
Abstract
PURPOSE:
This study aimed to describe brace use, progression of scoliosis, and surgery in children with cerebral palsy (CP) and spina bifida (SB) who were initially treated with a brace.
METHODS:
Medical records were retrospectively analysed for brace compliance, treatment complications, curve size measurements with and without the brace at both start and at follow-up, and number of patients undergoing spine surgery.
RESULTS:
Sixty-eight children were included (CP 47, SB 21), 37 of whom were girls, with a mean age at start of treatment of 11.1 (CP) and 8.2 (SB) years. Most had severe motor problems; only four children with CP and five with SB were able to walk. Thirty-five in the group with CP and 11 in the group with SB had a curve size over 40°.
Forty used the brace full-time, 19 half-time and nine for a varying proportion of time. Transient complications of brace treatment were seen in 28%. The yearly progression of curve-size was 4.2° in CP and 2.3° in SB.
Twenty-eight patients underwent surgery and complications were present in 75% of these patients. Twenty-seven out of 46 patients with severe scoliosis did not undergo surgery.
CONCLUSION:
Brace treatment was possible, even in patients with severe scoliosis. Bracing can delay the progression of scoliosis.
Introduction
In children with cerebral palsy (CP) and spina bifida (SB), scoliosis is common and correlates with gross motor function [1–4], with a higher incidence in children who are unable to walk [1, 5–8]. A higher frequency of scoliosis has been reported in patients with CP whose general state of health is poor [2, 7]. Scoliosis is often associated with an asymmetric sitting position and an increased risk of pressure ulcers [9, 10].
The progression of scoliosis in patients with CP has been reported as a yearly curve increase ranging from 0.8 to 23.5° [2, 11]. The progression is dependent on age, functional level, and severity of the scoliosis. There is a higher risk of progression if the curve size is above 40° and increasing risk with more spinal rotation [11]. Deterioration can continue even after skeletal growth has ended.
Scoliosis in patients with SB differs from that in patients with CP with regard to underlying causes; scoliosis in SB can be of congenital origin or a symptom of a tethered spinal cord. The yearly curve increase has been reported to range from 1.2° to 14° with a mean yearly progression of 4.5°. The smallest increase in angles is seen in children with a curve less than 20°, and largest increase in children with a curve above 40° [12, 13]. The fastest progression was seen between the ages of 11 and 15 years, and after 16 years of age there was hardly any progression [12].
Scoliosis can affect many functions in daily life, such as sitting ability, respiration, and gross motor skills, and it can also cause pain. Patients with severe scoliosis may be unable to assume a sitting position and hence unable to participate in many everyday activities [14, 15]. Treatment options for scoliosis in CP and SB include bracing and surgery [6, 16–18]. As in idiopathic scoliosis, surgery is usually recommended if the curve size is above 40–45°. However, surgery is associated with a higher risk of complications in neuromuscular scoliosis than in idiopathic scoliosis [19–21]. There is an ongoing discussion about the effect of brace treatment in children with neuromuscular scoliosis, but studies of such children are scarce. Brace treatment can be problematic in patients with CP and SB due to problems with gross motor function, asymmetric postures and contractures, sensory loss, and problems with feeding and sleeping. Further, fitting the brace to a patient is a challenge; comfort problems and ulcers have been reported [11, 17], and gastrointestinal trouble and respiratory problems have been reported to cause termination of brace treatment (9). The primary purpose of brace treatment is to slow down the progression of the scoliosis, but a secondary purpose may be to facilitate sitting [9, 17]. In addition, brace treatment may prevent the spine from collapsing in cases of rapidly increasing scoliosis [10, 14]. In some patients, surgery is not possible for medical reasons, making a brace the only possible intervention.
Studies have shown that a brace can have a positive effect on curve progression in patients with SB and CP if the curve size is less than 40° at the start of treatment [9, 17]. A large immediate correction obtained with the brace was a predictor of a better end result, as has also been described for idiopathic scoliosis [22]. In two studies, it was found that flexible curves above 50° could also be handled with conservative treatment [9, 14]. Finally, it has been reported that sitting function can be improved by a brace [14, 23].
The aim of the present study was to describe brace use, scoliosis progression, and subsequent need for spine surgery in children with CP and SB who were initially treated with a moulded Boston-type scoliosis. This study also aimed to describe complications and adverse events in connection with both bracing and surgical interventions.
Materials and methods
A retrospective review was made of the medical records of all children with CP and SB who were followed at a regional orthopaedic clinic and fitted with a Boston-type scoliosis brace at the regional rehabilitation centre from 2003–2013. Data were searched for a minimum of five years after the start of treatment. Data were retrieved with regard to the following:
brace compliance, in hours of daily use reported by parents curve size of the scoliosis, measured using the Cobb method on posterior anterior x-rays with and without the brace at the start of treatment and at follow-up number of patients for whom surgery was recommended number of patients who underwent spine surgery complications/adverse events in brace treatment and in surgery.
All x-rays were taken sitting; support was given for those who needed it via a specially made chair with a high backrest and a belt. If needed, a parent could also provide support to allow the child to maintain a balanced position. Scoliosis severity was classified according to whether the primary curve at the start of treatment was above or below 40°. Indication for surgery was based on size and progression of the scoliosis.
Gross motor function was classified using different systems depending on diagnosis. For children with CP, the Gross Motor Function Classification System (GMFCS) was used [24], in which levels I–III represent independent walkers, with or without aids. The children with SB were classified in accordance with Hoffer [25], in which scores 1–2 represent walkers. Sitting ability was classified according to whether a patient was able to sit without support or not.
Only those children who had used a brace for at least two years were included in the evaluation of the size of the scoliotic curve.
The study was approved by the Central Ethical Review Board of Gothenburg, Sweden, on 24 November 2017 (Ref. No. 915-17).
Statistical methods
Parametric t-tests were used for the analysis of age and curve size, the independent t-test was used for comparison between groups, and the paired t-test was used to compare outcomes before and after the intervention. The chi-squared test was used for the analysis of differences in nominal data. The level of significance was set to p < 0.050. For the analysis of the correlation between the curve size at follow-up and the initial correction, the Pearson product-moment correlation was used.
The statistical analyses were performed using the SPSS software package, version 25 (SPSS Statistics, IBM Corporation, NY, USA).
Results
A total of 75 patients meeting the inclusion criteria were found. Of these, five were excluded because they only had kyphosis, one was lost to follow-up after moving away from the area, and in one patient an attempt to use the brace was terminated owing to poor general health. This left 68 children who were included in the study. All braces used were made from a mould and were of the Boston type [26]. It was recommended that the brace should be worn for 23 hours a day if possible.
Information about the participants is presented in Table 1. Among the 47 children with CP, there were 25 girls and 22 boys with the following sub-diagnoses: bilateral spastic CP (n = 20), dyskinetic CP (22), ataxic CP (two), and unknown (three). Most of them had severe motor problems; according to the GMFCS, 35 were at level V, eight at level IV, three at level III, and one at level I. However, nine could sit without support, of whom four could walk, with or without aids. Among the 21 children with SB, there were 12 girls and nine boys. All children with SB had the myelomeningocele type of SB; 16 of them could sit without support, and five could walk, with or without aids.
Data on participants, including curve size and brace use. Data presented as mean (SD) and as min–max or number of patients (%)
Data on participants, including curve size and brace use. Data presented as mean (SD) and as min–max or number of patients (%)
CP: cerebral palsy; max: maximum; min: minimum; SB: spina bifida; SD: standard deviation.
There was a statistically significant difference between the children with CP and those with SB at the start of brace treatment: the children with CP were older (p = 0.003) and had a greater curve size (p = 0.026), while a higher percentage of the children with SB could sit without support (p < 0.001).
Of the children with CP, 24 used the brace both day and night, 18 used it on a “half-time” basis (8–14 hours a day), and five used it for varying proportions of time, ranging from periods with full-time use to periods without the brace; see Table 1. Of the children with SB, 16 were full-time users, one used the brace half-time, and three varied in their time of use; data are missing for one patient. After the scoliosis treatment period, 14 patients with CP and three with SB continued to use the brace as a sitting support.
One or more complications from brace use were noted in 13 children with CP. Early issues consisted of skin problems, vomiting, respiration problems, and difficulties sleeping at night. These complications were transient and could be resolved by adjustment of the brace, by more time getting used to the brace, or by a decision not to use the brace in some situations, such as during meals and while sleeping. Late problems arose in connection with a change of brace or with other surgical or medical interventions. Two patients had hip flexion contractures, which, as the brace stabilised the lumbar spine, prevented them from standing and walking with an erect posture; this indicated that they would need hip surgery before scoliosis surgery could be considered. In the children with SB, six had transient problems, including early difficulties with daily activities, problems with itching, and difficulties tolerating pressure over the bladder. Late problems in the children with SB included pressure marks/wounds when changing to a new brace or in connection with other surgery. All of these problems could be resolved by adjusting the brace.
A total of 33 children with CP and 18 with SB were X-rayed in a sitting position both with and without their brace at the start of treatment; see Table 2 and Fig. 1. The scoliosis was considered severe in 25 children with CP (76%) and nine with SB (50%). There was a statistically significant correction of the curve with the brace, regardless of the severity of the scoliosis; there was no difference between CP and SB (p = 0.319). The amount of correction varied greatly, with a range of 0–45° in the group with CP and 3–40° in the group with SB. At follow-up, which was on average 4–5 years after the start of treatment, 45 patients were x-rayed without their brace. The mean curve size had increased in both groups, but there was considerable variation; some patients actually had a smaller curve at the follow-up than they did at the start of treatment. The mean yearly increase was 4.2° in CP (standard deviation [SD] 3.9) and 2.3° in SB (SD 5.3). There was a weak correlation between the increase of the scoliotic curve at follow-up and the initial correction (r = 0.321, p = 0.049), with better results for those who had a better in-brace correction at the start of treatment, but there was no difference depending on whether the initial curve was severe or not. Comparison of 27 children who used their brace full-time with 17 part-time users (half-time or varied) showed a tendency for results to be better with full-time use, but this tendency did not reach statistical significance (p = 0.059). The mean total progression of the scoliosis from the start of treatment to follow-up was 10.7° in full-time users and 19.9° in part-time users.
Data on the scoliotic curve in children with brace use > 2 years in 51 children at the start of treatment and in 45 children at follow-up. Data broken down by diagnosis. Mean (SD) and min–max. Negative figures indicate increased scoliosis
CP: cerebral palsy; max: maximum; min: minimum; SB: spina bifida; SD: standard deviation.
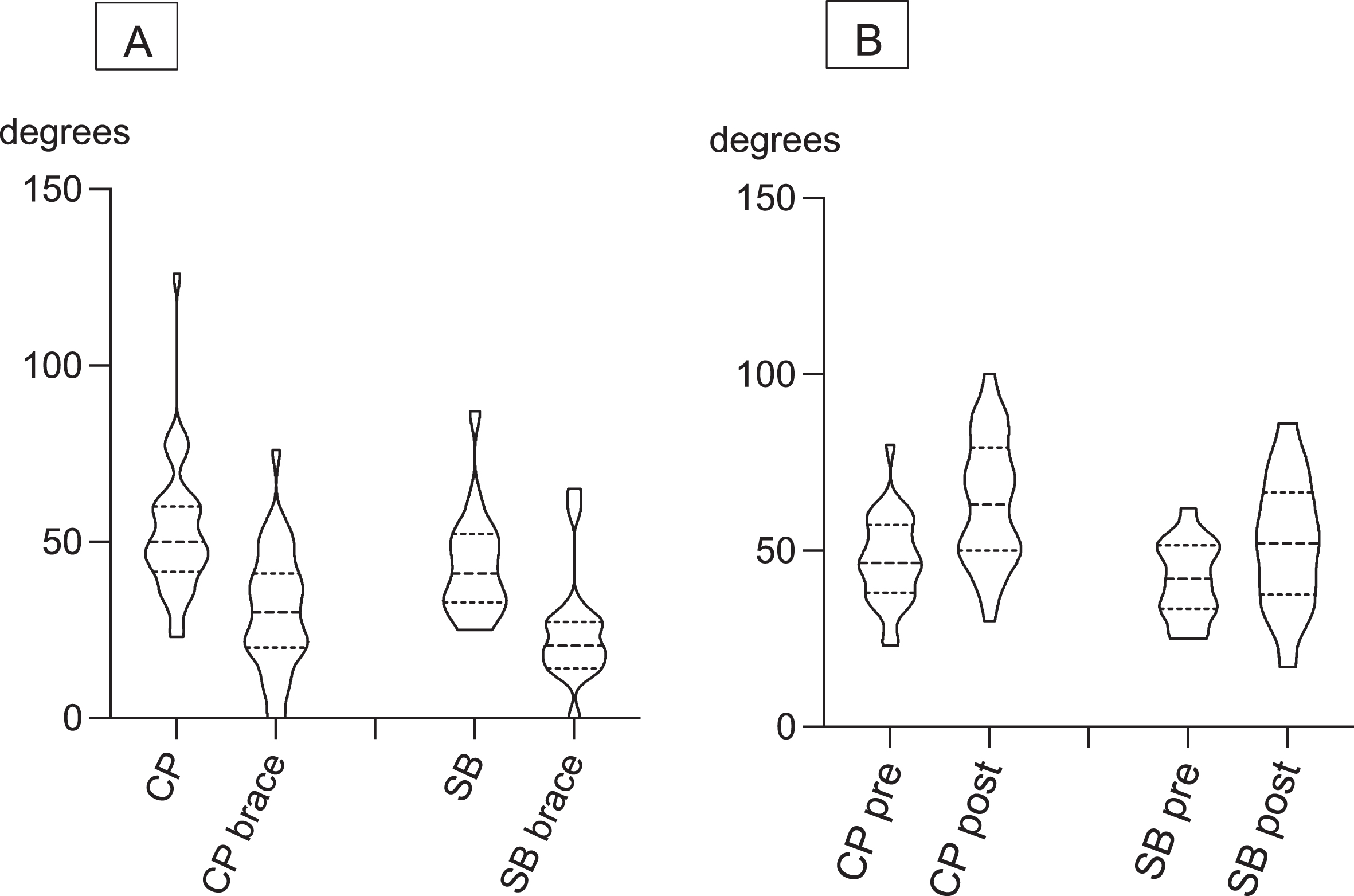
Curve size, split by diagnosis: A –without and with brace at start of treatment, B –without brace before treatment and when brace treatment for the scoliosis was completed. Data are presented as violin plots, indicating distribution of data and with median, first and third quartile as dotted lines. CP: cerebral palsy; SB: spina bifida.
Surgery was discussed for all patients with severe scoliosis at the start of treatment and when there was a progression, but subsequent surgical correction of the scoliosis was only performed on 20 children with CP and eight with SB at a mean age of 15.1 years; see Table 3. This included 40% of the children with a small curve and 34.2% of those with a severe curve, with no statistically significant difference depending on whether the curve was small or severe at the start of treatment. Of the 35 patients with CP and 11 patients with SB who had severe scoliosis at the start of treatment, 20 with CP and seven with SB never had spine surgery. Three of the non-surgery group were not in good enough health to undergo surgery, one was still waiting for surgery, three were waiting for various other interventions prior to surgery, and three declined because of the risk of losing motor function. Furthermore, 13 children/families were satisfied with using a brace and were not interested in a surgical intervention. Surgical correction was also discussed in children with a small curve size (less than 40°), and four out of nine with CP and one of five with SB did not receive spine surgery. All but two of the children who underwent surgery used their brace until surgical correction.
Data on surgery. Age at surgery, number and complications, presented as mean (SD), number and percentages
CP: cerebral palsy; max: maximum; min: minimum; SB: spina bifida; SD: standard deviation.
Complications were reported in 15 of the 20 children with CP who underwent surgery; some patients experienced more than one problem. Five patients needed surgical revisions and three developed infections. Three children had a long and complicated recovery period; of these, one had recovered at follow-up but the other two still had serious medical problems. Five had increased problems with sitting (three due to extreme lordosis), one had increased problems with pelvic asymmetry compared to before surgery, and one had problems with neck position. Further, one patient had problems standing erect owing to flexion contractures in the hips. Regarding the children with SB who underwent surgery, six out of eight had complications in conjunction with their surgery. At follow-up, three had loss of sensory or motor function, two had longstanding problems with pain, and one had problems with pressure ulcers.
Treating children with scoliosis and severe gross motor deficits with a brace is a challenge, but the present study showed that brace treatment was possible and that most problems could be handled even in those with more severe curves. This is consistent with findings from a study on neuromuscular scoliosis to the effect that a flexible curve above 50° can be handled with conservative treatment [14]. Compliance in terms of brace use was good overall but was highly variable. All braces were made from a mould by experienced orthotists, and the children all spent a period as inpatients after receiving their first brace, which may have had a positive effect. During that period, the treatment time was gradually increased and the parents were trained to handle the brace. After this, there was regular follow-up at the orthopaedic clinic every six months. The importance of the involvement of experienced orthotists has also been described in another study in children with CP [9].
In the current study, there was a progression of scoliosis despite the brace treatment. In patients with SB, the yearly progression was less than the natural course [12, 13], and in patients with CP, the yearly progression was similar to that observed in another study of brace treatment [9]. No studies were found on the natural course in CP that were directly comparable to the sample in the present study. Comparing the rate of progression to idiopathic scoliosis, in which brace treatment is deemed to have failed if the yearly curve progression is more than six degrees [27–29], indicates a positive result of the brace treatment in this study. Further, it has been described that the fastest progression is seen in curves above 40° [2, 7]. In the current study, no differences in scoliosis progression were observed between severe and mild scoliosis, and contrary to previous studies [9, 17], there was only a very weak correlation between the initial correction with the brace and the effect on progression. However, the patient groups in those studies were not fully comparable to the present study.
Besides having a direct effect on the scoliosis, a brace can also have other areas of use. For example, bracing is known to be an effective way of stabilising the trunk and improving sitting function [9, 23]. Fourteen patients with CP and three with SB in the current study continued to use the brace as a sitting support after the treatment period. A brace can also be used while waiting for surgery: if the scoliosis progression slows down, the child will have more time to grow and hence the scoliosis may be less severe at the time of surgery. Also, if severe scoliosis is untreated, there may be a risk of a collapsing spine owing to gravity [14]. Further, problems with posture and positioning could be identified by bracing and considered before surgery, as exemplified by the patient not being able to stand erect after surgery due to flexion contractures in the hips that were compensated by the lordosis before surgery.
The Cobb method, which involves measurement of curve size using x-rays, is the most common way to evaluate the progression of scoliosis. Although this is an objective measure, comparison to other studies may be difficult because the x-rays are sometimes made in a sitting position (as in the present study) and sometimes in a supine position [9, 11]. The latter position may lead to an underestimation of the magnitude of the scoliosis, considering the frequent problems with postural control and muscle weakness in children with CP and SB. Gravity may also be more important for the development of neuromuscular scoliosis than idiopathic scoliosis. Therefore, performing x-rays in a sitting or standing position has been recommended in patients with CP [5, 10].
Studies of idiopathic scoliosis have shown that treatment with a Boston brace for 21–23 hours a day had a good effect on retarding scoliosis progression [29, 30]. The guidelines for treatment underpinning the present study follow the same recommendation; if a patient could not tolerate wear for 23 hours a day, they were encouraged to use the brace as much as possible. Concerning duration of brace use, the results differed between full-time and half-time users, but the difference did not reach statistical significance. This finding may indicate that it is possible to be less strict regarding night-time bracing, especially in children with CP who often have sleeping problems. On the other hand, it has been reported that some children are more relaxed with the brace than without it [23]. More studies concerning brace treatment in neuromuscular scoliosis are needed to increase knowledge and to provide guidance when choosing among treatment options for children with multiple comorbidities. This is also pointed out in recently-published orthopaedic guideline for people with SB, which recommended trying bracing as a first treatment option and avoiding surgery if possible [31].
There were some complications associated with the braces in areas such as skin concerns, eating, and sitting. Most problems were transient and could be resolved through adjustment of the brace, adjusting wear time, or by adjustments to sitting support in the child’s chair. The high rate of complications from surgery observed in this study is similar to the results from other studies of surgery in neuromuscular scoliosis [19–21]. Adverse effects of surgery may be irreversible, and this possibility needs to be taken into account when planning treatment. Surgery was discussed or proposed at the start of brace treatment for all patients with severe scoliosis in the present study, but only one-third of them eventually underwent a surgical correction. Further, compared to studies on the natural course of scoliosis [2, 11–13], bracing seemed to delay the progression of the scoliosis. As bracing was used from the start in the present study, it can be interpreted that bracing may have delayed progression to a point at which surgery was no longer considered necessary. Many patients functioned well with the brace in everyday life and declined surgery due to a poor general state of health or the risk of losing motor function.
There are a few limitations to the present study that may influence the generalisability of its results. First, it is a retrospective study with no control group. There are only a few previous studies on the natural course of scoliosis, and differences in assessment protocols make comparison with other studies difficult. Second, for analysis of subgroups, the sample size may be too small to detect differences. Third, data were collected from medical records, and treatment time in hours as reported by parents is not an exact measure. In addition, there were a few long treatment gaps for some patients, and this may have influenced the results. Those gaps included periods associated with other types of surgery or medical problems that made brace use difficult. However, all children in the region (covering about 1.7 million inhabitants) with CP or SB and scoliosis who tried brace treatment were included in the study. The various clinics involved in the treatment of scoliosis have a well-established working relationship, and the health care professionals involved have many years’ of experience with children with CP and SB.
Conclusion
This study showed that brace treatment was feasible in children with CP and SB and appeared to be effective with relatively few complications. Compliance was mostly good but varied over time for some participants. Bracing can delay the progression of scoliosis in many patients, even in those with a severe curve. In the present sample, 32 of the 60 patients, for whom a spinal correction was initially planned, did not get spine surgery.
Footnotes
Acknowledgments
The study was funded by the Petter Silfverskiöld memory foundation.
Conflict of interest
The authors have no conflicts of interest to report.