
Abstract
Background:
Maternal infections are responsible for maternal mortality and can lead to adverse pregnancy outcomes such as stillbirth, maternal sepsis, and spontaneous abortion as well as dire outcomes for the neonate. The impact of obstetric infections is largely felt in low- and middle-income countries, with Pakistan being one such country.
Objectives:
To assess the frequency of maternal infections, the common sources responsible for their progression and their resulting impact on pregnancy, maternal, and neonatal health outcomes.
Design:
An observational cross-sectional study was conducted in a tertiary care, public sector hospital in Pakistan.
Methods:
A total of 439 women, either antenatal or postnatal, with symptoms of infection were enrolled. Case report forms were used to collect data on clinical characteristics, type of infection, investigational and diagnostic profile, and pregnancy, maternal, and neonatal outcomes. Frequency and percentages were computed for categorical variables. Comparisons of pregnancy and neonatal outcomes were analyzed by the chi-square test or Fisher’s exact through categorization of patients as per the severity of their condition.
Results:
The observed frequency of maternal infections was 12% in pregnant or recently pregnant women admitted during the study period. Respiratory tract infection (16.9%) and chorioamnionitis (14.4%) were more prevalent among antenatal women, whereas wound/skin infection (15.5%) and puerperal/genital tract infection (12.3%) were the most common infections observed in postnatal women. Blood transfusion was the most common complication observed in the included women (26.9%). Among the study population, 13.9% had organ dysfunction, primarily cardiovascular (42.6%) and neurological dysfunction (40.9%). Women with severe infection had adverse pregnancy outcomes such as a high number of still births (17.5%). The total number of maternal deaths recorded was 19 (4.32%). Regarding neonatal outcomes, APGAR score, suspicion of infection, and low birth weight were significant across the severity groups. There was no significant difference for neonatal deaths across the three groups.
Conclusion:
Infections from various sources contribute significantly toward adverse maternal, pregnancy, and neonatal outcomes. Enforcing infection prevention measures, equipping primary healthcare units with adequate resources and emphasizing antenatal and postnatal care can prevent infections and their related complications. Early detection and management of maternal infections is equally necessary.
Introduction
Maternal infections are one of the major causes of maternal mortality and severe maternal morbidity. 1 Maternal infections are associated with adverse pregnancy outcomes such as spontaneous abortion, stillbirth, low birth weight, increased risk of maternal sepsis, and death in severe cases. 2 In certain situations, the infection is transmitted to the fetus, resulting in neonatal morbidity or fetal loss. 3 Direct obstetric infections have been recognized as the third most common cause of maternal mortality, 1 representing around 10.7% of deaths in low- and middle-income countries (LMICs) compared to 4.7% of deaths in high-income countries. 1 The prevalence of maternal infection among women ranges from 17% to 44% in low- and lower-middle-income countries, whereas in upper-middle- and high-income countries, the prevalence is significantly lower, reported between 13% and 26%. 4
It is evident that maternal infections pose a threat to LMICs and that low-resource settings in these countries almost always have the highest burden of adverse maternal and neonatal outcomes due to infections. 4 Pakistan is one such country that faces a heavy burden of maternal infections. 5 Pregnant women in this region are predisposed to infections due to a multitude of factors. These risk factors include poor quality health services, struggle to access appropriate antenatal care (ANC), economic challenges, and cultural influences. 6 Lack of education and awareness among women and their families about seeking medical care during pregnancy and childbirth further acts as a barrier toward accessing appropriate care. 6 There is a scarcity of antenatal and postnatal care as well as a shortage of skilled birth attendants in the country. 6 Due to cultural factors in the country, there is an increased practice of home births. These are assisted by traditional birth attendants who lack the proper training needed to deal with infection-related obstetric complications. 7
Furthermore, as Pakistan is spending less than the World Health Organization (WHO) recommended GDP on its healthcare system, 8 the health facilities, especially in rural areas, have poor-quality maternal care services. 9 These facilities are under-resourced, have weak health infrastructure, and poor infection prevention and control practices, all of which combined exacerbate chances of contracting infections in pregnant women. 9 Hence, these complex and interlinked risk factors pose a challenge for the health system and policymakers to make improvements in the field of maternal infections.
There is a dearth of data on the actual incidence of maternal infections in Pakistan due to underreporting and absence of reliable surveillance systems through which to monitor the situation. 10 Consequently, maternal mortality is insufficiently reported by 27% and neonatal mortality by 50%. 10 In addition, there may be misclassification of the cause of death when fatalities are reported. 11 This further contributes to unreliability in the mortality data for maternal infections.
Thus, knowing the frequency, common sources and the resulting impact of infections on maternal health is necessary to develop context-specific interventions and guidelines tackling this issue.
This study was carried out in a large public sector hospital in Pakistan to assess the frequency of maternal infections, the common sources responsible for its progression and their associated maternal outcomes, severity of condition of patients, and its impact on pregnancy and neonatal health outcomes. We hypothesize that patients with maternal infections are at an increased risk of pregnancy and neonatal complications.
To test our hypothesis, we used data of maternal patients who were admitted with signs and symptoms of infection. The clinical presentation of included patients, their sources of infection, and their associated outcomes were assessed.
Methods
Study design and participants
An observational cross-sectional study was conducted in a large tertiary care, public sector hospital in Pakistan from June 2021 to December 2021. Women of reproductive age (15–49 years) who were admitted to the obstetrics and gynecology units of the selected facility were assessed for eligibility for inclusion in the study. The eligibility criteria included pregnant women or those within 6 weeks of the postpartum period, women with ectopic pregnancies, miscarriages, termination of pregnancy, or delivery. We included women if they had signs and symptoms suggestive of infection or had received a clinical diagnosis, made by onsite physicians, on the basis of clinical signs or symptoms suggestive of infection. The signs and symptoms suggestive of infection included, but were not limited to, fever, pain, tenderness, abnormal vaginal bleeding, foul smelling vaginal discharge, burning micturition, tachycardia, hypotension, hypothermia, or tachypnea. Although our target population was women of reproductive age, only those above 18 years of age were enrolled in the study. There were no exclusion criteria for the study.
The prevalence of maternal infection among women in low- and lower-middle-income countries has been reported to range between 17% and 44%. 4 Using a 95% confidence level and a 5% margin of error, the sample size was calculated based on the standard formula for estimating a single population proportion: n = Z 2 p (1 − p)/d2, with Z = 1.96 (for 95% confidence), p = 0.43, and d = 0.05. Thus, the estimated sample size was approximately 385 participants. However, to enhance the robustness of the study and include all eligible cases, a total of 439 participants were recruited during the study period.
Study setting
Study participants were enrolled from the Liaquat University of Medical and Health Sciences (LUMHS), which is a public, tertiary referral hospital situated in the second largest city in the province of Sindh (Hyderabad) in Pakistan. As LUMHS hospital provides free-of-charge services, it serves a large proportion of the underprivileged population from both urban and rural areas of Sindh, making it a true reflection of Pakistan’s general population.
Data collection
Study data were collected prospectively over a 7-month period from the medical records of maternal infection patients admitted to the obstetrics and gynecology units. Ethics approval was obtained from the Institutional Review Boards of the Aga Khan University (AKUH), LUMHS hospital, and National Bioethics Committee prior to collecting patient data.
All the women who were screened gave consent to be part of the study. Written informed consent was taken from the 439 enrolled patients prior to data collection (Supplemental Material 1). Data were collected by research staff who were trained to collect data on patients’ clinical characteristics, type of infection, investigational and diagnostic profile, and pregnancy and neonatal outcomes (where applicable) using case report forms (Supplemental Material 2).
Maternal and neonatal diagnoses were assigned as documented in the medical records.
Post hoc analysis was conducted through categorization of patients according to the severity of their condition according to a WHO global study. 4 The three groups were as follows: (1) less severe infections, (2) infection with complications, and (3) infection-related severe maternal outcomes. This categorization helped to assess the severity of conditions of patients with maternal infections enrolled in our study and to assess their pregnancy and neonatal outcomes.
Statistical analysis
Analyses were performed using SPSS 19.0 (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA). Frequency and percentages were computed for categorical variables. Comparisons of pregnancy and neonatal outcomes were analyzed by the chi-square test or Fisher’s exact. Statistical significance was accepted as p < 0.05.
STROBE guidelines have been used to prepare this manuscript (Supplemental Material 3).
Results
A total of 3602 obstetric patients were admitted to OBGYN units of the hospital during the study period from June 2021 to December 2021. The 439 women included in this analysis were suspected of infection on admission or had developed an infection during their hospitalization. More than half of the women admitted with signs and symptoms of infections were antenatal (257/439, 58.5%), with majority (246/257, 95.7%) in the third trimester. From the perspective of infection severity, the highest percentage was of women in their third trimester falling in the less severe infection category (83.8%). Abnormal pain (45.8%), fever (26.9%), and vaginal bleeding (23.5%) were the common signs and symptoms at the time of admission. The primary source of infection was identified in 304 out of the 439 patients enrolled in the study. The remaining 135 patients were enrolled based on clinician’s suspicion and signs and symptoms suggestive of infection. Respiratory tract infection (RTI; 24.3%), wound/skin infection (22.3%), chorioamnionitis (21%), puerperal/genital tract infection (17.5%), and urinary tract infection (UTI; 11.18%) were the most common sources of infection (Table 1). Other sources included tuberculosis, breast infections, meningitis and chronic viral infections including Hepatitis B and C. The identified primary sources of infection in the enrolled patients, categorized by their pregnancy status, are presented (Figure 1).
Clinical characteristics of maternal patients (n = 439).

RTI: respiratory tract infection; UTI: urinary tract infection.
Count of multiple signs and symptoms and primary sources is greater than total sample size (n = 439).
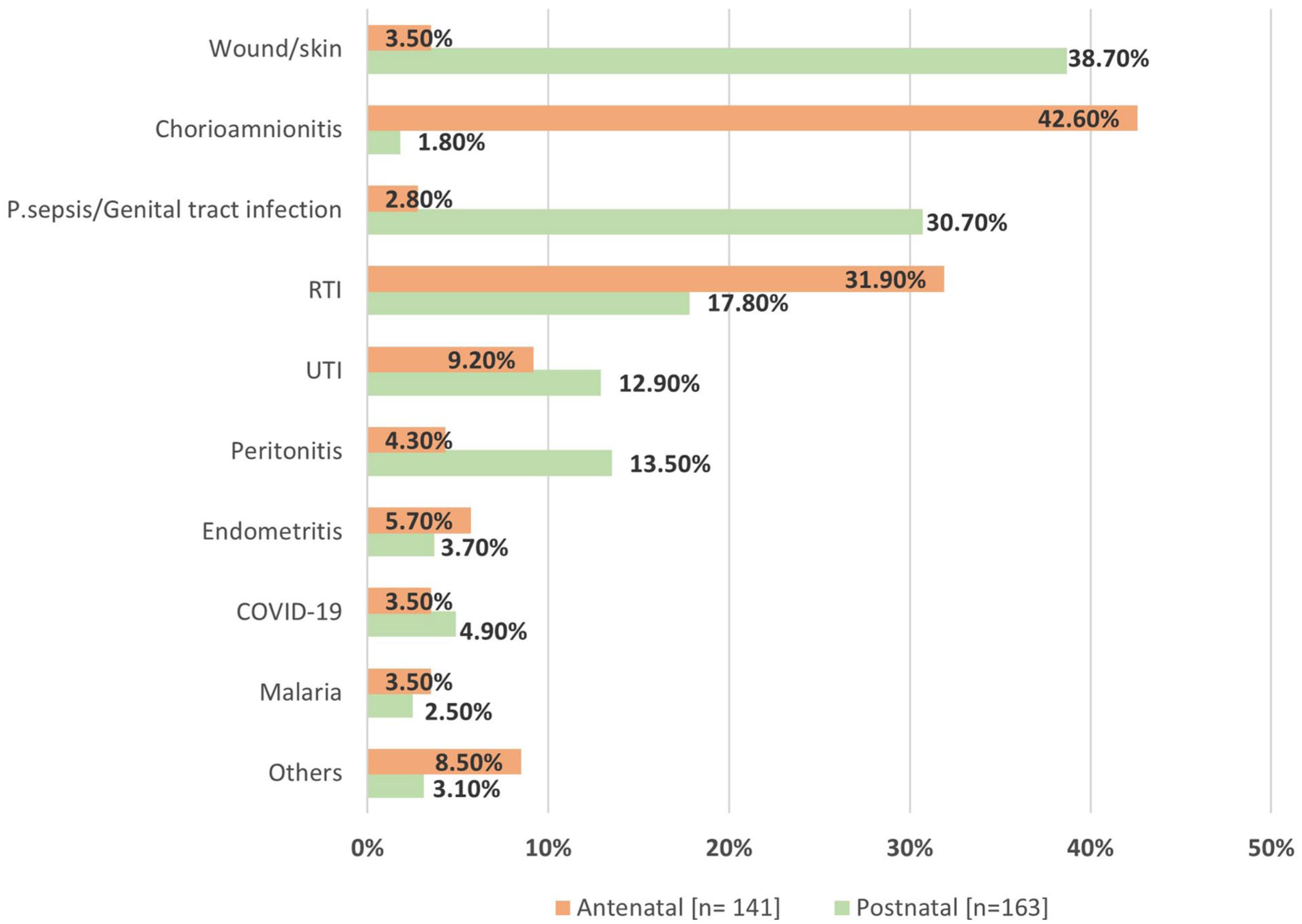
Primary source of infection according to admission status.
The most common maternal complication developed by the 439 patients in the study was the need for blood transfusion (118 patients, 26.9%). Other complications included return to the theatre (37, 8.4%), changes in mental status (32, 7.3%), reduced urine output (11, 2.5%), and pulmonary edema (10, 2.3%). Thirty-three patients (7.51%) were transferred to high levels of care including intensive care units and high dependency units. Most of the patients transferred had RTIs (21, 63.63%). Organ dysfunction was seen in 13.9% of women, with the highest numbers being cardiovascular (42.6%) and neurological dysfunction (40.9%). A total of 19 maternal deaths (4.32%) were reported in the study population. Among these, in 12 women (3.2%), a single source of infection was identified, while 7 of these women (1.8%) had multiple sources of infection. Women with any two organ dysfunctions accounted for the greatest number of deaths. The highest mortality was observed in women who had RTI only (05, 41.66%), followed by wound/skin infections (03, 25%), peritonitis (01, 8.3%), puerperal/genital tract infections (01, 8.3%), and other type of infections (02, 16.66%).
Table 2 presents the pregnancy and neonatal outcomes of enrolled patients according to the severity of their infections. Preterm births were a significant pregnancy outcome in our cohort. The highest number of still births (54/56, 96.4%) and live births (172/353, 48.7%) occurred among women in the third trimester. Neonates born to mothers who had the most severe infections had significantly lower APGAR scores at 5 min (31.8% versus 16.9% in less severe infections, p = 0.006). A higher incidence of suspected infection/sepsis was also noted in neonates born to mothers in this group (7.6% versus 0%, p = 0.043). While differences in neonatal death rates (3% versus 2.6% in less severe infections) and neonatal intensive care unit (NICU) admissions (21.2% versus 15.6%) were not statistically significant, the trend shows worse neonatal outcomes with increased severity of maternal infections. 36.4% of neonates born to mothers with less severe infections had birth weight below 2.5 kg, which is notably high compared to the 12.1% in the infections with complications group (p = 0.0005). Low birth weight was significantly associated with preterm birth (p = 0.020), with the highest percentage of low birth weight due to preterm recorded in the less severe infections category (19.5%).
Pregnancy and neonatal outcomes of patients with maternal infections according to severity.

NICU: neonatal intensive care unit.
Infection related to severe maternal outcome versus less severe infection.
Infection related to severe maternal outcome versus infection with complication.
Less severe infection versus infection with complications.
Discussion
This study paints the most current picture of maternal infections in Pakistan, presenting data from a large public sector hospital on the frequency of maternal infections, sources of infection, and their maternal outcomes and pregnancy and neonatal outcomes categorized by severity of infections.
The observed frequency of maternal infections was 12% in pregnant or recently pregnant women admitted during the study period. The main sources of infection in antenatal women were chorioamnionitis and RTI (Figure 1). This finding is corroborated with a study in India which found that 16.7% of direct obstetric deaths were due to respiratory diseases. 12 In Pakistan, lower RTIs are the second largest cause of mortality among the general population, 13 and our findings reveal that it is commonly found among pregnant women as well. During this study period, there was also an upsurge of COVID-19, which could have affected the occurrence of RTIs. Due to the limited number of testing kits available at public sector hospitals, 14 COVID-19 tests were performed only on critical patients. Therefore, the actual number of COVID-19 positive cases could not be approximated during the study duration, and consequently, we were unable to rule out the COVID-19 cases from the RTIs in our cohort. Poor immunization level of pregnant women in LMICs is another factor behind the prevalence of RTIs. 15
The study did not find any significant difference between the number of antenatal and postnatal women admitted to the hospital, implying that regardless of the stage of pregnancy women are in, they are susceptible to infection. The physiological adaptations the body undergoes during pregnancy leaves women immunocompromised and therefore more prone to infection. 16 Deficiency of micronutrients and vitamins is another risk factor increasing susceptibility to infection, especially in the postpartum period. 17 This is a prevailing issue in Pakistan, with women of reproductive age women having more than one vitamin deficiency. 18 The number of postnatal women being admitted to the hospital highlights the unhygienic nature of the settings where these women delivered, as well as inferring that other hospitals in the surrounding area do not have effective infection prevention guidelines/strategies in place.
As LUMHS is a tertiary care public hospital, providing free-of-charge services, the majority of the underprivileged population in the surrounding rural and urban areas are referred there. Nevertheless, the study found a high number of direct obstetric admissions. This further adds to the previous statement regarding the unsatisfactory quality of the surrounding health facilities which are not meeting the health needs of pregnant women, leaving these women no choice but to come to LUMHS. For some, LUMHS is not in the vicinity either, meaning women have to travel long distances to access care, which can further exacerbate their condition. Delay in accessing care for obstetric complication is known to contribute towards maternal death 19 and may warrant the number of women in the cohort that were transferred to higher care or expired. Direct admissions also bring attention to the lack of knowledge on the importance of maternal health related services, such as antenatal visits. Women in this population are not aware of when to seek medical attention and visit health facilities only when complications develop. Absence of ANC is a persistent issue in other LMICs as well, for example in Bangladesh, where the issue of low ANC attendance was dealt with the introduction of healthcare workers at the rural level, which led to an 89% increase in women receiving more than four ANC visits. 20
Among postnatal women in the study, wound/skin infection, puerperal/genital tract infection, and UTI were observed in high numbers (Figure 1). These results align with findings from an Egyptian hospital, which reported wound infections (29.1%) and UTIs (71.8%) to be the most common sources of infection among postpartum women. 21
The reason behind the high prevalence of wound/surgical site infections could be due to the high rates of C-sections in our sample. It is well-established that postpartum surgical site infections are a major source of postpartum infection among women who have undergone a C-section, ranging from 3% to 15% worldwide. 22 Moreover, the C-section rate in Pakistan is at 22%, 23 despite WHO’s recommendation of an optimal range of 5% to 15%. 24 Thus, the increased prevalence of C-sections among this population, coupled with other factors such as lack of aseptic practices and equipment sterilization when performing procedures, 25 leads to a higher likelihood of surgical site infections developing.
Mode of delivery is a determinant underlying another source of infection in our study, UTIs. A Danish study found that chances of contracting UTI is 36% higher in caesarean delivery over vaginal delivery, due to urinary catheterization, increased hospital stays, and reduced mobility. 26 The high prevalence of caesarean deliveries in Pakistan mentioned earlier, therefore, increases the likelihood of postpartum UTI. In our study, the prevalence of UTIs was higher in postnatal women (12.9%) compared to antenatal women (9.2%; Figure 1); nonetheless, UTIs are a well-documented issue among Pakistani women, with a study revealing 81% of women having a UTI while pregnant. 27 Women residing in underprivileged areas are generally more prone to developing UTIs due to poor hygiene practices carried out by traditional birth attendants, lack of clean water, and delivering in environmental conditions that do not meet the WHO minimum criteria. 28 The high incidence of UTIs can also be accounted for by the high occurrence of women returning to the operating theatre, as UTIs have been found to occur during invasive procedures that are performed in unclean operating rooms. 29
Puerperal/genital tract infections are also common infections that develop in the postpartum period, with a high number of cases reported in developing nations. 30 In Pakistan, the odds of puerperal sepsis are 2.7 times in women who have home births compared to those in a hospital facility. 31 However, even in hospital facilities, if the environment where invasive procedures are occurring are unsanitary, puerperal sepsis-causing infective organisms can be introduced into the body. 32 Our study population primarily belongs to low socioeconomic groups and thus may be more inclined toward home births leading to an increased chance of infections developing. Absence of postnatal checkups in LMICs also leaves puerperal infection unchecked, 33 allowing progression to puerperal sepsis. This is a likely scenario in Pakistan where 36.4% of women and 69.3% of newborns do not receive a postnatal checkup within 6 weeks of childbirth. 34
The neonates in our study had outcomes related to APGAR scores, and suspicion of infection/sepsis strongly associated with maternal infections. Interestingly, a high percentage (36.4%) of low-birth-weight neonates were born to mothers with less severe infections. Although there was no significant difference in neonatal deaths and NICU admissions across the severity groups, the trend of higher neonatal deaths in mothers with infections related to severe maternal outcomes aligns with the results of the GLOSS study. 35
The third group, related to severe maternal outcome, had the highest percentage of low APGAR score at 5 min as well as the highest percentage of suspicion of infection/sepsis. This also aligns with other studies, which revealed that low APGAR score significantly increases chances of sepsis among neonates. 36 Another study showed low APGAR is associated with maternal infections as well. 37 The importance of ANC is raised again with APGAR scores, with an Ethiopian study finding that women who had minimal ANC gave birth to neonates with low APGAR scores. 38
Strengths and limitations
The strength of our study is that it provides a recent picture of the incidence of maternal infections and their subsequent maternal, pregnancy, and neonatal outcomes in a large local healthcare setting in Pakistan. The findings from this study can help provide a basis for future interventional and randomized control studies, in addition to the development of targeted maternal infection programs in the future.
A limitation of our study is that we only gathered data of hospitalized patients during this 7 month period from a single hospital site. However, given the range of patients that were received from the surrounding area, a diverse population was represented so the findings from this study can give some idea on the impact of maternal infections for this province. Another limitation is the inclusion of patients for whom the primary source of infection could not be identified during the hospital stay. They were included based on positive signs of infection and the clinician’s suspicion. Lack of data on confounding variables and various neonatal outcomes was another limitation, arising from the limited access the study team had to the hospital files. Finally, the COVID-19 pandemic also influenced study findings to some extent.
Conclusion
Overall, the findings from this study suggest that maternal infections of all kinds, regardless of severity of maternal conditions, are a major threat to fetal and neonatal outcomes. Good infection prevention and control measures are key to prevent women not only from maternal morbidities caused by maternal infections, but also adverse neonatal outcomes. Maternal and neonatal care can also be improved through the increased presence of skilled birth attendants in underprivileged and remote areas. Prevention of neonatal sepsis can further be achieved through immunization of mothers during pregnancy. Emphasizing antenatal and post-natal care can further prevent infections and their related complications. While prevention is key, detection and management of maternal infections is equally necessary. This can be achieved by introducing early detection and management strategies, which would not only improve the handling of maternal infection but also strengthen the local healthcare system.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251387427 – Supplemental material for Incidence of maternal infection and its related outcomes in a public sector hospital in Pakistan
Supplemental material, sj-pdf-1-whe-10.1177_17455057251387427 for Incidence of maternal infection and its related outcomes in a public sector hospital in Pakistan by Fizza Amir, Bakhtawar M. Hanif Khowaja, Faiza Sattar, Amir Raza, Ramsha Zafar, Raheel Sikandar, Fahmida Parveen, Naheed Parveen, Shazia Rani, Lumaan Sheikh and Sheikh Irfan Ahmed in Women's Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057251387427 – Supplemental material for Incidence of maternal infection and its related outcomes in a public sector hospital in Pakistan
Supplemental material, sj-pdf-2-whe-10.1177_17455057251387427 for Incidence of maternal infection and its related outcomes in a public sector hospital in Pakistan by Fizza Amir, Bakhtawar M. Hanif Khowaja, Faiza Sattar, Amir Raza, Ramsha Zafar, Raheel Sikandar, Fahmida Parveen, Naheed Parveen, Shazia Rani, Lumaan Sheikh and Sheikh Irfan Ahmed in Women's Health
Supplemental Material
sj-pdf-3-whe-10.1177_17455057251387427 – Supplemental material for Incidence of maternal infection and its related outcomes in a public sector hospital in Pakistan
Supplemental material, sj-pdf-3-whe-10.1177_17455057251387427 for Incidence of maternal infection and its related outcomes in a public sector hospital in Pakistan by Fizza Amir, Bakhtawar M. Hanif Khowaja, Faiza Sattar, Amir Raza, Ramsha Zafar, Raheel Sikandar, Fahmida Parveen, Naheed Parveen, Shazia Rani, Lumaan Sheikh and Sheikh Irfan Ahmed in Women's Health
Footnotes
Acknowledgements
We would like to acknowledge the healthcare practitioners, nurses, and hospital staff at LUMHS hospital for their support and assistance in the conduct of this study. We would especially like to acknowledge Ms. Ruqaiya Bano for data collection of this study.
Ethical considerations
Ethical approval for this study was obtained from the LUMHS hospital (REC/-886, 4-87), Aga Khan University Ethical Review Committee (2019-2061-7102) and National Bioethics Committee (515/20/).
Consent to participate
Written informed consent was taken from participants prior to data collection.
Consent for publication
Written informed consent was taken from participants prior to data collection regarding findings being shared.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available as Supplemental Material submitted with manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.