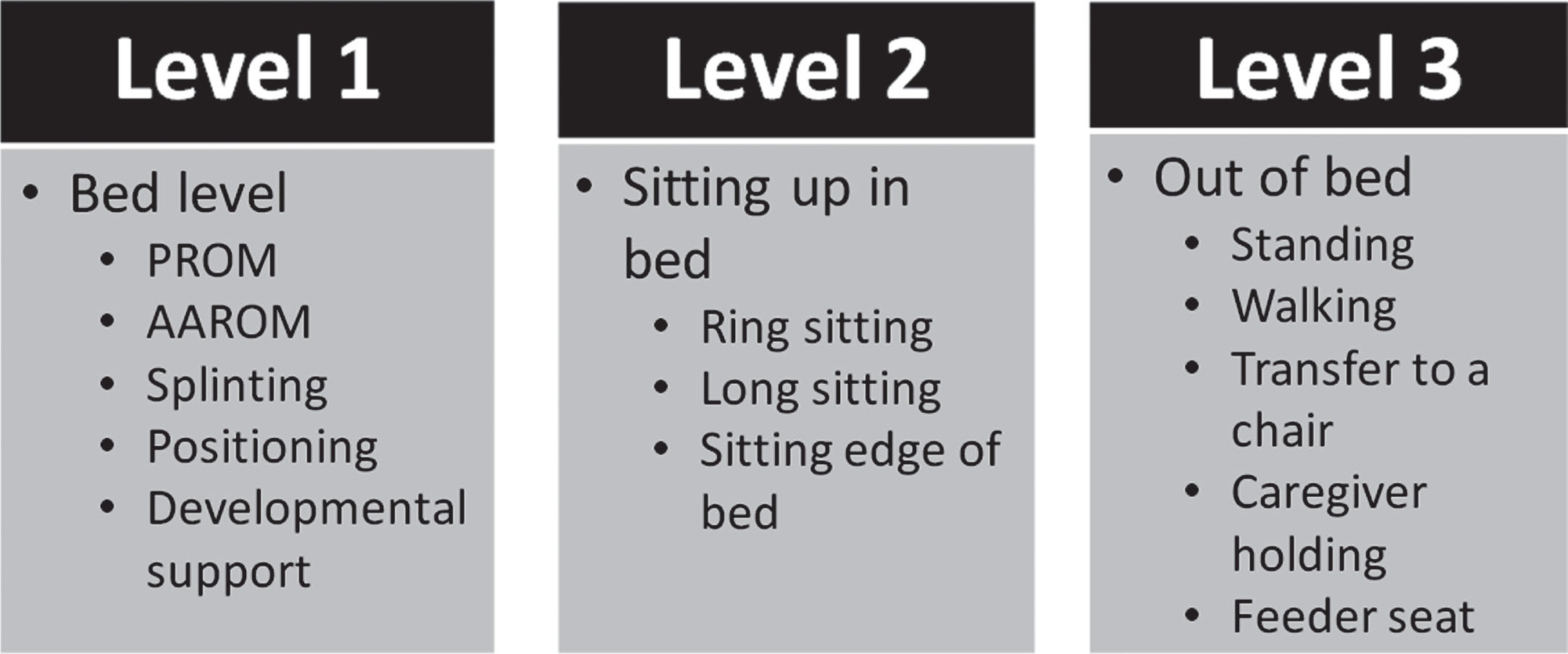
Levels of mobility. PROM = passive range of motion; AAROM = active assisted range of motion.
PICU patients were evaluated by a team of physiatrists for medical appropriateness to transfer to IRU. Patients had to meet admission criteria for inpatient rehabilitation, which required needing at least two of three rehabilitation disciplines: PT, OT, or speech language pathology (SLP). They must be able to tolerate three hours of therapy each day, have a caregiver present for training, and be medically cleared for rehabilitation. All patients were scored on the WeeFIM at admission and discharge, which is a standardized measure of functional performance for use in children aged six months through seven years, or in adolescents up to 21 with developmental disabilities.
EM protocol
An EM task force was created in 2014, consisting of physician champions, rehabilitation and nurse leaders, PTs, OTs, respiratory therapists (RT), and a child life specialist. In that year, the first intubated patient was mobilized from supine to a sitting position at the edge of the bed. Over the next four years, the task force defined levels of mobility (as defined above, as well as in Fig. 1) to indicate each patient’s readiness for progression of mobilization. A checklist was created in 2015 to ensure that a stepwise approach was taken to prioritize safety of the patient and minimize risk of adverse events during EM sessions. Each EM session required a dedicated team with a predefined role. The team included: a PT and/or OT, an RT, and the bedside nurse. Additionally, a physician order for EM had to be in place prior to each session. Immediately following each session, a form was completed in RedCap to record any adverse events, defined as: unplanned extubation, hemodynamic instability, loss of central venous line, loss of arterial line, displacement of extracorporeal membrane oxygenation (ECMO) cannula, or cardiopulmonary arrest. Extensive education for rehabilitation and ICU staff was completed from 2015–2019 to ensure their understanding, buy-in, and comfort. This was achieved through multiple avenues including but not limited to daily rounds, nursing education carts, lunch-and-learn sessions for staff, and newsletters.
WeeFIM
The WeeFIM measures 18 different items in 3 categories (self-care, mobility, & cognition) and each one scores from 1–7 on assistance needed from “total assistance” to “complete independence” [21]. WeeFIM scores were indicated by category at admission to IRU, adjusted for age-norms, and reported as a developmental functional quotient (DFQ) score.
Prism scores
Pediatric Risk of Mortality (PRISM IV) scores were obtained for all patients to compare both groups for risk of mortality and morbidity, and therefore severity of illness. The PRISM score is a physiologically-based severity of illness measure using 17 commonly measured physiologic variables and their ranges [22]. The higher the score, the higher the risk of morbidity and mortality [23].
Statistical analysis
Data was extracted and stored on the shared drive in a password protected folder; only study personnel had access to it. There were no hard copies of the data. Descriptive statistics were computed for the demographic and clinical variables for the EM and comparison groups when stratified by clinical diagnosis. This included means, standard deviations, medians, interquartile range (IQR), counts, and percentages, as appropriate. Only respiratory, neurology, and trauma/neurosurgery diagnoses were compared due to sample sizes (see Table 1). Unpaired t-tests (parametric) and Wilcoxon tests (non-parametric) were used to compare continuous data, while Chi-squared tests and Fisher tests were used to compare categorical data to evaluate the differences between the EM and comparison groups. Statistical significance was assessed at the p≤0.05 level. Because this study was exploratory and had a small sample size, multiple testing correction was not required. The analysis was conducted utilizing the statistical software R [24].
Admitting diagnosis category
Admitting diagnosis category
From 2015–2019, 1269 patients were intubated in the PICU for greater than 48 hours; 320 (25%) transferred to IRU at discharge. Of those transferred to IRU, 189 were deemed eligible to be included in this study. Of these patients, 78 had received EM (level 2 or 3 mobility) while intubated and 111 were deemed eligible for EM by retrospective chart review but did not receive EM interventions. (See Fig. 2 for inclusion criteria.) A total of 47 patients in the EM group achieved level 2 mobility as their highest level, and 31 patients achieved level 3 mobility while intubated. During an EM session, there were zero adverse events, again defined as unplanned extubation, hemodynamic instability, loss of central venous line, loss of arterial line, displacement of ECMO cannula, or cardiopulmonary arrest.
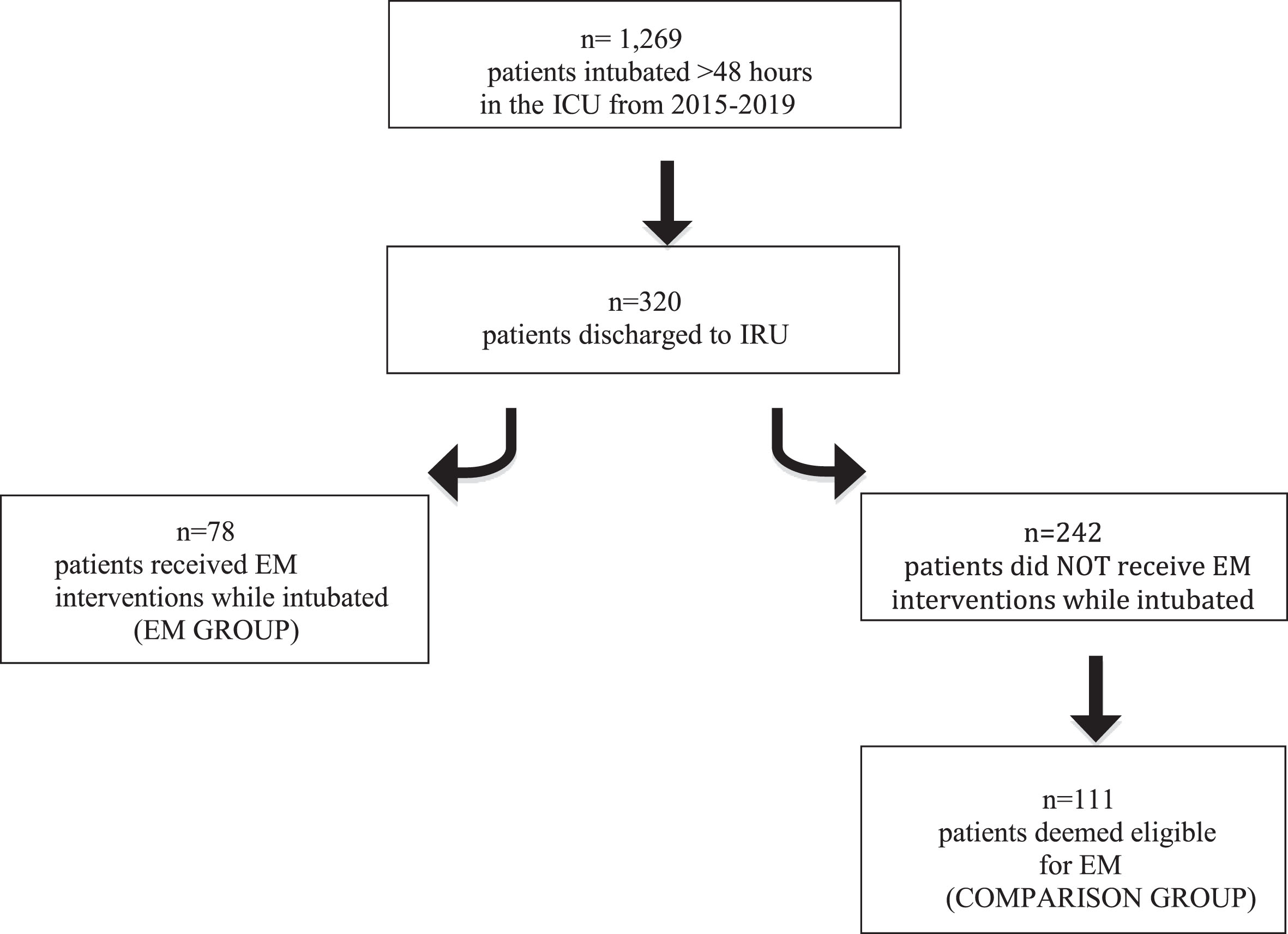
Inclusion Criteria. ICU = intensive care unit; IRU = inpatient rehabilitation unit; EM = early mobility.
When analyzed by diagnosis, respiratory patients who received EM had higher total WeeFIM scores at the time of IRU admission (mean = 48.11 (SD 20.07)) compared to those who did not (mean = 39.87 (SD 21.06), p = 0.13), though this was not statistically significant. Patients who received EM had a statistically significantly higher score for the WeeFIM mobility subcategory (mean = 44.32 (SD 21.91)) than the comparison group (mean = 31.37 (SD 20.11), p = 0.02). Though not statistically significant, the EM group also had higher scores at admission for self-care (mean = 47.57 (SD 21.61)) than the comparison group (mean = 37.31 (SD 22.33), p = 0.078), as well as higher scores in cognition (mean = 55.34 (SD 24.63)) than the comparison group (mean = 54.94 (SD 30.11), p = 0.956). See Table 4.
Age and gender by diagnosis
Patients in the neurology group were admitted primarily for a non-traumatic neurological problem such as seizures, meningitis, and/or stroke. See Table 3 for demographics of patients. WeeFIM scores revealed the comparison group had higher scores in all categories at admission to IRU compared to the EM group, none of which were statistically significant. See Table 5 for comparison.
Age in years on admission to the intensive care unit
Respiratory group clinical outcomes and WeeFIM scores
**Patients omitted from WeeFIM scores if less than six months old. PRISM = Pediatric Risk of Mortality; LOS = length of stay; ICU = intensive care unit; IRU = inpatient rehabilitation unit; ETT = endotracheal tube; ADM = admission; DFQ = developmental functional quotient.
The trauma/neurosurgery group had patients with a primary diagnosis of a traumatic neurological problem such as traumatic brain injury (mild to severe) or spinal cord injury. See Table 3 for demographics of patients. The EM group had higher total WeeFIM scores at admission (mean = 32.83 (SD 16.63)) compared to the comparison group (mean = 32.34 (SD 18.40), p = .687), as well as higher cognition scores at admission (mean = 47.44 (SD 31.01)) compared to the comparison group (mean = 40.41 (SD 25.36), p = .652). The remainder of the scores at admission and discharge were higher for the comparison group than the EM group, see Table 6.
Neurology group clinical outcomes and WeeFIM scores
**Patients omitted from WeeFIM scores if less than six months old. PRISM = Pediatric Risk of Mortality; LOS = length of stay; ICU = intensive care unit; IRU = inpatient rehabilitation unit; ETT = endotracheal tube; ADM = admission; DFQ = developmental functional quotient.
For all three diagnosis categories, the EM group had higher PRISM scores and longer hospital LOS, PICU LOS, and IRU LOS, compared to the group that did not receive EM interventions. See Tables 4–6.
Trauma/neurosurgery group clinical outcomes and WeeFIM scores
**Patients omitted from WeeFIM scores if less than six months old. PRISM = Pediatric Risk of Mortality; LOS = length of stay; ICU = intensive care unit; IRU = inpatient rehabilitation unit; ETT = endotracheal tube; ADM = admission; DFQ = developmental functional quotient.
This study demonstrated several key results. First and most notably, even though they were more critically ill based on PRISM scores, the EM group had slightly higher WeeFIM scores at admission to IRU on a few categories indicating a higher functional level soon after discharge from the PICU. However, results did not demonstrate the EM group had significantly better outcomes for all diagnoses. Second, it was surprising to find that the groups were not homogenous in their severity of illness, with the comparison group having lower PRISM scores for all diagnoses than the EM group. Third, because the EM group was more critically ill, they also had longer hospital LOS, IRU LOS, and more days with an ETT, which is not what was hypothesized.
The most notable finding similar to what was hypothesized was the respiratory group having statistically significantly higher WeeFIM scores on the mobility subcategory at admission to IRU than the comparison group. One explanation is that because the EM group was mobilized while intubated and worked on functional tasks such as bed mobility, sitting balance edge of bed, ADLs while sitting or standing, and cognitive tasks, this group had improved function upon admission to IRU. The literature to support this is limited due to the heterogeneity of the term “early mobilization” which can mean anything from passive range of motion to walking, or “early” in a PICU stay whether they are MV or not. One important point is that there needs to be clearer, standardized language around the phrase “early mobilization”. A randomized controlled trial (RCT) by Schweickert et al. specifically looked at functional outcomes in adults following EM while MV, finding a significantly functional status (as measured by the Barthel Index) at hospital discharge [2]. In a systematic review by Adler et al, four studies were identified that looked at Functional Independence Measure (FIM) scores in adults following EM interventions, and found that three of them reported an increase in FIM scores in the treatment group versus the control group [12]. However, all of these studies differed in their definition of EM, and none of them focused solely on patients who did level 2 or 3 mobility while MV as this study did. The results of the respiratory group however could be confounded by age, as the EM group was significantly older than the comparison group.
PRISM scores were higher across all diagnosis categories for the EM group versus the comparison group, indicating that patients in the EM group had a higher acuity level, and yet still demonstrated slightly higher WeeFIM scores on some categories. PRISM scores were initially chosen as a data point to demonstrate homogeneity so WeeFIM scores could be more objectively compared. However, it was not expected for there to be a significant difference between the groups like the data showed and for the EM group to have higher PRISM scores. This was a limitation of the retrospective nature of the study and could have been a result of self-selection bias. Selecting patients who were more critically ill for the EM group also likely resulted in this group having longer ICU & hospital LOS as well as more days with an ETT, the opposite of what this study was hoping to demonstrate. One reason this occurred was that EM is a novel intervention plan. It is not standard practice for all patients intubated > 48 hours to automatically participate in level 2 and 3 EM. Some in the comparison group may have been intubated for just over 48 hours, then extubated soon after. Many of the EM patients may have been intubated for days or weeks before they were considered. Hence, they had a higher acuity level, and therefore had higher PRISM scores and longer LOS. Barriers that may have prevented some patients in the comparison group from receiving EM interventions while intubated include staff availability, staff buy-in to a new intervention, medical procedures or temporary decline in medical status at the time an EM session was scheduled, and difficulty in optimizing sedation level for patients to be awake to participate. An important finding was there were no serious adverse events during EM treatment sessions, despite the high acuity level of the patients who were mobilized while intubated.
A few pediatric centers have reported outcomes of their EM program, but most of them include all patients in the PICU, not just those with an ETT completing level 2 and level 3 mobility making it difficult to compare results [16, 20]. Ten multidisciplinary experts in critical care and rehabilitation published an article in 2018 outlining practice recommendations for EM of critically ill children [25]. The authors agreed that MV should not be a contraindication to participation in EM activities, but rather a precaution to ensure that a safe approach is taken with these patients. This study supports the idea that EM can be done safely with patients who are considered to be critically ill, including those with an ETT, with a safe, methodical, multidisciplinary approach.
There are several limitations to this study. As a retrospective review, only associations can be presented; causality cannot be inferred. Another limitation was the small sample size in one institution. Results also may not be generalized to the greater population because of potential age differences between groups, level of illness severity, sociocultural, and regional differences by location.
Conclusion
A retrospective comparison between patients who received EM interventions while MV and those who did not indicated that patients with a higher acuity level were more likely to be mobilized, and it was done so safely. Patients with a primary respiratory diagnosis who received EM interventions had higher WeeFIM mobility scores on admission to IRU indicating they were functioning at a higher level compared to those who did not. An important finding of this retrospective study was that there were no adverse events during EM therapy sessions indicating that it can be done safely with proper protocols. Future studies that are prospective in nature are needed to demonstrate the importance of EM in improving patient function.
Conflict of interest
The authors have no conflicts of interest or sources of funding to acknowledge.
Ethical considerations
Approval was obtained by the Children’s Healthcare of Atlanta institutional review board (IRB) on June 10, 2019, approval number: STUDY00000195.
Footnotes
Acknowledgments
The authors have no acknowledgements.