
Abstract
PURPOSE:
To examine the effect of age on postural control outcomes among patients being seen during their initial post-concussion clinical visit.
METHODS:
Youth patients were seen≤14 days post-concussion, and completed a series of postural control evaluations: tandem gait, Romberg, and Balance Error Scoring System (BESS) tests.
RESULTS:
We included 109 children 8–12 years of age (24% female, evaluated median = 7 [interquartile range = 4–10] days post-injury) and 353 adolescents aged 13–18 years (36% female, evaluated median = 7 [4–10] days post-injury). There was a higher proportion of children who demonstrated abnormal tandem gait relative to adolescents (26% vs. 11%; p < 0.001). They also made more BESS errors in single (median = 5 [2–10] vs. 4 [2–6] errors) and tandem (median = 3 [1–6] vs. 2 [0–4]) firm stances. After covariate adjustment, children demonstrated worse tandem gait (adjusted odds ratio = 3.05, 95% CI = 1.68–5.53) and more firm surface BESS errors (double stance β=0.51, 95% CI = 0.22–0.80; single stance β= 1.18, 95% CI = 0.42–1.95; tandem stance β= 0.98, 95% CI = 0.28–1.68) than adolescents.
CONCLUSIONS:
Tandem gait and BESS performance following concussion differ in children compared to adolescents who present within 2 weeks of injury. Clinicians assessing and managing concussion should recognize age differences in postural control performance when assessing those with concussion.
Abbreviations
Balance Error Scoring System Health and Behavior Inventory Modified Balance Error Scoring System Child Sport Concussion Assessment Tool
Introduction
Presently, there is less evidence examining concussion management strategies and assessing outcomes among children compared to adults [1]. Previously, researchers have compared young adult to adolescent populations [2–4], yet few outcome comparisons exist between adolescents and their younger counterparts under the age of 12. The 5th International Consensus Statement on Concussion in Sport indicated that children 12 years and under likely require special paradigms for assessment and treatment. However, the lack of studies within this population reduces the ability to provide evidence-based recommendations [5]. As a result, studies of younger children should be a research priority [5]. Recent multi-site work has found that symptom reporting behavior is similar between adolescents and younger children but that varying symptom profiles between age groups may help to discern symptom recovery prognosis [6]. Self-reported symptom profiles represent a valuable component of concussion evaluations. However, there may be added value in distinguishing the effects of concussion related to age through the use of objective measures.
Existing studies that have examined outcomes following sports-related concussion among children under age 13 have focused primarily on the number of symptoms and symptom severity scores [7–9], rather than more objective, performance-based clinical outcomes that measure physiological functioning. Specifically, there are many ways that clinicians assess function following concussion using methods such as tandem gait assessment [10], Balance Error Scoring System (BESS) test [11], near point of convergence assessment [12], or King Devick Test administration [13]. Although each of these techniques is commonly used by clinicians, their utility among younger children with concussion remains poorly understood. Using the Child Sport Concussion Assessment Tool (SCAT) among a large cohort of uninjured children 5–13 years of age, Brooks and colleagues observed that younger athletes (ages 5–7) made more modified BESS (mBESS) errors and had longer tandem gait times when compared with children over age 7 [14]. This study’s strength was the large number of patients aged 5–13 years old. However, no comparisons were made to adolescents older than 13 years of age or to a cohort of participants who had sustained a recent concussion. Thus, whether postural control differences exist on a multifaceted set of clinical measures between different age groups after a concussion have yet to be determined.
In order to ascertain whether concussion evaluation strategies among children should differ from adolescents following sport-related concussion, a study was conducted which examined clinical postural control test performance amongst children and adolescents who recently sustained a concussion. The primary purpose of this study was to cross-sectionally examine the effect of age group (children vs. adolescents) on postural control outcomes when assessed within the first 14 days of a concussion. It was hypothesized that children 6–12 years of age would demonstrate more postural control abnormalities (e.g. more BESS errors, greater proportion of tandem gait and Romberg test abnormal tests) relative to adolescents 13–18 years old.
Methods
Study design and participants
Data were obtained from patients seen between January 1, 2015 –August 31, 2017 at the Children’s Hospital Colorado Sports Medicine Center for evaluation of a potential concussion. The data was collected as a part of a prospective clinical registry of children and adolescents with concussion. Patients were included if they were ≤18 years of age and presented to clinic for evaluation within 14 days of injury. Patients were excluded if they sustained a concussion from a non-sports-like related mechanism, had trauma-related pathology on neuroimaging, or returned for care following a second head injury prior to full recovery from the index concussion. All patients were diagnosed with concussion using a definition consistent with Berlin guidelines [5] by a board-certified sports medicine physician. Upon being seen for their initial evaluation, variables were collected as a part of the clinical registry. Patients were then followed according to their individual clinical needs until symptom resolution, return-to-play clearance, or referral to a specialist. Prior to conducting this study the local institutional review board approved the protocol.
Grouping variable: Age
The primary grouping variable was patient age. Age was calculated as a continuous variable as the difference in days between date of injury and date of birth and converted to years dividing by 365.25. Consistent with the recommendations provided by the 5th International Consensus Statement on Concussion in Sport [5], patients were then grouped into the following age categories: 8–12 years of age (children), 13–18 years of age (adolescents).
Clinical evaluation
During the initial clinical evaluation, several medical and injury history variables were obtained. These included time elapsed (days) from injury until clinical evaluation, the presence of loss of consciousness (LOC) at the time of injury, self-reported prior history of diagnosed concussion, pre-injury diagnosis of attention-deficit/hyperactivity disorder (ADHD), anxiety disorder, and migraine headaches or headache disorder. Furthermore, data were also obtained pertaining to post-injury variables that included the presence of a headache at the time of the initial clinical evaluation, Health and Behavior Inventory (HBI) [15] rating at initial clinical visit, symptom resolution time in days, and number of days to return to full athletic participation. The HBI is a 20-item scale that measures the frequency of different concussion-related symptoms. All participants, both the child and adolescents groups, completed the child version of the HBI, without assistance from the physician but with assistance from their parent if needed, by rating the frequency of symptoms experienced on a 4 point Likert a scale from 0 (never), 1 (rarely), 2 (sometimes), and 3 (often) [15]. The total symptom score was then calculated as the sum of all items, where higher scores indicate a greater symptom burden.
Balance Error Scoring System (BESS)
The postural control battery for all patients included the BESS, the tandem gait test, and the Romberg test [10, 16]. During the BESS, patients stood in three different stances: with their feet together (double leg stance), on their non-dominant foot (single leg stance), and with their feet positioned where the non-dominant foot was placed directly behind the dominant foot (tandem stance). Foot dominance was determined by the foot patients would kick a soccer ball with. Patients completed each of the three stances while standing on two different surfaces: floor (firm surface) and medium density foam (foam surface). The three stances were performed with hands on hips and eyes closed for 20 seconds each. The primary outcome variable for the BESS is the number of errors made by the patient in each stance condition. Errors were assigned for specific behaviors including opening eyes, lifting hands off hips, lifting the heel or forefoot off the testing surface, stumbling or falling, abduction or flexion of the hip beyond 30 degrees, and remaining out of the proper testing position for greater than five seconds [11, 17]. A higher total score indicated worse performance on the test. All tests were administered by certified athletic trainers who regularly perform the test as part of their clinical practice.
Tandem gait
Tandem gait was measured while the patient was not wearing shoes, and in accordance with SCAT-5 guidelines [18]. During the test, the patient was asked to stand behind the starting line with their feet together. In response to a verbal cue, they walked with an alternating heel-to-toe gait in a forward direction down and back along the pathway as quickly and accurately as possible. The primary outcome variable from the tandem gait test was dichotomous: normal or abnormal, rather than the timed version used in recent studies [10, 20]. A normal test was identified by being able to walk without significant loss of balance and to maintain heel/toe contact throughout the test. In addition, excessive upper body movement while the lower extremities successfully completed the task was identified as an abnormal test, as this may indicate exaggeration and symptom feigning.
Romberg test
The Romberg test was performed by having the participant stand, hands at sides or across the chest, feet together such that the left and right medial malleoli were touching while the clinician monitored their stance [16]. Participants were asked to close their eyes after attaining a stationary standing position, and were instructed to maintain balance for 20 seconds. The primary Romberg test outcome variable was dichotomous: normal or abnormal. A normal Romberg test was defined as the patient being able to hold still without significant loss of balance (opening eyes, lifting foot, falling out of position). An abnormal test was defined as loss of balance or exaggerated movement during the test. As with the tandem gait, increased upper body movement while the feet remained still was classified as an abnormal test.
Statistical analysis
Continuous variables were presented using a median [interquartile range], and categorical variables were presented as the number included and corresponding percentage. Potential differences were assessed in patient demographic, injury history, and recovery characteristics using Mann Whitney U and Fisher’s exact tests. Univariable comparisons of the proportion of patients in each age group who demonstrated abnormal tandem gait and Romberg tests using Fisher’s exact tests were performed. Then the number of errors made in each BESS condition between age groups using Mann Whitney U tests were compared. Statistical inferences were not made based on the results of these univariable comparisons.
In order to conduct multivariable comparisons accounting for potential confounding factors, the independent association of patient age group with tandem gait and Romberg test performance was assessed using multivariable binary logistic regression analyses. The outcome variable was abnormal test performance (yes vs. no), the predictor variable was age group, and included covariates were patient characteristics that demonstrated potential significant differences between groups, defined as p < 0.20. A series of multivariable linear regression analyses to examine the independent association between age group and BESS performance was conducted. The outcome variable was number of errors made in each condition, the predictor variable was age group, and the same covariates were included as described in the binary logistic regression models. Furthermore, the association between age group and symptom resolution time was assessed, as well as age and return-to-play time using a multivariable regression model with the same covariates described above.
For each regression model, collinearity was assessed using condition indices and corresponding variance inflation factors. A condition index > 30 was determined to require individual collinearity assessments, which were performed using variance inflation factors. Collinearity between two variables was detected with a variance inflation factor (VIF) > 2.5 [8, 9]. Statistical significance for multivariable analyses was defined as a 95% confidence interval that did not cross one (logistic regression) or did not cross zero (linear regression), and all tests were two-sided. Statistical analyses were performed using Stata version 15 (StataCorp, College Station, TX).
Results
During the study period, 934 patients were evaluated for a potential concussion. The records of 472 patients were excluded after applying inclusion/exclusion criteria. Thus, a total of 462 participants were included in this analysis: 109 (24%) children ages 8–12 years of age and 353 (76%) adolescents aged 13–18 years of age. There was a higher proportion of females, as well as individuals with a prior history of concussion and pre-injury history of migraine or headache in the adolescent age group relative to the child age group (Table 1). In contrast, there was a higher proportion of individuals in the child age group who reportedly experienced LOC at the time of concussion compared to the adolescent age group (Table 1).
Child and adolescent patient group demographic, injury history, and recovery characteristics (median [IQR] or n (%))
Child and adolescent patient group demographic, injury history, and recovery characteristics (median [IQR] or n (%))
†: Data were available for n = 162 and n = 242 patients for symptom resolution time and return to full athletic participation, respectively.
Upon univariable comparison, there was a higher proportion of patients in the child age group who demonstrated abnormal tandem gait test performance relative to those in the adolescent age group (Fig. 1). In addition, patients in the child age group made more errors than the patients in the adolescent age group on each of the firm surface BESS conditions, but not on any the foam surface conditions (Table 2). There was no significant difference between the child and adolescent groups in the proportion of patients who demonstrated an abnormal Romberg test. In the child age group, 16 patients (15%) failed both Romberg and tandem gait tests, while in the adolescent age group, 26 patients (7%) failed both tests. Upon multivariable analysis, the child age group was independently associated with abnormal tandem gait test performance (Table 3) and with more firm surface BESS errors (Table 4). There was no significant association between age group and symptom resolution time (β coefficient = 1.47 [95% confidence interval (CI) = –3.13 –6.09]) or return to play time (β coefficient = 7.90 [95% CI = –1.23–17.0]).
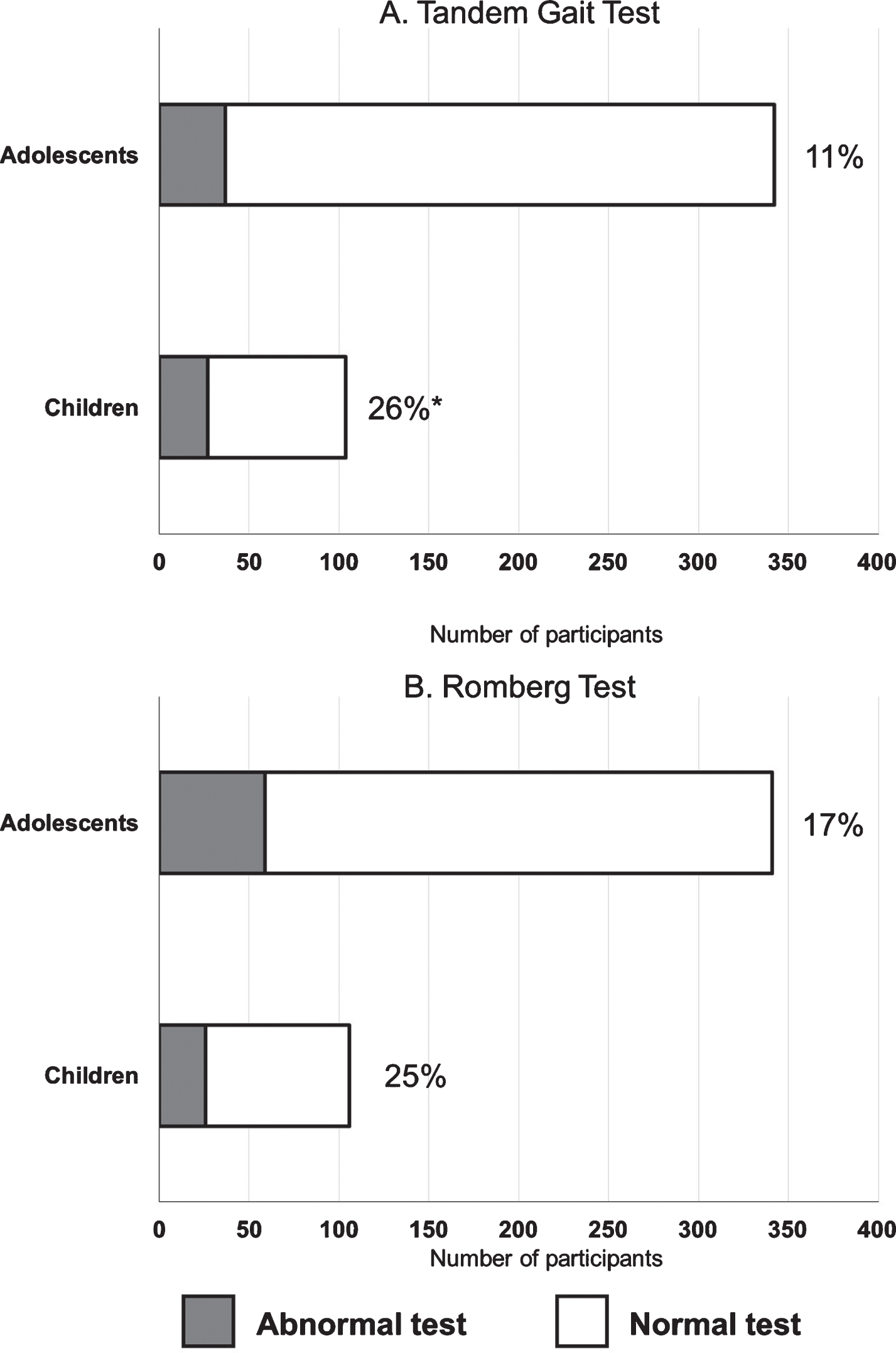
The rate of normal and abnormal tandem gait (A) and Romberg (B) tests for adolescents and children assessed within 14 days of concussion. Percentages indicate abnormal test rates within each group. *There was a significantly higher proportion of children who failed the tandem gait test compared to adolescents (p < 0.001).
The number of errors committed during each of the BESS stances among children and adolescents
The independent effect of younger age on abnormal test performance, adjusting for sex, LOC at time of injury, prior concussion history, and prior migraine/headache history
*Younger age (5–12 years) was independently associated with abnormal tandem gait performance.
The independent effect of younger age on BESS performance, adjusting for sex, LOC at time of injury, prior concussion history, and prior migraine/headache history
*Younger age (5–12 years) was independently associated with more errors in each of the three firm surface BESS conditions.
The primary results from this study suggest that tandem gait performance and BESS errors following concussion differ in children compared to adolescents who present for care to a sports medicine clinic within 2 weeks of injury. Specifically, in this study children performed worse on tandem gait testing and had more errors on firm surface BESS at the initial post-injury evaluation. However, a significant difference was not observed on Romberg test between child age group and adolescent age groups. This may be that the Romberg test has greater focus on upper body movements compared with BESS. The Romberg test is a qualitative test compared with the BESS test which relies on a standardized scoring system. Moreover, the scoring of the BESS test is more clearly outlined when compared with the Romberg test. As such, the findings indicate that age is associated with postural control performance across the youth age spectrum following concussion. Clinicians assessing and managing concussion should recognize age differences in postural control performance when assessing children with concussion. This study addresses a growing need for studies investigating the signs and symptoms of childhood concussion as compared to adolescents.
The tandem gait test has become an increasingly popular method to assess postural control after concussion in conjunction with other established assessment methods [10, 19–22]. As a relatively complex motor task, the tandem gait test may be more difficult for children due to their ongoing motor system maturation [23]. It is known that brain development occurs into young adulthood [24]. Specifically, the amount of white matter in the brain increases throughout childhood and adolescence whereas grey matter shows regionally distinct increases predicated on location within the brain and age [25]. Prior studies have found that a majority of uninjured adolescents (∼75%) perform the tandem gait test slower than the 14 second cutoff recommended by the SCAT3 [21], suggesting that they likely have more difficulty performing the test than the uninjured young adults from which this threshold was established [26]. Furthermore, the definition of an abnormal tandem gait test in this study was based upon a binary outcome, limiting the ability to compare to other studies that have used an objective time to completion as an outcome measure. However, an abnormal test likely indicates gross motor dysfunction that is easily observable by a trained clinician, or an inability to comprehend the instructions provided. As such, the tandem gait test as a postural dysfunction screening tool may possess clinical value and is viable to conduct in most settings, thus providing information that augments other established test protocols, such as the BESS.
Previously, Brooks and colleagues observed that among uninjured youth athletes, younger aged individuals (5–7 years) showed more firm surface BESS errors compared to older aged individuals (8–10 years and 11–13 years) [14]. These findings illustrate significant differences in firm surface BESS between children and adolescents with concussion, where children made significantly more errors than their adolescent counterparts during this testing condition. In light of the Brooks findings, it is possible that these findings are partially due to inherent age differences in postural control, and independent of a concussion. However, no differences in foam surface BESS were identified. One potential explanation for the lack of a significant between-age-group finding in this condition may be the sensory novelty of the foam surface. Other studies have shown that the modified (firm surface only) BESS is more reliable than the full version (with foam) BESS [27]. The firm surface condition may also provide adequate complexity and/or difficulty to distinguish between age groups, while the foam surface likely possessed some ceiling effects (i.e. patients scored closer to 10). Prior work by Zemek and colleagues and Howell and colleagues has suggested that the firm/tandem stance of the BESS can provide prognostic information [28, 29].
Prior research has shown that children 10–13 years of age without history of concussion perform the BESS firm conditions with an average of 5.69 errors [17]. This study, which included only patients with a concussion, indicated that the child age group completed the firm BESS conditions with a median of 8 errors. It is feasible to expect that children who sustain a concussion will make a greater number of errors after concussion than when uninjured. Similar to these findings, Khanna et al. corroborated no difference in foam BESS scores between uninjured child and adolescent groups [17].
The findings of this study have implications for the assessement and management of children who are diagnosed with a concussion. Clinicians should interpret balance performance of patients with concussion in the context of age. Specifically, they may consider specific management strategies and counseling to parents of concussed children relative to injury management related to activity recomendations, or specialist referral. Further research is necessary to fully corroborate such management strategies. As such, it may be worthwhile to examine patient performance in light of age in order to develop appropriate individualized management plans for concussion recovery.
Limitations
This study has limitations and its findings should be interpreted with these in mind. Although the sample of 462 patients is a strength of the study, it was performed at a large quaternary care hospital with pediatric concussion specialists. Thus, patients included in the study may have had more severe injuries when compared to the general population of youth who sustain a concussion. As such, further work will be required to better understand the generalizability of these findings. This study did not have a control group and this analysis was based upon chronological age rather than biological maturation. It is possible that postural control measures correlate more strongly with biological maturation vs chronological age. Furthermore, groupings were chosen to be aligned with the age groupings of the child SCAT-5, ages 5–12 years old, and SCAT-5, ages 13 years old and older. Additionally, athletes were not analyzed based upon specific sport. Given the inherent differences in postural control demands between sports, such comparisons may provide further elucidation of the effects of concussion on postural control. It was also observed that the adolescent age group had a higher proportion of females than the child age group. This may reflect the demographics or referral patterns present within this single-institution specialty care sports medicine practice, but also likely played a role in the observed effects.
Conclusion
In conclusion, postural control deficits were more common among the child age group compared with the adolescent age group when assessed within two weeks following a diagnosed concussion. Specifically, the child age group was independently associated with abnormal tandem gait test performance and more errors on the firm surface condition of the BESS. Accordingly, postural control performance may provide key insights into concussion assessment differences between children and adolescents and may help to identify individualized treatment pathways.
Footnotes
Acknowledgments
The authors wish to thank Gerald Clayton, PhD, Jacqueline Murray, RN, PhD, and Pamela Wilson, MD who helped develop and implement the concussion clinical registry.
Conflict of interest
The authors declare no conflicts of interest related to this study. Unrelated to this study, Dr. Howell has received research support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development, the National Institute of Neurological Disorders And Stroke, and MINDSOURCE Colorado Brain Injury Network.