
Abstract
PURPOSE:
The current study’s aims were to (1) examine long-distance walking ability (6-minute walking test [6MWT]) and walking hemodynamic responses (i.e., heart rate) among youth with functional neurological symptom disorder (FNSD) before and after an integrative pediatric rehabilitation (IPR) program; and (2) explore factors predicting improvement in walking ability.
METHODS:
Thirty-one youth with FNSD participating in an IPR program were recruited. The IPR program was activated biweekly in an ambulatory format. Study measures included the 6MWT, hemodynamic characteristics, rate of perceived exertion (RPE), pain-intensity perception, and Child’s Somatization Inventory-24 (CSI-24). All measures were conducted upon admission to the IPR and discharge.
RESULTS:
Findings indicated a significant increase in 6MWT distance, as well as decreases in heart rate, RPE, and pain-intensity perception from admission to discharge. At admission, CSI-24 and pain intensity predicted 6MWT distance (adjusted R2 = 0.68). Pain intensity predicted discharge 6MWT distance (adjusted R2 = 0.18). Initial 6MWT predicted changes in 6MWT distance from admission to discharge (adjusted R2 = 0.33).
CONCLUSION:
Using an integrative rehabilitation approach increases walking distance and decreases pain-related symptoms in youth with FNSD, emphasizing the need for collaboration between physical therapists and pediatric psychologists. Moreover, changes in walking ability may increase participation and thus should be the focus of IPR.
Introduction
Functional neurological symptom disorder (FNSD), an impaired voluntary motor or sensory function without a recognized neurological or medical basis, is among the most common diagnoses in neurology practice [1]. With high rates of comorbidities [2, 3], FNSD encompasses several disorders such as those related to movement and gait [4]. Recently, the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5)[5] introduced the term FNSD, assigning the disorder to the category of “somatic symptom and related disorders.”
Treating FNSD is often costly to health services [6]. For example, FNSD has been associated with high levels of treatment costs and health care use, comparable to those for care-intensive neurological disorders [7]. This emphasizes the need to develop effective treatments to improve overall function in patients with FNSD. In addition, FNSD is considered to be composed of a complex interplay between physiological stimuli, alterations in central processing of sensory input [8], and expectation, learning, and misdirected attention in unconscious processes [9]. The aforementioned are mediated through a Bayesian framework, predisposing and perpetuating the various inputs [10].
According to the biopsychosocial framework [11], environmental factors (specifically parental factors) tend to increase a child’s vulnerability to somatic symptoms [12]. For example, parents’ thoughts, illness beliefs, and attitudes toward their child’s complaints, as well as their own physical condition, were found to impact the child’s ability to cope with symptoms. Moreover, parent-child communication (e.g., about symptoms) has been associated with child’s symptoms and functioning [12–14]. Accordingly, parents and other family members all have a crucial role in the management of childhood FNSD [15].
Over the last decade, there has been a growing consensus regarding the advantages of using an integrative pediatric rehabilitation (IPR) approach [16, 17] in pediatric settings. IPR focuses on combining pharmacology, psychology and physiotherapy interventions when treating children with FNSD [18]. However, clinical guidance regarding treatment of children and youth with FNSD, including guidelines for the assessment of treatment effectiveness [20], is sparse [19], although the importance of incorporating objective assessments in physical therapy sessions has been previously acknowledged. The objective assessments may have two components: (1) indirect observation of the child’s functional performance (e.g., abnormal movements), and (2) more traditional objective assessments of physical function to help track progress over time, such as walking tests [21] and cardiovascular responses to walking. High levels of symptom variability are a hallmark of FNSD. This temporal variability is an important issue for objective tests of motor symptoms among individuals with FNSD [22, 23]. Nonetheless, it is recommended to also use objective assessments in physiotherapy to help track progress over time [20]. Moreover, according to a recent systematic review and recommendations on outcome measurement in FNSD, there are few well-validated FNSD-specific outcome measures. Thus, at present, it is recommended to use existing outcome measures known to be psychometrically robust in FNSD or closely related populations. In the current study, the 6-Minute Walk Test (6MWT) was used as it has already demonstrated test-retest reliability within other related populations, such as those with psychological or psychiatric problems that also present high levels of symptom variability [24]. Moreover, the ability to walk for a distance is an inexpensive measure of physical function and an important component of quality of life, as it reflects the capacity to conduct daily activities [25]. Such measures can also provide information about various physiological functions (i.e., the ability to ambulate in the community) [26]. As increased functional activity (a task or act that allows one to meet the demands of the environment and daily life) is often accompanied by increased reports of pain, integrating both physical and psychological determinants associated with pain perception among individuals with FNSD is necessary.
A limited number of studies have used walking ability before and after physiotherapy with standardized gait and/or transfer as outcome measures among individuals with FNSD [27, 28]. A recent randomized feasibility study [29] also assessed, among other things, the effect of physiotherapy intervention among individuals with functional motor symptoms using a 10 meter walk test. The results indicated a medium to large effect size (d ranging from 0.46 to 0.79). However, all of the above studies used a short-distance walking test, a measure that does not fully reflect a more general functional walking capability. In another randomized controlled trial of physical rehabilitation with one-year follow-up [30], significant improvements in gait in functional mobility for 5, 50, and 500 meters were reported. These changes were sustained at follow-up. However, this study included only adult participants (18–62 years old). Within the pediatric population, positive outcomes were described among children with FNSD admitted to an inpatient medical rehabilitation program [31]. At discharge, patients significantly improved in functioning on the mobility subscale of the Functional Independence Measure for Children. In another case report, an adolescent girl (15 years old) with FNSD showed improvement in several function-related outcome measures, including the 6MWT, following interprofessional rehabilitation treatment [19]. However, using the Reliable Change Index metric, improvements in 6MWT scores were not statistically rare (scores did not fall outside of the confidence interval).
From the aforementioned literature it appears that FNSD studies did not commonly assess long-distance walking ability/disability. Accordingly, a scoping review on inpatient treatment of functional neurological disorder by Gilmour et al. [32] reported that the degree of disability was most commonly captured with the Functional Independence Measure (N = 3) and the Modified Rankin Scale (N = 2). In addition, only 7 of a total of 34 articles included in the review reported changes in walking ability.
Factors important for walking distance may be valuable in predicting functional capacity and participation and thus may promote health-related outcomes in children/youth with FNSD. A long-distance walking test such as the 6MWT is of particular importance because it may indicate the capacity to participate in peer-group activities [33, 34], promoting well-being.
The current study’s aims were to examine long-distance walking ability among youth with FNSD using the 6MWT, to examine hemodynamic responses (i.e., heart rate [HR]) before and after an IPR program, and to explore factors predicting improvement in walking ability.
Methods
This study is a clinical care observational study conducted in an ambulatory clinical setting in a children’s hospital in the center of the country, treating youth from the entire country.
Participants
During the period 2017–2019, youth presenting with FNSD were referred to the ambulatory rehabilitation clinic by their primary/secondary care physician after ruling out other somatic causes of the symptoms.
Inclusion criteria
The inclusion criteria included (1) age 6 to 18 years; (2) a diagnosis of FNSD based on the DSM-5 (Conversion Disorder-300.11; FNSD-318) (5); (3) admission to the ambulatory clinic; and (4) exhibition of lower-limb weakness, and/or paralysis or sensation disorder, and/or gait disorders (e.g., abnormal gait pattern) due to FNSD (5). Diagnosis of gait disorders was based on recognition features and gait observation [35]. In addition, according to the recommendations of Gray et al. [21], the assessments were conducted using indirect (i.e., informal behavioral observations) and direct measures. Indirect assessment involved observation by a physical therapist to determine the participant’s functional capacity (e.g., posture, use of limbs, abnormal movements, and signaling of pain) while engaging in a task/game (e.g., tossing a bean bag at a target on the wall 10 times). In the direct assessment, the therapist observed the participant’s gait pattern while conducting the 6MWT, a traditional objective measure of physical function.
Exclusion criteria
Exclusion criteria included (1) pain symptoms with no motor/sensory involvement; (2) exhibition of only upper-extremity disorders; (3) hospitalized at the inpatient rehabilitation department; and (4) other clinical diagnoses that might explain the symptoms.
All study procedures were approved by the Sheba Medical Center Ethical Review Board (7394-20-SMC; May 2020).
Outcome measures
As part of a routine physical and psychological evaluation, all participants completed a comprehensive evaluation battery upon admission (admission evaluation = T0) and discharge (discharge evaluation = T1) from the clinic. According to the International Classification of Functioning, Disability and Health –Children and Youth version (ICF-CY; [36]), the evaluation battery consisted of measures from various domains (personal factors, body function, and activity).
Demographics and medical information
Demographics (age and sex), medical information (pharmaceutical treatment and medical diagnostic tests), and IPR intervention duration were retrieved from medical records.
Somatization symptoms severity
Somatization symptoms severity was evaluated using the Child’s Somatization Inventory-24 (CSI-24) [37]. The questionnaire is composed of a list of 24 symptoms experienced within the past two weeks. Participants were asked to rate the frequency of each symptom on a 5-point scale (0 = not at all; 4 = a whole lot). Two scores were generated: number of symptoms (0–24) and symptoms intensity (0–96), with higher scores indicating higher intensity of somatic complaints. Cronbach’s alpha reported for the CSI-24 was 0.87 [37]. The CSI-24 was administered once, upon admission to the rehabilitation program, to document participants’ severity of somatization symptoms and symptoms’ associations with 6MWT distance.
Walking ability
Walking ability was assessed using the 6MWT [26]. Participants were instructed to walk for 6 minutes as far as they could at a comfortable pace. During the test, participants used their usual assistive devices. Those using a wheelchair could not do the 6MWT and therefore their walking distance in the test was 0 meters. Participants’ walking ability relative to the norm was evaluated by calculating the number of standard deviations (SDs) below the mean according to the norms published by Geiger et al. [38]. Note that high levels of symptom variability are a hallmark of FNSD [22, 23]. Nonetheless, it is recommended also to use objective assessments in physiotherapy [21]. Thus, at present, it is recommended to use existing outcome measures known to be psychometrically robust in FNSD or closely related populations, such as the 6MWT [24].
Hemodynamic characteristics
Resting, exercising, and recovery HR were measured using a Polar S810 watch. Exercising HR was measured immediately upon completion of the 6MWT. Participants’ predicted maximal HR was calculated using Tanaka’s maximal HR equation (208 –0.7×age) [39] and was converted to percentage of maximal HR. Exercising at 50% to 70% of the maximum HR is considered moderate exercise intensity, and exercising at > 70% is considered vigorous exercise intensity [40].
Rate of perceived exertion (RPE)
RPE was evaluated at the end of the 6MWT using the OMNI Walk/Run RPE (OMNI-RPE), which consists of a series of four pictures of a child walking up a hill and looking progressively more tired. The OMNI-RPE has been validated for typically developing children/youth ages 8 to 18 years [41–43].
Pain intensity
Pain intensity was evaluated before and after the 6MWT using a numerical pain rating (NPR) scale ranging from 0 (no hurt) to 10 (hurts like the worst pain imaginable) [44]. Patients with chronic pain prefer the NPR scale to other measures of pain intensity because of its comprehensibility and ease of completion.
All outcome measures were assessed both at T0 and T1 except for the CSI-24, which was evaluated only at T0.
Procedures
IPR program
The IPR program was activated biweekly in an ambulatory format and involved treatment by the Pediatric Rehabilitation Department multidisciplinary team including physiotherapy, occupational therapy, psychological therapy for children and parents, and educational courses. The program’s goals were returning patients to age-appropriate functioning, minimizing recurrence of symptoms, and improving parent-child interaction. In addition, family meetings (child/youth and parents) with the entire clinical staff were conducted weekly. These meetings aimed at reviewing the previous week’s achievements, setting physical rehabilitation goals, and modeling parent-child direct communication. Note that the country where the study was conducted is small, and even people who do not live very close to the hospital managed to attend the sessions, minimizing selection bias. In addition, the treatment program included an educational team, and, upon arrival, all patients were academically assessed. Following family’s consent, the educational team received information from school teachers about the subjects currently studied, and preferred subjects were chosen to minimize academic gaps due to missing days at school. For some patients, return to school was delayed since undetected learning disabilities arose, and new adapted learning was required.
The key discharge factor was the return to age-appropriate activity and participation (e.g., school attendance). For additional information about IPR, see Gerner et al. [45].
Physiotherapy
Physiotherapy was conducted twice a week. Each treatment session lasted 45 minutes. The first one to three sessions emphasized getting to know the child (e.g., behavior) and developing a rapport. During that phase, as described by Nielsen et al.’s [46] consensus recommendations for physiotherapy practice for functional motor disorders, one goal was for the child/youth to understand that their treating health professionals acknowledged that their problems are genuine (i.e., not “made up” or “imagined”). In addition, this “get-to-know” phase focused on the “ill use” of the affected limb, engaging in daily activities, and beginning various exercises. Exercises were accompanied by psychoeducation explaining the reason for the recommended activity. After the first three sessions, in addition to the individual sessions, each child was assigned to group therapy with specific exercises tailored to their impairment and activity limitations. A combination of aerobic and functional exercises was gradually presented.
During the weekly meetings, the child was encouraged to present continuous progress. The progression pace incorporated principles from the field of motor learning, specifically focusing on providing less physical support and verbal cueing, and more intrinsic feedback [47]. Moreover, the treatment progressed via short- and long-term goals, selected jointly by the child and the physiotherapist during weekly meetings.
Each patient was given up to three home exercises adapted to their individual ability and engagement level, for example, bridging laying on mattress/bed; shifting weight while sitting/standing; and specific exercises to strengthen the weak limb (e.g., straight leg raising). The number of repetitions was discussed with the patient during the weekly meetings. The home exercises were considered homework and part of the program. The child was responsible for self-administration and was asked to report progress or difficulties during the training. A key principle of the physiotherapy was to compliment the child for their efforts and not for their success. For example, therapists did not comment about an abnormal gait pattern. Instead, they provided positive reinforcement of correct movement patterns. Another key principle was the clinical team’s approach to pain and pain intensity. In contrast to the pain-exposure approach [48], during exercise, the child was not asked about the level of pain or asked to perform against higher levels of pain. Instead, they were asked to participate and perform at their best comfort level.
Statistical analysis
Changes from pre- to post-intervention (T0 and T1, respectively) were examined via paired t-tests. 6MWT distances at T0 and T1 were also presented graphically using box plots. Changes from T0 to T1 in 6MWT distance were examined via Cohen’s d effect size (ES) (mean Δ/SD average of two means) [49]. A correction for the dependence among means was conducted using the correlations between the two means following Morris and DeShon’s equation [50]. In general, values≤0.20 are considered trivial ESs, values between 0.20 and 0.50 small ESs, values between 0.51 and 0.80 moderate ESs, and values > 0.80 large ESs [49]. Variables associated with 6MWT distance at T0, T1, and change from T0 to T1 in 6MWT distance were examined using Pearson correlation coefficients. Finally, three separate forward multiple stepwise regression analyses for factors predicting T0 6MWT distance, T1 6MWT distance, and change from T0 to T1 in 6MWT distance were conducted. Only variables significantly correlated with the dependent variables were included. All independent variables were checked for multicollinearity using the variance of inflation factor > 10 [51]. The criterion for inclusion in the model was an alpha level of 0.05, and for exclusion was an alpha level of 0.10.
Power analysis for the mean difference between the two dependent means was conducted using the observed sample ES (post-hoc power analysis). Power analysis was conducted using G*Power 3.0.10 [52]. In all statistical analyses, p-values lower than 0.05 were considered to indicate statistical significance.
Results
Study participants
A total of 42 children/youth with FNSD were screened for eligibility. A total of 11 were excluded; thus, 31 participated in this study (Fig. 1; mean age = 13.75 + 2.71). P ost-hoc power analysis showed that when using the ES of change observed in the study’s primary outcome measure (6MWT distance) with a sample size of 31, the power of the t-test was 0.81. In addition, in the regression analyses, only a maximum of two predictors were entered. Post-hoc power analysis for multiple regression shows that for the study’s primary outcome measures with two predictors, the power achieved is greater than 0.80.
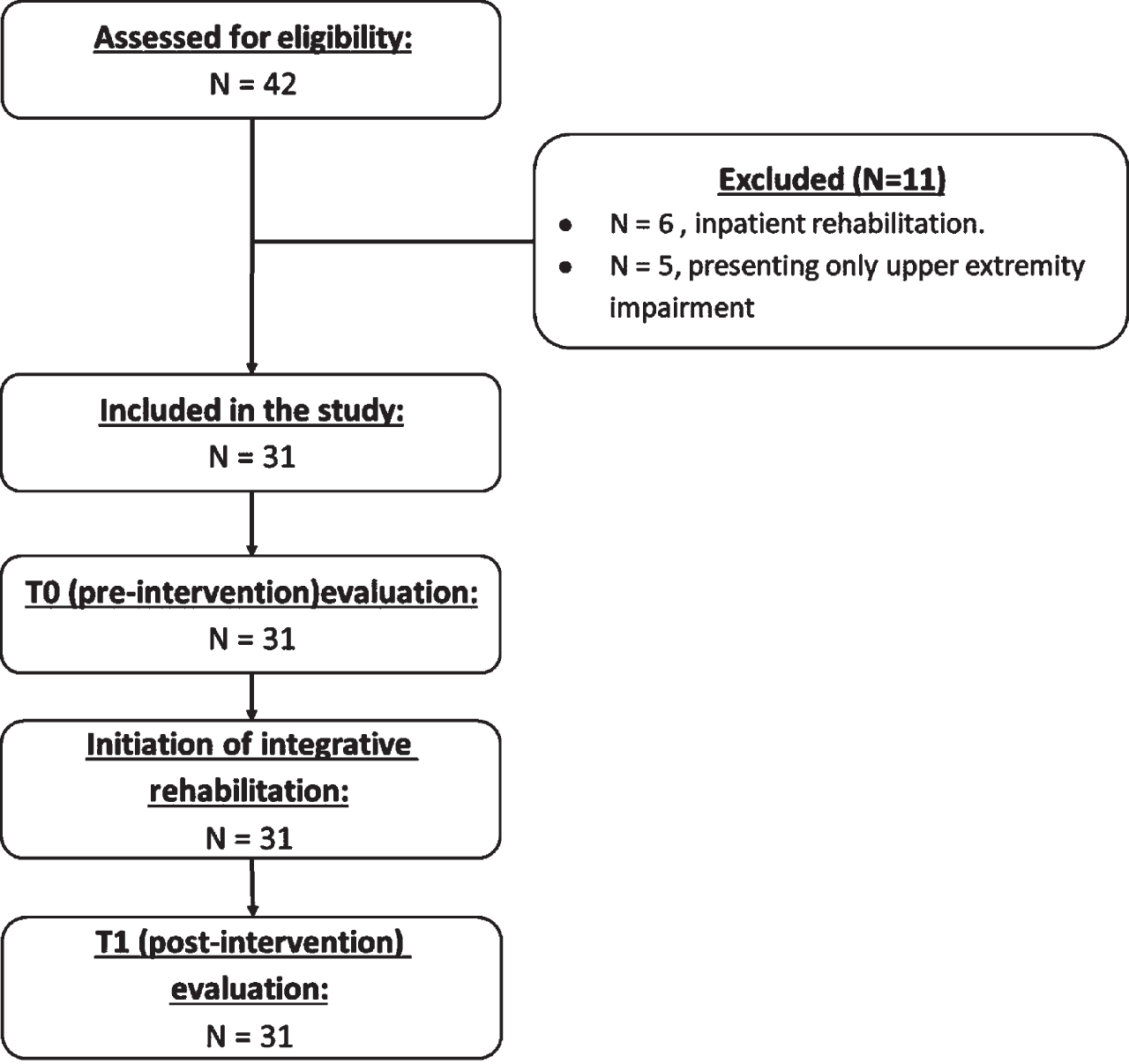
Flow chart of study design.
The mean number of symptoms in CSI-24 was 13.42 (3.59). All study participants had a gait disorder and most of them presented with pain (n = 27, 87%). In addition, most study participants walked without aids (n = 18, 58.06%); 22.58% (n = 7) walked with a walker/crutches, and 19.35% (n = 6) used a wheelchair. For description of study participants’ demographics and clinical characteristics, refer to Table 1.
Demographic and clinical characteristics of study participants (N = 31)
Notes: †Child’s report; SD, standard deviation.
Figure 2 shows that walking distance in the 6MWT at T0 varied considerably. In addition, from T0 to T1, participants significantly increased their walking distance (ES = 0.53). Accordingly, 6MWT SD from the norm significantly decreased (Table 2). Overall, 64.50% of participants increased their walking distance by at least 1SD; 35.40% did not achieve such improvement (chi-squared = 4.12; p = 0.04).
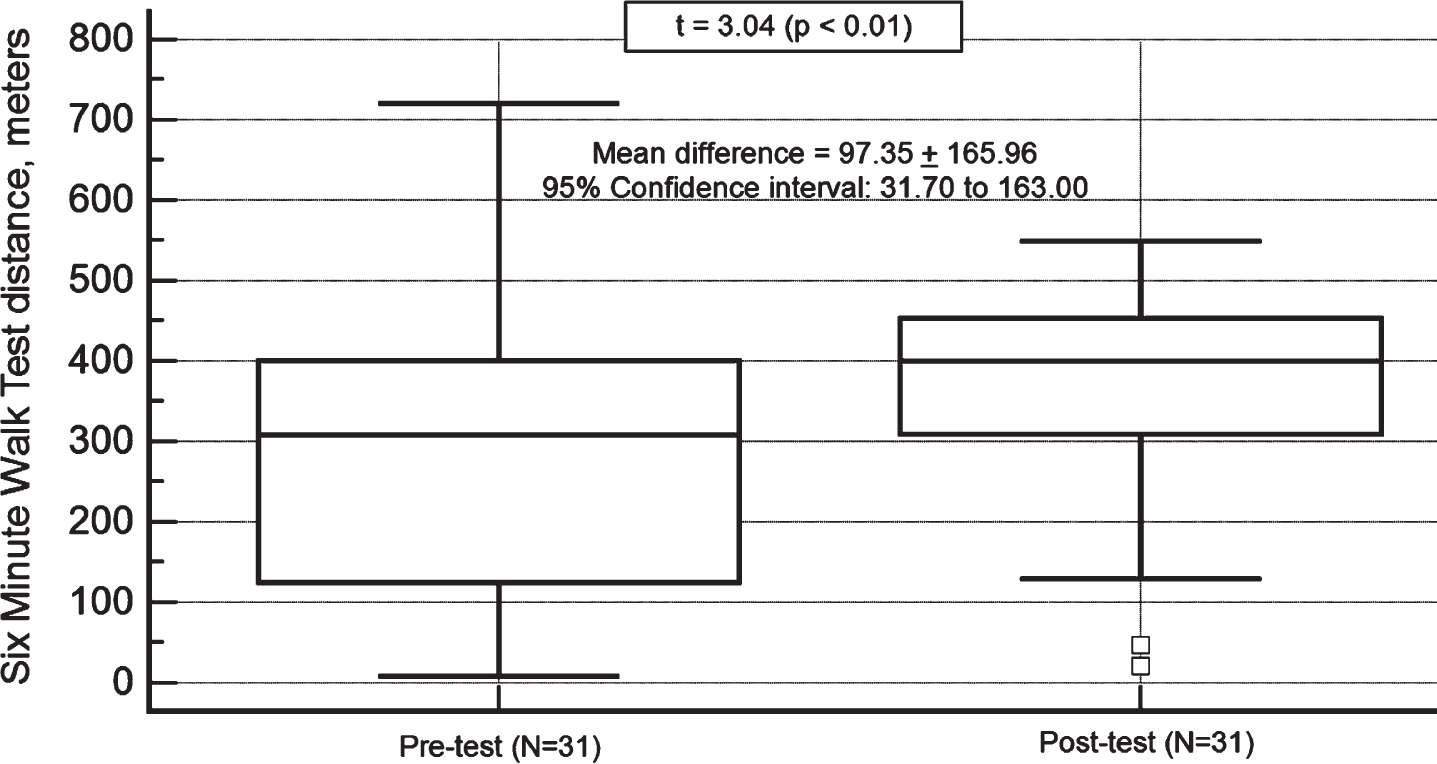
Changes in 6-Minute Walk Test distance. Note: the central box represents the values from the lower to upper quartile (25th to 75th percentile); effect size = 0.55; the vertical line extends from the minimum to the maximum value, excluding outside values. An outside value is defined as a value that is smaller than the lower quartile minus 1.5 times the interquartile range, or larger than the upper quartile plus 1.5 times the interquartile range; the middle line represents the median.
Changes in walking ability and exercising and pain intensity perception (N = 31)
Note: *Significant differences at the p < 0.01 level, 2-tailed (paired sample t-test); 6MWT, 6-minute walk test; CI, confidence interval; SD, standard deviation; T0, pre-intervention; T1, post-intervention; NPRS, Numeric Pain Rating Scale; 6MWT walking distance and heart rate measurements are graphically illustrated in Figs. 2 and 3.
Figure 3 shows that at T0 and T1, participants’ T1 6MWT HR ranged from light-to-vigorous intensity, with no significant changes in percentage of HR maximum. However, recovery HR, a physiological measure of cardiovascular fitness, decreased from T0 to T1 (p < 0.05). Changes from T0 to T1 were also observed in OMNI-RPE and pain-intensity perception before and after the 6MWT (Table 2).
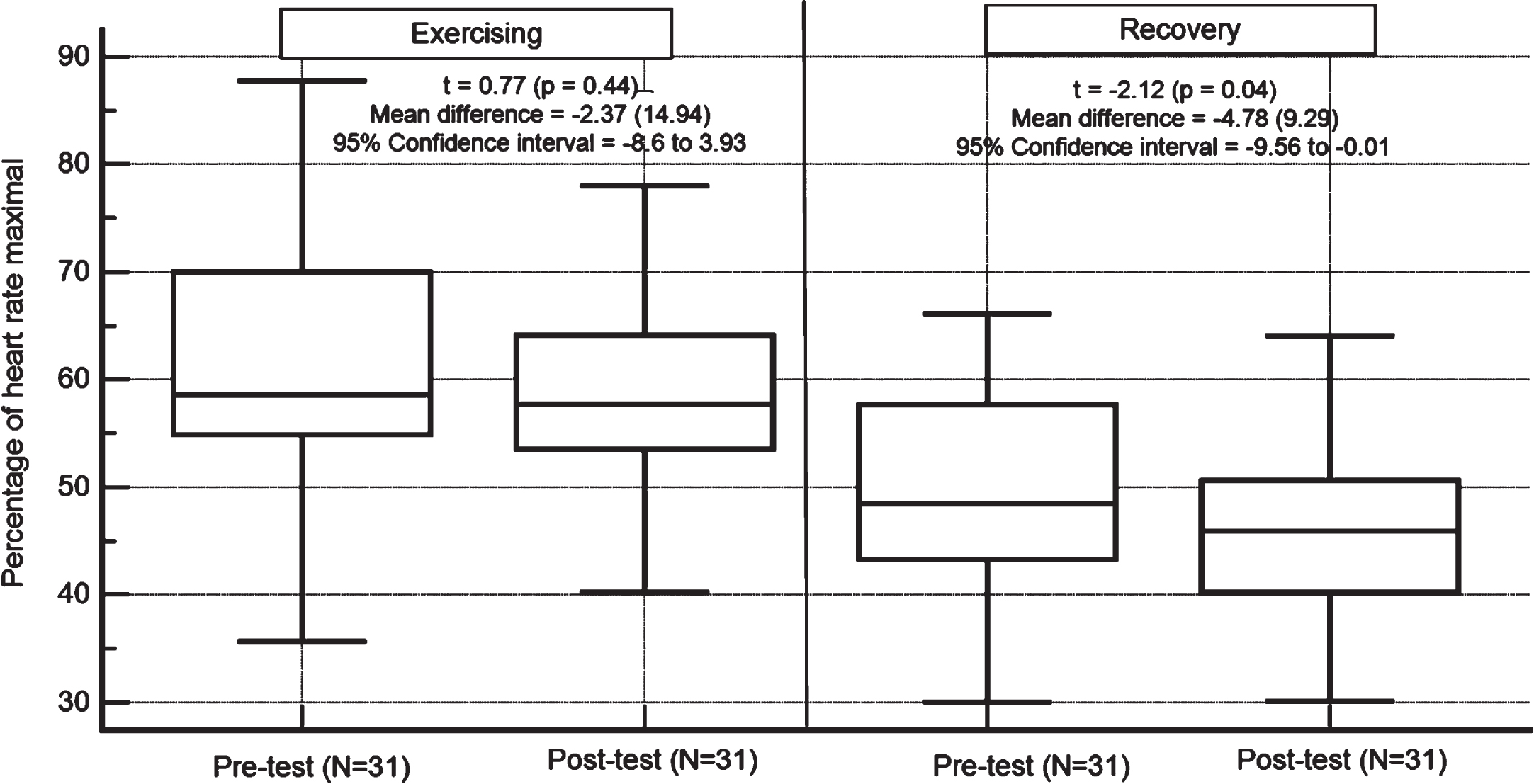
Changes in exercising and recovery percentage of maximal heart rate. Note: *significant differences from pre- to post-test; effect sizes: exercise and recovery effect sizes = –0.20 and –0.59, respectively; the central box represents the values from the lower to upper quartile (25th to 75th percentile); the vertical line extends from the minimum to the maximum value, excluding outside values. An outside value is defined as a value that is smaller than the lower quartile minus 1.5 times the interquartile range, or larger than the upper quartile plus 1.5 times the interquartile range; exercising at > 70% of maximal heart rate is considered vigorous exercise intensity (40).
At T0, 6MWT distance was significantly correlated with the number of symptoms reported on the CSI-24 (r = –0.84; p < 0.01) and with pain-intensity perception before and after the 6MWT at T0 (–0.59 and –0.44, respectively; p < 0.04; Table 3). Because there were high correlations between pain-intensity perception before and after the 6MWT (r = 0.85; p < 0.01), only the before pain-perception scores were entered into the regression model. The model showed that the number of somatic symptoms at T0 and pain-intensity perception at T0 both predicted T0 6MWT distance (adjusted R2 = 0.68; F-ratio = 27.13; p < 0.01; Appendix 1).
Variables related to walking ability - Pearson correlation coefficients (N = 31)
Variables related to walking ability - Pearson correlation coefficients (N = 31)
Note: * Significant correlations at the p < 0.01 level (2-tailed); †Child’s report; 6MWT, 6-minute walk test; CSI, Children’s Somatization Inventory; HR, heart rate; NPRS, Numeric Pain Rating Scale; T0, pre-intervention; T1, post-intervention.
At T1, 6MWT distance was predicted by pain-intensity perception at T0 (ß= –0.42; p < 0.05; Table 3; Adjusted R2 = 0.18; F-ratio = 6.32; p = 0.01; Appendix 1).
Changes from T0 to T1 in 6MWT distance were negatively associated with the child’s number of symptoms (r = –0.49; p < 0.05) and with T0 6MWT distance (r = –0.69; p < 0.05; Table 2). However, only the latter predicted changes observed in 6MWT distance (adjusted R2 = 0.33; F-ratio = 21.41; p < 0.01; Appendix 1).
The current study explored long-distance walking ability of youth with FNSD participating in an IPR program. The results highlight the positive changes in performance in this ability among study participants following physiotherapy as part of an IPR program. Currently, there is limited research examining the effect of IPR on functioning of children and youth with FNSD [19, 53]. However, the effect of such interventions has been examined in other pediatric populations, such as children with chronic headaches [54].
Participants in the current study significantly increased their walking distance from T0 to T1. This finding aligns with previous findings among individuals with chronic pain conditions (e.g., fibromyalgia) who participated in an integrative treatment program and experienced improved functional status compared with a control group receiving conventional pharmacologic treatment [55]. However, in comparison to population norms, the 6MWT walking distances at T0 and T1 in the current study were significantly low, indicating that participants did not reach normative levels of functioning in terms of physical capabilities.
The partial recovery in age-appropriate walking capability observed in the current study may be supported by imaging studies in children with complex regional pain syndrome [56]. This is cited here because complex regional pain syndrome research may enhance mechanistic understanding of FNSD [57]. For example, during active pain, stimuli to the affected limb produced a greater level of positive blood oxygen level-dependent activations than stimuli to the unaffected limb [58]. Erpelding et al. [59] also showed that, compared with controls, children with FNSD had reduced activity in motor-system-related brain areas such as the gray matter in the primary motor cortex. Interestingly, in the asymptomatic state (i.e., symptoms clinically resolved), there were still significant differences in the central nervous system responses after stimulation of the affected and the unaffected limbs, especially involving regions in the frontal and parietal lobes, insula, and basal ganglia [60]. The aforementioned brain areas all have important roles in generating movements [61–63]. Moreover, as these regions’ function is altered in the asymptomatic state, it may partially explain the reduced walking ability of study participants at T1. More specifically, considering the available literature, it is reasonable to assume that despite the improvements seen in participants’ somatic symptoms (i.e., reduction of pain intensity perception), the function of motor-related areas in the brain remains altered and therefore may be partially accountable for the reduced performance on the 6MWT.
Another important finding was that age and cardiovascular-related fitness measures in the sample did not predict 6MWT distance at T0. This finding is in contrast to previous findings in healthy children, in which age was considered one of the most prevalent predictors of 6MWT walking distance [64]. In the current study, only FNSD-related factors, as measured by the number of symptoms and pain-intensity perception, predicted 6MWT distance at T0. These findings indicate that, unlike in healthy children, physiological factors such as aerobic capacity do not significantly contribute to the variability in 6MWT distance among children and youth with FNSD. This has practical implications for physical rehabilitation programs, suggesting that cardiovascular fitness is probably not a major component in the IPR, and that pain and symptom perception should be further addressed. Moreover, standard musculoskeletal approaches to physical therapy may exacerbate symptoms because they are unresponsive to the biopsychosocial context in which FNSD emerges. For example, in FNSD, symptom presentations are often intensified by psychological factors. Therefore, a key principle of any physical therapy for children and youth with FNSD is to communicate that the symptoms are genuine and understood. Moreover, it is recommended that therapists address the child’s maladaptive patterns of behaviors during therapy, such as thoughts and states of high arousal that might trigger pain-related symptoms [21]. In addition, improvements observed in the current study might also be directly related to exercising. For instance, according to Gray et al. (2020) [21], exercising by itself is valuable because it might prevent long-term physical complications, activates the motor system in healthy ways, promotes learning, helps switch off the pain system, regulates the autonomic nervous system, and so forth. From the aforementioned literature, it is apparent that physiotherapy for children and youth with FNSD has unique characteristics. However, physiotherapists surveyed about their exposure to and attitudes toward patients with functional (psychogenic) motor symptoms reported that inadequate service structures, knowledge, and support from non-physiotherapy colleagues are barriers to provision of care [65].
Another important finding was that despite the increase in walking distance, pain-intensity perception before and after the 6MWT decreased. This finding may be associated with one of the program’s key features, i.e., working toward improving function without directly asking the child about their pain intensity during sessions. This finding is supported in previous studies indicating that in adults with chronic pain, attentional biases toward pain-related information may facilitate a focus on symptoms and pain [66]. In children and youth, in addition to possible pain-related attentional bias, parents’ attentional biases may also play a role in shaping a child’s responses to contextual threats and pain [67]. This factor of parental attentional bias may have an important influence on a child’s pain perception (i.e., pain-intensity perception) and behavior [68]. Thus, the reduction in pain-intensity perception observed also may be attributed to the IPR program, which includes both physical and psychological treatments, with a strong emphasis on parental acceptance of the child’s progress even in the face of pain. For example, in the physiotherapy sessions, the child was taught to notice physical signs from their body (e.g., to “listen” to their body sensations). In the psychological sessions, parents and children/youth learned to recognize the body-mind association, linking emotional distress with physical symptoms, thus gradually acquiring the ability to express emotional distress verbally (e.g., verbalize fears). This process was supported by the focus on improving their communication skills. Eventually, it is possible that because of the focus on family communication in the study’s IPR program, the attention of both the child and parents shifted from a focus on physical symptoms and pain to a mechanism aimed at resolving emotional distress and improving function and participation [59].
Another important strength of the study is its use of child self-report measures. The literature indicates that self-report measures have often been underutilized in assessing children’s pain [69]. Therefore, examining children’s pain perceptions in relation to functional level (e.g., walking ability) is of special interest. Further, this study has good external validity, as children/youth from the entire country were treated in a clinical setting as part of routine treatment for children/youth with FNSD. Moreover, the duration of the IPR program was neither predetermined nor limited by external factors. More specifically, the key discharge factor was the return to age-appropriate activity and participation.
Limitations
This study was subject to several limitations. First, despite the robust ES, the relatively small sample requires further examination of the contribution of an integrative rehabilitation approach to FNSD in children/youth on activity and pain-intensity perception levels. Furthermore, the lack of a control group may affect the ability to inquire about the unique contribution of the IPR to the level of symptomatology and functioning among children/youth with FNSD. The lack of a control group, however, is in line with ethical considerations. More specifically, according to the World Health Organization [70], control conditions must be justified, and researchers must ensure that they do not deprive participants of effective care or programs to which they would have access. As participants in the current study presented with FNSD, which limited their participation in age-appropriate activity, having a control group not receiving IPR (which has proved to be beneficial [45]) might be unethical. Lastly, the current study did not include additional self-reported measures regarding disability/function nor mental-health status. Such information is in line with the biopsychosocial approach and is significant as it may improve understanding regarding the holistic experience of children/youth with FNSD and support the holistic multidisciplinary treatment programs tailored to their individual needs.
Conclusion
The study’s results indicate a clear improvement in participants’ walking ability, RPE, and pain-intensity perception from T0 to T1. However, relative to norms, participants’ walking ability remained considerably lower. Variables related to FNSD severity predicted T0 walking ability. However, only the perception of pain intensity at T0 predicted walking ability at T1. Given that the relationship between pain and function is not linear, it would be inaccurate to assume that changes in pain will correlate with changes in function. Additional research is needed to better understand how interventions may specifically address non-pain outcomes in FNSD such as function. This perspective is compatible with the ICF-CY [36] framework, which views a child’s body function, activity, and performance not only in terms of a “medical” or “biological” dysfunction but rather as composed of the child’s physical and psychological environment. Moreover, as psychological factors such as FNSD severity (i.e., CSI-24) and pain perception are all related to and predicted walking ability, a collaboration between physical therapists and pediatric psychologists in the IPR for youth with FNSD is required [71]. Finally, the information collected in the current study using different measures and different settings (medical, physical, and psychological) will help enhance collaboration between the child, their parents, and the clinical staff, and support their engagement in providing effective rehabilitation interventions.
Footnotes
Acknowledgments
We thank the children/youth and their parents/guardians for their participation in this study.
Conflict of interest
The authors have no conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.