
Abstract
PURPOSE:
The Wii Balance Board (WBB) can be used for assessment of steady state balance (SSB), but its reliability has not been studied in children aged 6–9 years. This study aimed to determine the test-retest reliability of the WBB for measuring SSB in this population. A secondary aim was to determine the minimum detectable change (MDC) and standard error of measurement (SEM) of the WBB in children aged 6–9 years.
METHODS:
52 children between 6–9 years of age participated. “One leg stand balance” was used to assess center of pressure velocity (COPV) and center of pressure area (COPA) on three occasions by the same tester. Two tests were conducted on the same day (Day 1) and the third test was performed on another day (Day 2), with a period of 5–13 days between the two test days. Intraclass correlation coefficient (ICC 3,1), SEMs, and MDC were calculated.
RESULTS:
Intra-day test-retest reliability of COPA was found to be good (ICC3,1 =0.86; 95% confidence interval [CI]: 0.75, 0.92) and that of COPV was also found to be good (ICC3,1 =0.87; 95% CI: 0.77, 0.92). Inter-day test-retest reliability was found to be good for COPA (ICC3,1 = 0.87; 95% CI: 0.75, 0.93) and COPV (ICC3,1 = 0.89; 95% CI: 0.81, 0.94). SEM for COPA in intra-day testing was 18.90 mm2 (15.78%), and in inter-day testing it was 16.44 mm2 (13.61%). SEM for COPV in intra-day testing was 1.12 mm/s (7.6%), and in inter-day testing it was 1.01 mm/s (6.9%). MDC for COPA in intra-day testing was 52.41mm2 (42.75%), and in inter-day testing was 45.58 mm2 (35.75%). MDC for COPV in intra-day testing was 3.11 mm/s (21.2%), and in inter-day testing it was 2.80 mm/s (18.9%).
CONCLUSION:
The WBB has good test-retest reliability for assessing SSB of children between 6-9 years. COPA measurements appear to be less sensitive to clinical changes in SSB when compared to COPV. Assessment of validity of the WBB in this age group is recommended before it can be considered as a potential balance assessment tool in children.
Introduction
Motor control is an important predictor of a child’s cognitive skills, general health behavior and participation in physical activities [1–3]. Balance is one of the important factors for normal motor development along with muscle strength, endurance, body mass index (BMI) and physical activity [3, 4]. Steady state balance (SSB) is the ability to maintain the projected center-of-mass (COM) within the limits of the base-of-support (BOS) and has often been called “static balance.” However, the term ”static balance” is misleading as the amount of postural sway varies in quiet sitting or standing [5]. Several methods of detecting early balance problems have been used in the past [6, 7], but balance assessment of children remains complex and includes assessment of proactive/reactive SSB. Standardized tools such as “Motorisk Perceptual Udvikling” (Motor Perceptual Development [MPD]) [8] and Movement Assessment Battery for Children-2 (Movement ABC-2) [9] have been used for measurement of various developmental parameters including balance [10, 11]. However, the reliability and validity of MPD has been shown to be low [12] and Movement ABC-2 is considered subjective [13]. In addition, the balance domain of Movement ABC-2 has been reported to have questionable test-retest reliability (intraclass correlation coefficient [ICC] = 0.66) in addition to significant differences between two sessions [14].
Force platforms are considered the golden standard [15] for measurement of SSB in adults and children [16, 17]. A force platform measures the postural sway in standing position by measuring the center of pressure area (COPA) and center of pressure velocity (COPV) amongst other parameters. However, it is has been used mostly for research purposes because of its high cost, the time required for testing, and training requirements [18]. Therefore, there is a need to explore alternative objective, reliable and valid measures for SSB.
One of the emerging tools for SSB measurement is the Nintendo Wii Balance Board (WBB), which is a part of a videogame developed in 2005. The WBB was first reported as a potential balance measurement tool in 2009 [19]. Subsequent studies on its reliability and validity showed good to excellent within-device (ICC = 0.66–0.94) and between-device (ICC = 0.77–0.89) center of pressure (COP) test-retest reliability [18]. The WBB has four pressure sensors that collect information about COP and transfer the raw data to a software via Bluetooth [20]. The WBB is easy to use, transportable and considerably economical in comparison to force plates, and therefore it has the potential to be used as a balance assessment tool by clinicians. A Danish company has developed a software for the WBB called Fysiometer®, which allows the WBB to measure SSB. Limited studies conducted on Fysiometer® have shown good reproducibility for the WBB (minimum detectable change [MDC]: 26.5–28.6%, ICC: 0.76–0.83) and good validity (ICC: 0.74–0.87) for SSB measurements in children aged 10 to 14 years [21].
It is well established that children have lower postural stability, and the underlying reasons proposed are immaturity of the involved sensory systems, underdevelopment of integration between sensory systems, and lower degree of intersegmental coordination reflected in a hampered head stabilization [22]. Reliability of the WBB for measuring SSB has not been studied in children under 10 years of age. Considerable differences in concentration, motivation [18, 23], and static and dynamic balance as well as lower body weight of children under the age of 10 years necessitates that reliability of the WBB is established separately for this age group. Accordingly, this study was designed with the main aim of assessing the test-retest reliability (intra-day and inter-day) of the WBB for measuring SSB in children aged 6-9 years. A secondary aim was to determine the MDC and standard error of measurement (SEM) of testing to facilitate clinical interpretation of change over time.
Methods
Research design
This study was a repeated measures reliability study.
Study participants
A total of 68 grade 1 and 2 students from an ordinary Danish public school were invited to participate in the study. An information meeting for parents and teachers was arranged following which informed consent letters were sent to the parents. Parents of 58 students consented for their child to participate (22 students from grade 1 and 36 from grade 2). A sample size of 50 was considered to be adequate for a reliability study [24].
The following inclusion and exclusion criteria were used:
Inclusion criteria age between 6–9 years independence in activities of daily living
Exclusion criteria inability to run forwards and backwards on a 4 meter track inability to understand five oral instructions required for testing limited communication skills in the Danish language any reported painful musculoskeletal condition of the lower limb or the spine which could interfere with normal standing error in three or more of the first six test attempts of a single leg balance test inability to perform the two tests within the test period of 14 days
Six participants were excluded: one based on age, two due to illness, and three because of errors in three or more of the first six test attempts of a single leg balance test. Ultimately, 52 participants were included.
Ethical considerations
The study was designed in accordance with the Danish Code of Conduct for Research Integrity (Ministry for Higher Education and Science, 2014) and the ethical principles outlined in the Helsinki Declaration (World Medical Association, 2013). Internal Review Board approved the study as it was considered as a non-interventional study and did not require approval from the National Scientific Committee. Prior to testing, the participants were introduced to the testers, the aim of the study, the test procedure and the expected performance in a child-friendly manner. No participant was left alone at any point of time during the test sessions.
Statement of informed consent
Informed consent and baseline information was obtained using a standard form from parents of participants.
Test instruments
The WBB in combination with Fysiometer® was used for SSB measurements [20]. Data was collected at a frequency of approximately 100 Hz from each transducer and transferred via Bluetooth to a computer. A 4th order Butterworth filter with a cut-off frequency of 20 Hz was used to remove undesired frequencies. The Fysiometer® software can calculate mean sway ellipse area (COPA) in mm2 and mean sway velocity (COPV) in mm/s. Fysiometer® was originally developed with a test duration of 30 seconds, which was modified to 10 seconds for this study in accordance with normative data on 6-9 year old children’s ability to stand on one leg [5]. This duration for single leg testing has also been used in previous studies [25, 26]. The WBB manual mentions a lower limit of 3.2 kg [20] but preliminary testing by placing a variety of known loads at different positions on the WBB in combination with Fysiometer® revealed a minimum input of 10 kg.
Additional test materials used were marking tape for placement of the balance board on the floor, a red circular piece of cardboard 5 cm in diameter as a focal point on the wall, and a 5 m measuring tape. For the warm up protocol, a 4 m-long track marked with tape and cones was used. For participants’ engagement during wait time, a small play area was set up.
Test protocol
Test protocols of previous studies with outcomes of COPA and COPV in young people provided some inspiration for the development of the protocol [15, 27]. However, a new protocol, which included a warm up program for this age group, was developed. The developer of Fysiometer® trained authors of this study. After the initial training, the main tester continued to test many volunteers before recording actual measurements for this study. It was ensured that clothing for all participants were similar to each other to minimize the effect of clothing on proprioceptive input.
The same tester conducted the testing on three occasions to assess the test-retest reliability. Test 1 and Test 2 were performed on Day 1, and Test 3 was performed on Day 2. These three tests are referred to as Day 1 Test 1, Day 1 Test 2, and Day 2 Test 3 (Fig. 1). Day 1 Test 1 and Day 1 Test 2 were used to assess intra-day test-retest reliability, and Day 1 Test 1 and Day 2 Test 3 were used to assess inter-day test-retest reliability. There was a maximum gap of two weeks between Day 1 and Day 2. The tester received help from two authors in conducting the warm up program and reaction game, entering the demographic data and engaging the participants during waiting periods.
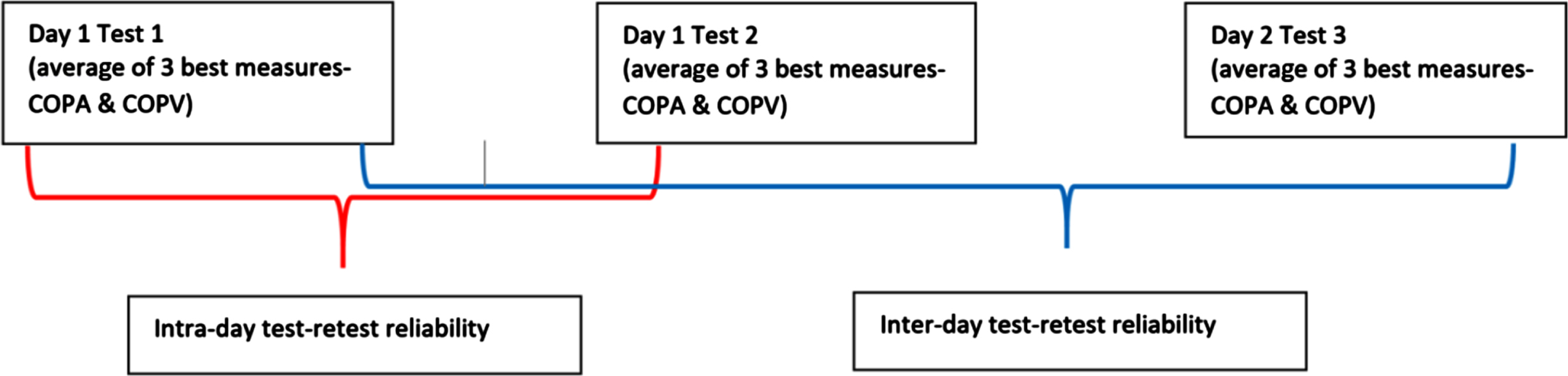
Illustration of testing sessions for intra-day test-retest and inter-day test-retest reliability of center of pressure area (COPA) and center of pressure velocity (COPV) using the Wii Balance Board.
Step 1: Participant preparation
Participants were taken to the gym in batches of 3-4 and were made to wear loose shorts or skirts to avoid sensory inputs from tight-fitting clothing [28, 29]. Warm up and testing were conducted barefoot to eliminate the effect of shoes on balance [30, 31].
Step 2: Collecting demographic characteristics
Age, height, gender and leg dominance of the participants were entered in Fysiometer®. Body weight was registered by the WBB. Dominant leg was identified by asking the participant to kick a football. If the leg preference was not obvious, the participant was asked to perform a single leg hop and the preferred leg was registered as dominant.
Step 3: Warm up
A standardized warm up program [29] comprised the following: Forward and backward running on a 4 m track for 1 minute. Cross body movements in the form of “skier” and “jumping jacks”. A reaction time game on the WBB immediately before the balance testing.
Dynamic warm up has been shown to have positive effects on reaction time [32] and has been used in the past in different age groups prior to balance testing [33, 34]. The authors agreed on the use of three exercises for the participants before balance testing on the WBB to minimize exclusions due to errors in testing.
Step 4: Positioning and focus
The test area was set up in a corner of the gym to minimize audio-visual disturbances. The WBB was placed at a distance of 2 m from a white wall. A red circular sticker adjusted to the eye level of each participant was used as a focal point on the wall. Participants were allowed to keep their hands on the waist, crossed on the chest, abducted to 90 degrees or side to side [35], and they were instructed not to move their arms during testing. The arm position was documented so the participant attained the same position during all three testing sessions.
Step 5: Testing and Data Collection
The participant was introduced to the WBB, and the system was calibrated without load at the start. The tester performed one test up to failure to show COP movement and instructed the participant to keep the COP in the center of the screen as much as possible. After one trial, the screen was turned in another direction. The purpose of providing this visual feedback to the participant in the beginning was to ensure that the child understood the testing process and expectations during the test.
The “one leg stand balance” function was used to measure COPV and COPA for 10 seconds as described by Duarte [36]. The test was considered a failed attempt and repeated if the lifted leg touched the floor or the WBB, or if the foot of the non-weight bearing leg touched any part of the weight bearing lower limb. The participant was given the following instructions: (a) “Stand on one leg on the WBB, as still as you can, until I ask you to stop” (10 sec); (b) “Keep looking at the red mark on the wall;” and (c) “Do not speak during the test period.” The rater stood behind the participant during the entire test period as a safety measure [18]. For ethical reasons, the test was repeated on both legs so the child would not feel demotivated if the performance on one leg was poor. However, only measurements on the pre-established dominant leg were used for analysis even if a measurement from the non-dominant leg was among the three best measurements. Verbal encouragement during the tests was given for optimal performance [37], and children were allowed to see their results after the test.
Data analysis
Data was analyzed using IBM SPSS statistics v24.0. An average of the three best out of nine COPA and COPV measurements from the pre-established dominant leg were used for data analysis. ICC 3,1 and 95% confidence intervals (CIs) were calculated for relative reliability of the WBB. ICC 3,1 represents a two-way mixed effects model and was chosen according to guidelines suggested by Koo and Li [38]. Bland-Altman plots were used for assessing 95% limits of agreement (LOA). SEM was calculated using the formula
SEM is an index of the precision of the test [40]. SEM was used to calculate the MDC using the formula
Results
Demographic characteristics
A total of 52 participants with an average age of 8 years and 4 months participated in the study. Twenty out of 52 students were from grade 1 with an average age of 7 years and 5 months, and 32 were from grade 2 with an average age of 8 years and 11 months (Table 1).
Demographic data of participants
Demographic data of participants
*Standard deviation.
Table 2 shows the COPA and COPV data with means, SD, SEM and MDC of the three tests performed on Day 1 and Day 2.
Center of pressure area (COPA) in mm2 and center of pressure velocity (COPV) in mm/s of the three test sessions
Center of pressure area (COPA) in mm2 and center of pressure velocity (COPV) in mm/s of the three test sessions
*Standard deviation; **Confidence interval.
The interpretation of ICC is based on guidelines for interpretation by Koo and Li [38], and the reliability coefficients are presented in Table 3. Intra-day test-retest reliability of COPA was found to be good (ICC 3,1 =0.86; 95% CI: 0.75, 0.92) and that of COPV was also found to be good (ICC 3,1 =0.87; 95% CI: 0.77, 0.92). Inter-day test-retest reliability was found to be good for COPA (ICC 3,1 = 0.87; 95% CI: 0.75, 0.93) and COPV (ICC 3,1 = 0.89; 95% CI: 0.81, 0.94).
Intraclass correlation coefficients (ICCs) with 95% confidence intervals (CIs), standard deviation of grand means (SD*), standard error of measurement (SEM) and minimal detectable change (MDC) of center of pressure area (COPA) and center of pressure velocity (COPV)
*Standard Deviation of Grand Means; ** Intra-day test-retest reliability; ***Inter-day test-retest reliability; ****The percentages of SEM and MDC are reported as percentages of grand means.
The 95% LOA of the Bland-Altman plot indicate good to excellent agreement for intra-day and inter-day test-retest reliability of COPA (Fig. 2) and COPV using the WBB (Fig. 3).
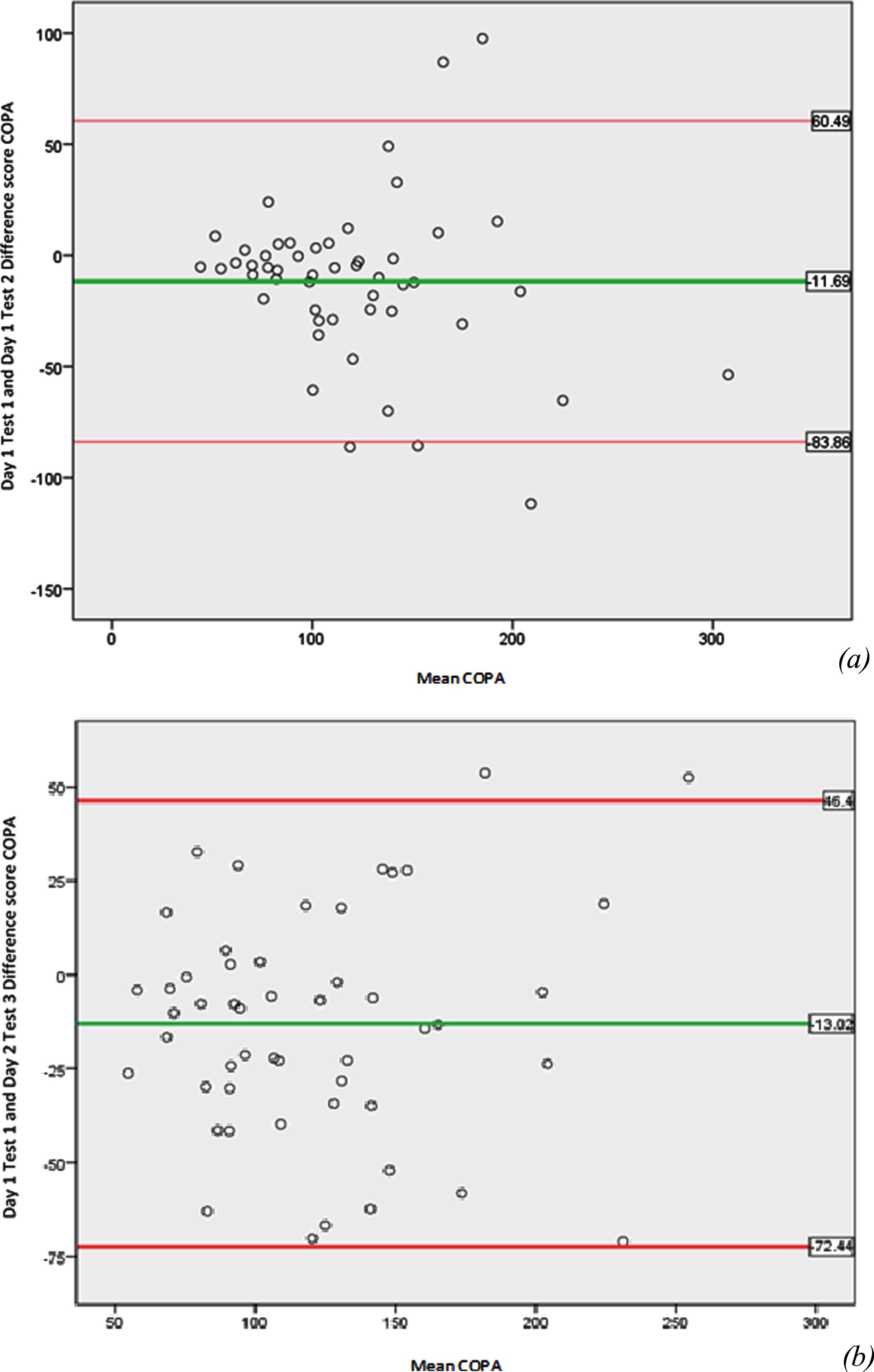
Bland-Altman plots for (a) intra-day test-retest reliability and (b) inter-day test-retest reliability of center of pressure area (COPA) using the Wii Balance Board.
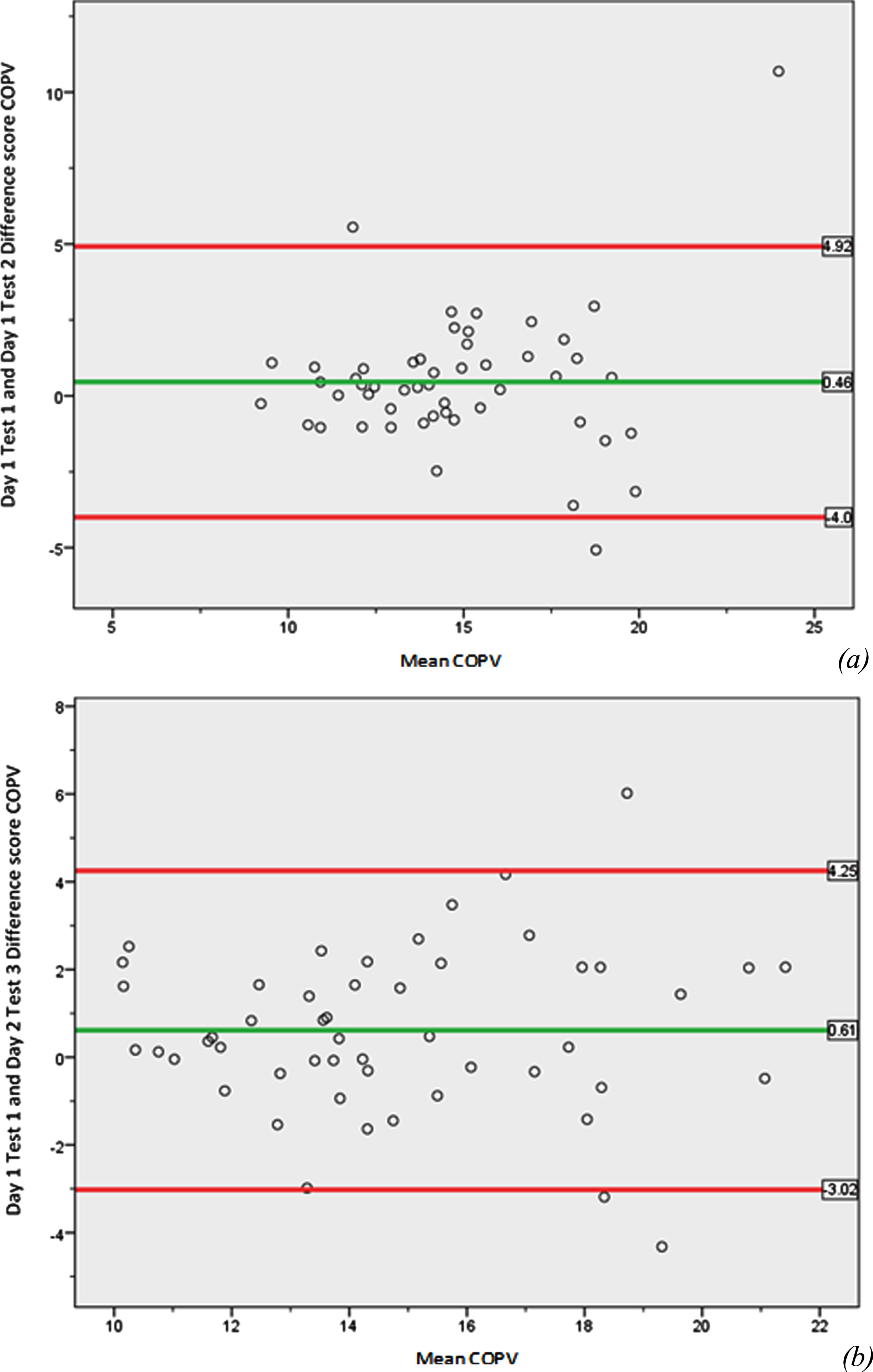
Bland-Altman plots for (a) intra-day test-retest reliability and (b) inter-day test-retest reliability of center of pressure velocity (COPV) using the Wii Balance Board.
SEM for COPA using reliability coefficient from intra-day testing was found to be 18.90 mm2 (15.78%), and SEM using inter-day testing was 16.44 mm2 (13.61%). SEM for COPV using reliability coefficient from intra-day testing was found to be 1.12 mm/s (7.6%), and SEM using inter-day testing was found to be 1.01 mm/s (6.9%). MDC for COPA using SEM from intra-day testing was found to be 52.41mm2 (42.75%) and that from inter-day testing was 45.58 mm2 (35.75%). MDC for COPV using SEM from intra-day testing was found to be 3.11 mm/s (21.2%) and that from inter-day testing was 2.80 mm/s (18.9%). The average time between Day 1 and Day 2 was 5.5 days with a range of 3-13 days.
Reliability of the WBB for assessing balance in children between 6-9 years has not been studied previously, and this study is one of the first to provide reliability measures of the WBB as a balance measurement tool for this age group. Test-retest reliability (intra-day and inter-day) of the WBB were found to be good for COPV and COPA measures [38], which is in accordance with previous studies conducted on adults [18, 43]. Furthermore, the results are also consistent with previous studies which assessed test-retest reliability of the WBB on multiple sclerosis patients (ICC = 0.84) [44] and Parkinson’s disease patients (ICC = 0.96) [45].
A study conducted by Martinez-Lemoz [46] assessed test-retest reliability of the WBB for assessing standing balance in young people with intellectual disability and reported that the variable that achieved the highest ICC was COPA (ICC = 0.76-0.99 for two subgroups). In spite of differences in the testing protocols and age groups in these studies, the WBB appears to be stable with repeated COP measurements.
SEM of COPA ranged from 13.61% (inter-day testing) to 15.78% (intra-day testing), which are lower than previously reported values for COPA measures conducted on the WBB and force platforms [47]. The MDC indicates the minimal amount of change that can be interpreted as a real change in SSB [48, 49]. In this study, the MDC of COPA was 42.75% (inter-day testing) and 35.75% (inter-day testing), which is comparable to previously reported MDC estimates of 21-44% in adolescents and adults [21, 50]. The results of the MDC indicate that large differences in COPA will be needed in a test-retest to detect a significant change in performance. Previous studies have reported that the WBB systematically overestimates COPV and COPA [18], and therefore studies to establish normative data in this age group are needed.
Commonly used force platforms can provide data on COP parameters such as COPV, 95% ellipse area, COP excursion in X and Y axis, total COP excursion length and average radial displacement amongst other variables. The WBB can provide only COPV and COPA values, which is a limitation, but previous studies have used COPV and COPA as measures of postural control [51, 52]. Given that COPV and COPA are reflective of SSB, the WBB has the potential to be used as a clinical tool for screening for balance deficits in view of its low cost and ease of use.
It has been proposed that postural strategies during SSB of children are different than those of adolescents and adults [53], which has the potential to affect the reliability of the WBB when used for balance measurements in different age groups [26]. In addition, it is likely that the lower body weight of children can affect the SSB measurements gathered using the WBB. The lower limit of weight inputs for the WBB was previously mentioned as 16 kg [18], but in this study, it was found to be 10 kg. This discrepancy can be attributed to the difference in the type of software used in combination with the WBB. A study by Clark et al. [18] in which the lower limit of weight input was found to be 16 kg used custom-written software (Labview 8.5 National Instruments, Austin, TX, U.S.A.) whereas Fysiometer® was used in this study. It is likely that the lower limit of 3.2 kg mentioned in the WBB manual is the lower limit only when used as a videogame with its original software. This reveals another issue that the software used in conjunction with the WBB should not be changed for repeated measurements and compatible software needs more standardization. Considering that Fysiometer® is a relatively new software that can be used with the WBB and the fact that SSB can fluctuate considerably in this age group, it was decided that the test-retest reliability should be investigated for repeated measures on the same day and on different days. The assessment of intra-day and inter-day test-retest reliability has increased confidence in the stability of the software used in conjunction with the WBB and SSB performance of children when tested on the same day and on different days.
Reliability of the WBB in the age group of 6-9 years is important to consider before it can be used for screening for SSB deficits. To the authors’ knowledge, only one study conducted to date has assessed reliability of SSB measurements using the WBB in children aged 10-14 years [21], which also reported good to excellent reliability. The protocol required several modifications to make it suitable for use on children in this age group. Communication with and handling of this age group needed a careful approach to avoid confusion and stress. It was decided that the test should be performed on a single leg as earlier studies have used this procedure for testing SSB [18]. Tandem standing could have been considered as a testing position, but earlier research has not shown a significant difference in reliability when comparing these two positions [18]. Similar controversies exist regarding testing with open and closed eyes and placement of the hands [18]. Studies that measured SSB with open and closed eyes did not show that visual condition had a significant effect on reliability [21, 54]. To minimize exclusions, participants were tested with open eyes and were allowed optional placement of their arms, the latter of which was chosen so the children could focus more on the balance testing procedure. Although arm positioning has the potential to affect the measurements, it was ensured that the chosen arm position was the same for each participant in all four tests. This study used one leg standing balance on the dominant leg using a leg preference determination method of kicking a ball. With a measurement time of 10 seconds, the authors felt the need to choose the dominant leg to avoid issues with any further time reduction in the duration of testing. It should be noted that differentiation between dominant leg and preferred leg itself has been questioned, and it has been shown that the preferred leg can show some differences in static balance [55].
It is possible that the four participants who were excluded based on three or more errors in the first six test attempts were distracted or disinterested. However, since completion of the tests was important to assessing the reliability of the WBB, these participants had to be excluded. The warm up program was included in the testing protocol with the intention of enhancing overall performance [32] of one leg standing ability and avoiding exclusions due to inability to complete the test. A study by Verschueren [56] showed that acute physical fatigue can impair performance of dynamic activities such as single leg hop but had an insignificant effect on Y balance test. Therefore, the authors are of the opinion that the relatively short duration warm up program used in this study is unlikely to affect the balance performance negatively.
The time between Day 1 and Day 2 varied between three days to two weeks, which is consistent with previous studies that assessed the reliability of the WBB [25, 50]. This duration avoids learning bias and significant motor development, which can potentially affect repeated measures. The authors suggest that a duration of 10 seconds and an average of the three best measures are more feasible in children given their short span of focus. In spite of relatively controlled conditions, the level of concentration and pressure of performance are factors that can affect static balance performance in this age group considerably and must be taken into account when planning future research in this area.
It is evident from the results that means of COPA and COPV increased slightly over the test period, suggesting reduced balance. This indicates that the negative impact of diminished concentration and motivation due to repeated measurements was actually larger than the learning effect.
Although the WBB can be a promising tool for SSB assessment, the issue of whether SSB is an indicator of dynamic control remains. Several studies have examined the association between steady state and proactive/reactive balance and have suggested that SSB is not completely representative of proactive/reactive balance [57, 58]. In addition, it is important for healthcare professionals to discuss and decide whether the WBB should be utilized as a clinical tool for measuring the effect of motor control interventions or whether it should be used exclusively as a screening tool for differentiating children with SSB deficits for further motor control assessment. Studies assessing validity and responsiveness of the WBB in children are required to answer these questions and further strengthen the case for clinical use of the WBB for SSB measurements.
Conclusion
The WBB has good to excellent test-retest reliability for assessing SSB of children aged 6-9 years. However, validity of the WBB for balance assessment of children aged 6-9 years needs to be assessed before the WBB can considered as a potential balance measurement tool for this age group.
Footnotes
Acknowledgments
We are extremely thankful to all children who participated in this study. We are also grateful to the school authorities and parents of these children who gave their consent for their children’s participation. We also thank our colleagues who provided their insight and expertise during the course of this project.
Conflict of interest
The authors have no conflicts of interest to report.
Funding
The study received funding from University College Absalon, Denmark.