
Abstract
PURPOSE:
The current study aimed to explore Gross Motor Function Measure (GMFM) profiles among children with cerebral palsy (CP) at various Gross Motor Function Classification System (GMFCS) levels in a low-resource setting.
METHODS:
Ambulatory capacity of children with CP was classified using GMFCS levels. Functional ability of all participants was measured using GMFM-88. Seventy-one ambulatory children with CP (61% males), were studied after signed informed consent was obtained from parents and assent from children older than 12 years.
RESULTS:
Children with CP in a low-resource setting had 12–44% lower GMFM scores in dimensions of standing, walking, running, and jumping with reference to children from high-resource settings with similar ambulatory capacity reported previously. The most affected components across various GMFCS levels were ‘sitting on a large and small bench from floor,’ ‘arm-free squatting,’ ‘half-kneeling,’ ‘kneel-walking,’ and ‘single-limb hop’.
CONCLUSION:
Knowledge of GMFM profiles can guide clinicians and policymakers in low-resource settings for strategic rehabilitation planning and extend the focus of rehabilitation from restoration of body structure and function to the wider domain of social participation in leisure, sport, work, and the community at large. Additionally, providing tailored rehabilitation based on a profile of motor function can ensure an economically, environmentally, and socially sustainable future.
Introduction
Children with cerebral palsy (CP) present delayed development of gross motor movement and balance which affects daily functions such as rolling, sitting, standing, and walking. Impairment of gross motor function reduces a child’s capacity to function in their environment and restricts participation in society [1]. The Gross Motor Function Classification System (GMFCS) is a five-level scale designed to record gross motor function of children with CP. The Scale is developed to classify severity of functional limitation/disability and ambulatory capacity of children with CP using qualitative measures. The scale rates a child’s gross motor function with an emphasis on movement initiation, sitting control, and walking. The GMFCS scale focuses on functional limitations and the need for assistive technology and mobility devices for ambulation, including wheeled mobility, rather than quality of movement. Literature reports good inter-rater reliability of 0.75 and very good predictive validity of the tool for children over the age of two years [2].
Major determinants of gross motor function among children with CP at various GMFCS levels include severity in primary impairments (namely spasticity, quality of movement, postural stability, and distribution of involvement) and secondary impairments (namely poor muscle strength, range of motion limitations, and reduced endurance). Adaptive behaviour and participation in the community are also recognized as significant minor determinants of gross motor function in children with CP [3, 4].
In addition to primary and secondary impairments, a wide range of intrinsic and extrinsic factors also affect gross motor function among children with CP [5]. Intrinsic factors include inherent characteristics of a child such as puberty and motivation [6]. The extrinsic factors affecting functional motor outcomes are family dynamics such as support systems, parental stress, adherence to a home-based program, parenting style, and availability, access, and options for interventions [4].
Development of gross motor function determines a child’s physical functioning capacity and participation in various social roles (education, employment, leisure, etc.) [7]. Typically, children with CP achieve their maximum potential of gross motor function around the age of 6-7 years. However, children with poor ambulatory capacity reach a plateau in motor development at a much younger age compared to children with higher ambulatory capacity [5]. Therefore, the universal fundamental goal of rehabilitation is to optimize gross motor function, which is inclusive of improving adaptive function, preventing development of secondary impairments, and promoting participation in daily life [4]. However, in low-resource settings, rehabilitation goals are driven mainly by societal and parental expectations. A 2021 systematic review suggested that low-resource settings are challenged by suboptimal healthcare service delivery, underdeveloped infrastructure, unmet rehabilitation needs (affordability of services and treatment, lack of insurance) [8], and poor environmental access to rehabilitation (distance to service, lack of access to or unaffordable cost of transport). Additionally, lack of skilled rehabilitation practitioners (fewer than 10 skilled rehabilitation practitioners per one million population) [8], lack of an adequate skilled rehabilitation workforce in rural areas [9], paucity of knowledge regarding CP, and the negative influence of beliefs and practices (including perceived need, fear, and lack of awareness about services) have resulted in underutilization of rehabilitation services in low-resource settings [8, 10].
In routine clinical settings, independence in walking is set as an essential long-term goal of rehabilitation from the perspective of both therapists and parents [11]. Moreover, walking is considered a symbol of independent, non-disabled living that provides an individual with the advantage of a secure future in work settings and socialization [12]. Such beliefs drive parents to expect the child to walk independently, because it is perceived as a symbol of normality [13]. This is the most likely reason that most parents and primary caregivers in low-resource settings discontinue supervised rehabilitation once the child has achieved independent walking. A recent study reported that only 26% children older than 3 years utilize rehabilitation services in low-resource settings [14]. Consequently, most children remain unmonitored until 9-10 years of age, which coincides with their growth spurt.
Development of gross motor function among children with CP in high-resource settings has demonstrated predictable patterns based on the child’s overall motor severity [5]. However; the gross motor function profiles of children with CP in low-resource settings with limited social, attitudinal, and environmental adaptations remain unexplored. Patterns of functional severity and motor type are known to vary among children with CP across different resource settings [15]. Hence, it is reasonable to speculate that gross motor function profiles of children with CP at similar GMFCS levels are likely to be influenced by the resource setting.
The present study aimed to explore the profiles of gross motor function among children with CP at various GMFCS levels in a low-resource setting. Findings will be useful to clinicians, policymakers, parents, and primary caregivers in comprehensive planning of rehabilitation goals. Additionally, they may urge policymakers to call for a reflection on the model of care in order to identify modifications required in current therapy guidelines and delivery systems for optimal utilisation of existing resources. Information on gross motor profiles may also help in building a sustainable model of rehabilitation, ensuring greater participation of children with CP in society [16].
Materials and methods
Participants
The study was approved by the Institutional Ethical Review Committee. Seventy-one ambulatory children (5–18 years old) with spastic CP (61% males and 39% females) who were able to comprehend instructions were studied after obtaining signed informed consent from parents and assent from children older than 12 years. Demographic characteristics are presented in Table 1. Data was reported for children at GMFCS levels I to IV. Sixty-eight children presented with bilateral spastic diplegic CP and three presented with unilateral CP. A total of five children had undergone at least one soft tissue release procedure, i.e., tendoachilles release [n = 5] and hamstring release [n = 4]. Twenty children had received botulinum toxin intervention at least eight months prior to evaluation. None of the children reported surgical bony corrections. Three children at GMFCS level III and five children at GMFCS level IV used walking aids with bilateral AFOs for ambulation. The remaining six children used hand-held assistance from a caregiver for indoor and outdoor ambulation. Twenty-nine children out of 71 were undergoing supervised therapy (minimum of three therapy sessions per week) during the study period. The remaining 42 children did not receive any supervised therapy or home exercise program; however, they performed routine functional tasks of daily living.
Characteristics of patients along with Gross Motor Function Classification System (GMFCS) levels
Characteristics of patients along with Gross Motor Function Classification System (GMFCS) levels
A physiotherapist with over 10 years’ experience in treating children with CP evaluated the functional ability and ambulatory capacity of all participants using the Gross Motor Function Measure (GMFM).
The GMFM is a test specially designed and validated for measuring gross motor function and the change over time in children with CP. The 88 items measuring gross motor function are distributed over five dimensions: A - lying and rolling; B - sitting; C - crawling and kneeling; D –standing; and E -walking, running, and jumping. The GMFM was constructed to measure quantitative aspects, viz., how much children can do, not the quality of their performance [17]. It is known that poor ambulatory capacity is associated with decreased motor ability in children with CP [5].
All participants were tested barefoot without walking aids. The same physiotherapist also classified each patient’s functional ambulatory capacity using the GMFCS tool. GMFM and dimension scores were computed as per standard protocol. A percentage score was computed for each dimension, and an overall score was obtained as a quotient of the sum of percentages divided by the sum of dimensions [17]. Data were analysed statistically using SPSS version 24 (IBM, New York, USA). Normality of distribution was ascertained using the Kolmogorov Smirnov test. Measures of central tendency and dispersion were calculated and reported as means and standard deviation. One–way analysis of variance (ANOVA) was used to study difference across four GMFCS levels for each dimension of GMFM scores, with level of significance set at p≤0.05 and GMFCS as an independent variable (factor). The linear contrast was applied to observe trends of decline for GMFM dimensions across GMFCS levels. Post-hoc analysis was performed using a Bonferroni test. Four Bonferroni corrections were adjusted at 0.01 to avoid type I error. The power was set at p < 0.01.
Results
A total of 71 children with CP were evaluated and classified by ambulatory capacity based on the GMFCS into four groups (refer to Table 1). The gross motor function characteristics of children and topographic classification (viz. unilateral or bilateral spastic CP) are presented in Table 1. All children were matched on marginal distribution of age, body height, and body weight. Although average values of age, body height, and body weight were marginally higher in GMFCS levels II and IV compared to children at GMFCS I and III, the difference was not statistically significant.
Table 2 presents GMFM scores of children with CP at GMFCS levels I, II, III, and IV. The total GMFM score and individual dimension scores were normally distributed. The total GMFM score was 91.26% in GMFCS level I, 75.42% in GMFCS II, 53.58% in GMFCS III, and 45.92% in GMFCS IV. Significant linear decline was observed in mean GMFM scores from GMFCS level I to GMFCS IV (p < 0.01). Further analysis of individual dimensions (i.e., A - lying and rolling; B –sitting; C -crawling and kneeling; D –standing; and E - walking, running and jumping) demonstrated a significant linear decline across GMFCS levels I to IV (p < 0.01) (Fig. 1). Activities in standing (dimension D) and walking, running, and jumping (dimension E) were most affected (performed least) across all GMFCS levels.
Activity (%) based on five domains of the Gross Motor Function Measure (GMFM) across Gross Motor Function Classification System (GMFCS) levels
Activity (%) based on five domains of the Gross Motor Function Measure (GMFM) across Gross Motor Function Classification System (GMFCS) levels
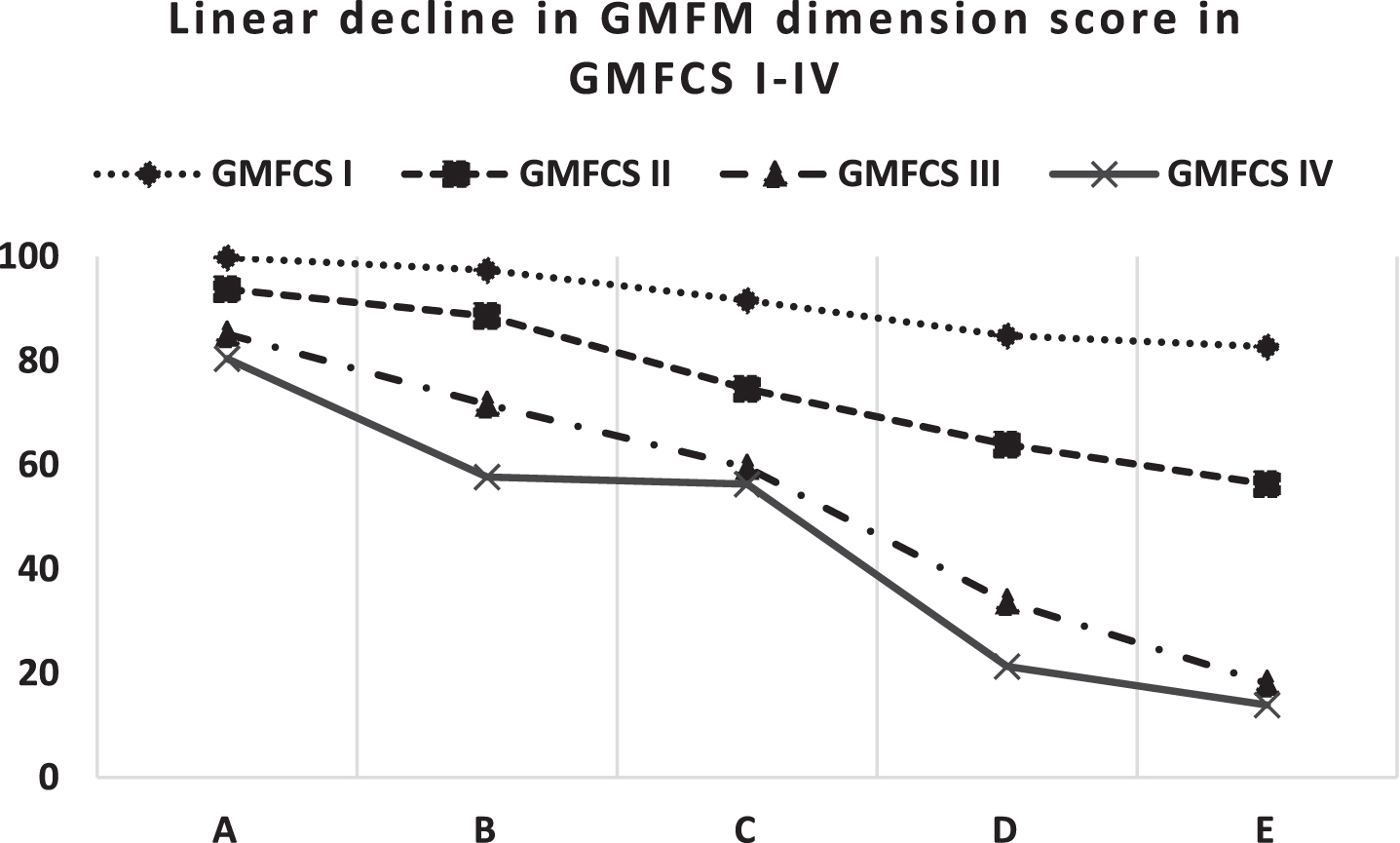
Linear decline in Gross Motor Function Measure (GMFM) dimension scores across various Gross Motor Function Classification System (GMFCS) levels. A - Lying and rolling, B - sitting, C - crawling and kneeling, D –standing, and E –walking, running and jumping.
At GMFCS level I (n = 21), ‘sit on large bench from floor’ was the most affected component in dimension B. None of the children at GMFCS level I completed all items in dimensions C (crawling and kneeling), D (standing), or E (walking, running, and jumping). Half-kneeling and forward-kneel walking were the most affected components in dimension C. Fifty percent of children at GMFCS level I could partially complete ‘lowering down to sit on floor’ and ‘squatting from standing position’. In dimension E, ‘hopping on single leg within 60 cm box’ was the most difficult task.
Three children with unilateral impairment could complete lying and sitting dimensions. The most affected components in dimensions C, D and E were ‘half kneeling arms free’, attaining ‘standing through half kneeling’ and ‘squatting arms free’, ‘stepping over knee level obstacle’, and ‘single leg hopping’, all on the affected side.
At GMFCS level II, ‘rolling from supine to prone’ and ‘prone to supine’ were the two most affected items in dimension A (lying). In dimension B, ‘sitting on a small bench from floor’ and ‘sitting on a large bench from floor’ were the two most affected items. In dimension C, more than 50% of children could partially complete crawling, kneeling, and half-kneeling activities, whereas maintenance of ‘half kneeling for 10 seconds’ was the most difficult task. In dimension D, attaining ‘squat arms free’ was the most affected component, followed by ‘return to stand arms free after picking up object from floor’ and ‘standing from half kneeling’. In dimension E, all children had difficulty in performing ‘single limb hop’, ‘high jump (30 cm)’, ‘forward jump by 30 cm’, ‘jumping with both feet’, and ‘obstacle crossing for each foot at knee level’.
Among GMFCS level III (n = 9), only two-thirds of children partially completed six items in the lying and rolling dimension. ‘Rolling from supine to prone’ and from ‘prone to supine’ were the most affected items in dimension A. In dimension B, less than 50% of children could barely initiate ‘sit on mat with feet in front and pivoting on either sides’ and ‘sitting on small and large bench from the floor’. In dimension C, maintenance of ‘half kneeling arms free’ and ‘kneel walking’ were the most difficult tasks. In dimension D, none of the children completed all of the items. Maintenance of ‘single limb stance on either side for 10 seconds’, ‘lowering oneself to sit on floor from standing position’ with control (arms-free), ‘attaining squat (arms free)’ and ‘return to stand with arms free after picking up an object from floor’ were the four most affected items in dimension D for children at GMFCS level III. All children at GMFCS levels III and IV were unable to perform all activities of dimension E (i.e., stand and walk without assistance).
At GMFCS level IV, all children were unable to complete the activities of dimension A. In dimension B, all children could only partially complete activities involving independently sitting on a mat. In dimension C (crawling and kneeling), all of the children partially completed items but were unable to perform half-kneeling and kneel walking activities. All children were unable to perform activities in standing (arms-free) and half-kneeling (Fig. 2).
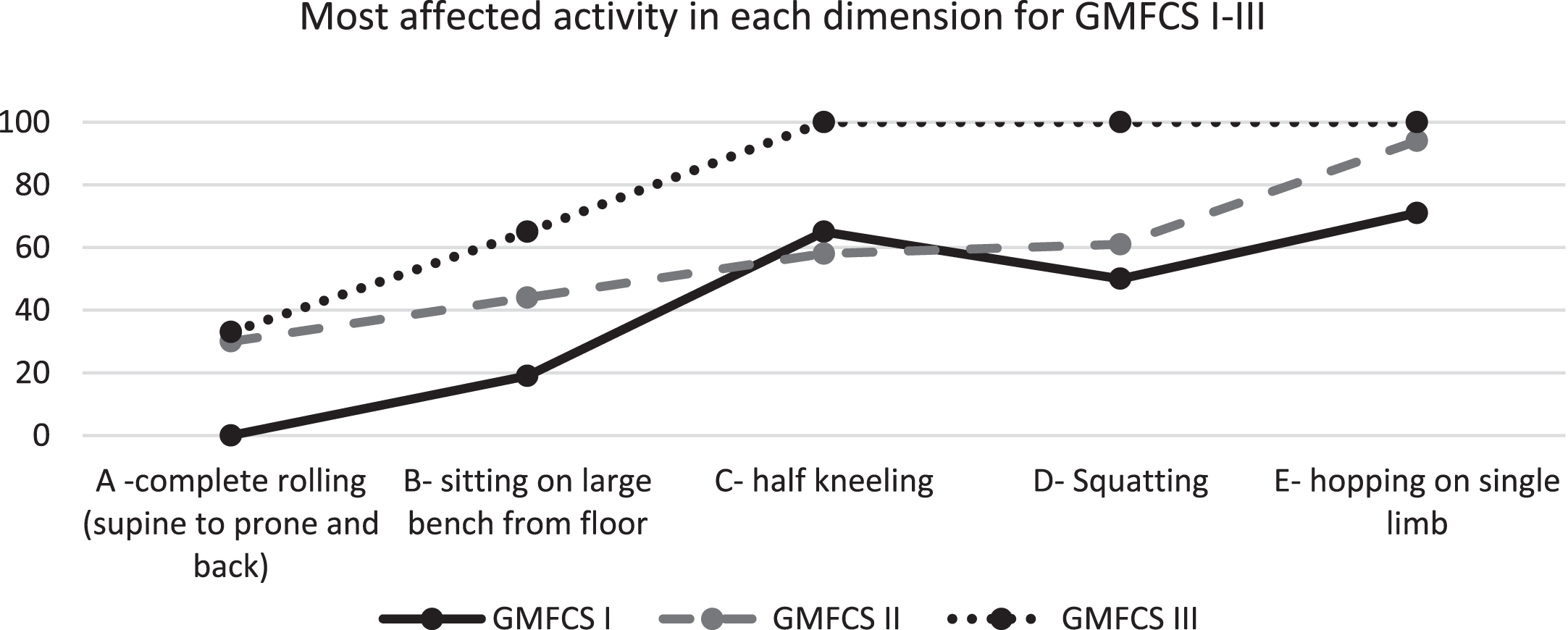
Most affected activities in Gross Motor Function Measure dimension among children with cerebral palsy from a low-resource setting. For GMFCS level I, the percentage of children who were able to partially complete the activity is shown, whereas for GMFCS levels II and III, the percentage of children who were unable to perform or initiate the activity is shown. GMFCS: Gross Motor Function Classification System.
Data from previous published studies that reported findings of dimensions D and E of children with CP from high-resource settings were referenced while reporting findings of this current study of children from a low-resource setting. Figure 3 presents the difference between dimension D and E scores of children with CP from low-resource settings (findings of present study) and high-resource settings (reported in previous studies).
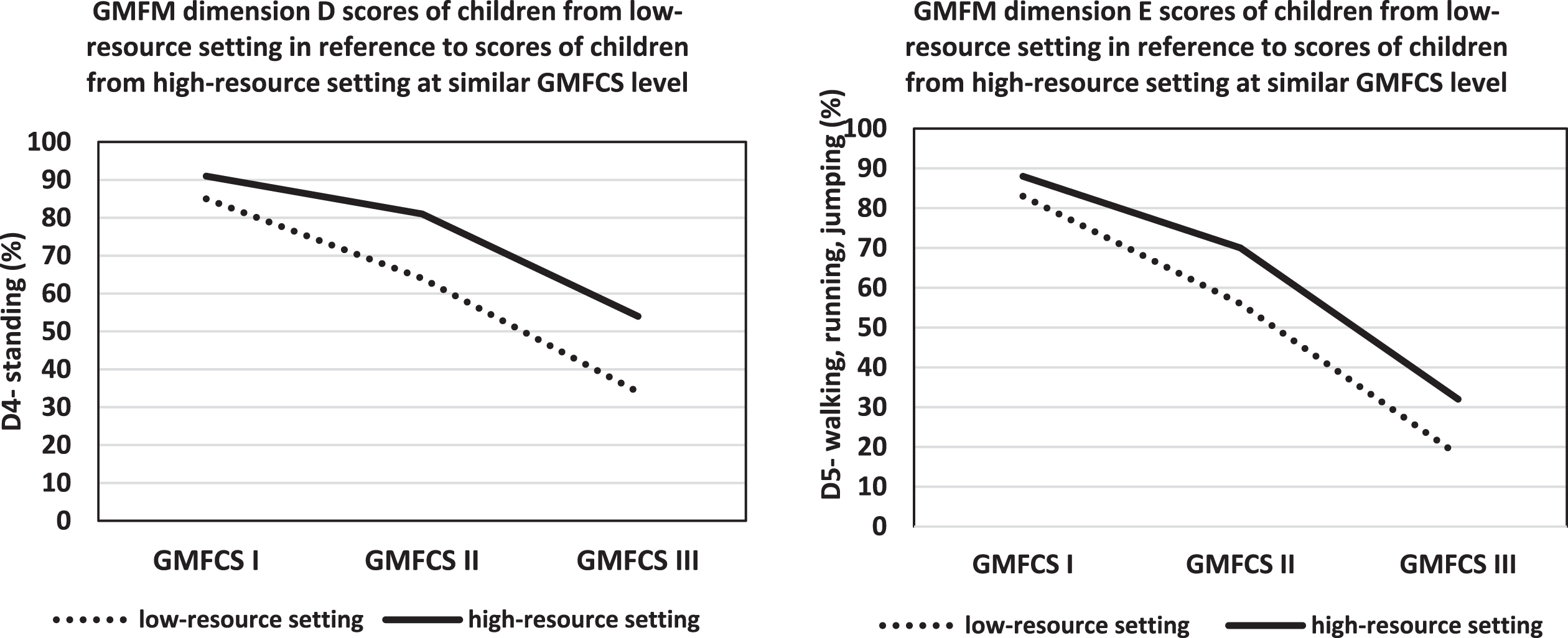
Gross Motor Function Measure (GMFM) dimension D and E scores of children from the present study (i.e., low-resource setting) with reference to children at similar Gross Motor Function Classification System (GMFCS) levels from a high-resource setting [19].
The present cross-sectional study reported gross motor function profiles of children with CP in a low-resource country. Findings suggested that children with poor ambulatory capacity demonstrated lower scores in gross motor function. Standing (dimension D) and walking, running, and jumping (dimension E) were the most affected domains.
Previous studies predicted ambulatory capacity of children with CP based on GMFM walking dimension (E) scores. Children with scores between 77–100 were classified as high-motor functioning/GMFCS level I; 41–76 as middle-functioning/GMFCS level II; 0–40 as low-motor functioning/GMFCS III [18]. Although the children in the present study presented lower scores on the walking dimension E when compared to children in high-resource settings, the scores were within the predicted range of functioning. Hence, it is reasonable to argue that the children were appropriately classified at their true ambulatory capacity.
At GMFCS level I, 50% of the children partially completed components of standing (D) and walking (E) dimensions. At GMFCS level II, only 30% of children completed all items, whereas at GMFCS level III, 60% partially achieved items in the lying dimension (A).
Children across GMFCS levels I-III encountered difficulty in tasks demanding advanced postural strategies, namely half-kneeling, arms-free squat, obstacle crossing, and single limb hop. Additionally, children within the middle- (GMFCS level II) to low-motor functioning levels (GMFCS level III and IV) also demonstrated difficulty in ground-level transitions (rolling from supine to prone and prone to supine).
Furthermore, dimension D (standing) and E (walking, running, and jumping) scores of children with CP from a low-resource setting were lower (10–12% lower in GMFCS level I; 24% in GMFCS level II; and 37–44% lower in GMFCS level III) with reference to scores reported in the literature for children at similar GMFCS level from high-resource settings (Fig. 3) [19]. Although the trend of linear decline in motor functioning with increasing neuromotor severity was similar in both settings, there was a difference in the motor function profile of children at similar GMFCS levels across different resource settings.
Performance of activities of daily living is known to be influenced by a wide range of intrinsic (physical: spasticity, poor muscle strength; cognitive: motivation) and extrinsic factors (contextual: dynamics and functioning of the family, availability and access to therapeutic interventions) [5]. Poor performance in ground-level activities and activities demanding controlled descent of the body into gravity could be attributed to poor lower extremity strength and endurance in children with CP. A previous study has reported 54–73% lesser lower extremity strength and endurance among children with CP compared to healthy children [20], wherein muscle strength was assessed using functional tasks such as the step up test, chair raise test, and calf raise test [20]. Reduced lower extremity muscle strength and endurance are known determinants of motor function [19]. Additionally, overall lower GMFM scores of standing (D) and walking E dimensions could also be attributed to a lack of adequate function-based therapeutic intervention, which are designed for overall improvement of activity and participation of children in their communities. Hence, it is deemed essential that the rehabilitation practices in low-resource settings account for the contextual factors and demands placed on the child to ensure active participation in school, play, and society.
Previous studies have demonstrated a positive correlation between deterioration in mobility and lack of physiotherapy and physical activity [14]. Therefore, reduced lower extremity muscle strength and endurance compounded by a lack of adequate physical activity or continued therapy could be speculated as a reason for low gross motor function scores of children with CP in low-resource settings despite similar ambulatory capacity.
Additionally, in resource-constrained settings, infrastructure, social, and financial extrinsic factors play a large role in the participation of children with CP in activities of daily living, school, sport, and leisure, over and above the physical challenges posed by body impairments [15, 21].
Factors such as delayed diagnosis, lack of availability of paediatric rehabilitation specialists in close proximity, lack of infrastructure to support inclusive transportation, excessive emphasis on scholastic achievement leading to compromised therapy time in older children, lack of in-house rehabilitation specialists, financial constraints due to out-of-pocket payments, and other contextual factors (viz. family support, lack of adherence to home program) lead to lower gross motor function among children with CP in low-resource settings. Furthermore, there is a gap between parents’ expectations from therapy and actual rehabilitation goal-setting practices in routine clinical settings in low-resource settings.
Therefore, understanding the complete profile of functioning is important for developing context-specific therapy guidelines. Clinical guidelines can help therapists (including novice therapists) and other members of the rehabilitation team adopt a comprehensive, evidence-based model of functioning such as the International Classification of Functioning, Disability and Health for evaluation, design, and monitoring of intervention strategies.
Detailed comprehensive information on the motor functioning profile can also aid in planning tailored, home-based therapy focused on goal setting and functional training in partnership with families and caregivers. Active engagement of parents and caregivers in the therapy can enhance compliance. Such a strategy can help to reduce the burden of financial cost and difficulties encountered in travel to rehabilitation centres because of inaccessible infrastructure in low-resource settings.
In parallel, it is necessary to provide an inclusive environment to children in resource-constrained settings through accessible infrastructure to enhance their participation in school, sport, leisure, and social domains. Secondly, it would help to develop a national registry of children with neuro-motor impairments in low-resource settings. A national registry could allow for prospective, longitudinal study of etiologic, demographic, and functional severity and enable ongoing monitoring, follow-up, and continuum of care of children with CP at all levels of social participation, including those who discontinue therapy due to either relocation or financial constraints. In the absence of a centralized health care system in low-resource settings, such a registry could serve as an invaluable tool to monitor treatment outcomes for various age groups.
However, findings of present study should be interpreted in light of the following observations. The study sample represented middle-class urban-dwelling children; it did not present motor function of children with CP from rural areas. However, there is evidence suggesting no association between socioeconomic status and GMFCS levels even in resource-constrained settings, which suggests that economic status may not influence motor function profiles of children with CP [22]. Furthermore, the present study did not record contextual factors affecting functioning profiles and rehabilitation and therefore could not explore the dynamics between contextual factors and functioning profiles. Hence, further studies are necessary to understand the association between various clinical factors (e.g., effect of supervised therapy, home exercise program) and contextual factors such as family support as well as their relationship with gross motor function and ambulatory capacity among children with CP in low-resource settings.
Conclusion
Present findings report gross motor function profiles of children with CP from a low-resource setting. Fifty percent of children at GMFCS level I completed all activities of standing (D) and walking, running, and jumping (E) dimensions. Activities demanding ground-level transitions (rolling) and advanced postural control strategies (sitting on a large and small bench from the floor, arm-free squatting, half-kneeling, kneel walking, single limb hop) were the most affected components for children at various GMFCS levels. Children from a low-resource setting demonstrated 10–44% lower scores on standing, walking, running, and jumping dimensions in reference to children from high-resource settings at similar GMFCS levels. Knowledge of GMFM profiles will help clinicians and policymakers in strategic planning, which is essential to broaden the narrow focus of rehabilitation from mere restoration of bodily structure and function with a typical endpoint of gait training to a wider dimension of social participation of children with CP in leisure, sport, work, and the community at large.
Footnotes
Acknowledgments
We are thankful to all children and parents for participation in this research study.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
None.