
Abstract
PURPOSE:
The primary aim was to describe sports participation of Dutch children and adolescents with lower limb deficiencies (LLD). The secondary aim was to explore perceived limitations concerning sports participation.
METHODS:
A total of 103 children and adolescents with LLD, aged 8–18 years (mean 11.7 years), were asked about their sports participation using a study-specific self-report questionnaire.
RESULTS:
Children and adolescents with LLD frequently (78%) participated in sports activities, and most of them (68%) participated in the sport of their preference. Just over half of all children (52%) perceived an inability to participate in specific sports. Physical performance (running) and endurance were mentioned as the most limiting factors in participating in certain sports.
CONCLUSION:
Children and adolescents with LLD in the Netherlands participate in a variety of sports. Despite dependency on lower limb prostheses in most cases, children and adolescents with LLD have a high potentiality of participating in sports.
Introduction
Children with lower limb deficiencies (LLD) deal with partial or total absence of the lower limb(s) due to a congenital deficiency, trauma, or secondary to disease [1]. Many of them have a congenital deficiency resulting in a longitudinal or transverse disorder, such as fibular deficiency, tibial deficiency, proximal focal femoral deficiency and ray defects of the foot. These deformities most often appear unilaterally and present great variability in severity [2]. Impaired physical function and decreased participation in physical activities can occur due to the altered structure of the deficient lower limb(s) [3]. In some cases of congenital deficiencies, surgical intervention including reconstruction or (conversion) amputation is required to achieve high functional performance, optimal participation and higher quality of life [4].
Most children with LLD are dependent on prosthetic devices for mobility to enhance their functional abilities [5]. In mild cases of LLD, children wear orthoses or a shoe raise to support unstable ankle joints or equalize small leg length differences. Functional outcomes of children with unilateral LLD are promising, whereas children with bilateral limb loss face more challenges [6]. In general, the more severe the LLD and higher the amputation level, the greater the challenges in walking and running. In the Netherlands, approximately 500–600 children (<18 years) use a lower limb prosthesis [7].
Participation in sports or physical activity is favourable for all children, including those with disabilities [8]. It promotes higher levels of psychological and physical well-being and a more positive body image compared to children who do not play sports [9]. Sports participation is strongly associated with increased levels of physical activity and better health-related fitness in youth, including in those with chronic diseases or physical disabilities [10]. Weekly participation in sports is suggested as a solution to maintain and optimize physical activity levels. Particularly for a child with LLD, involvement in sport activities is an important mechanism for developing motor coordination, integration with peers and adjustment to physical limitations [11, 12].
Despite a high level of physical activity and participation in a variety of sports, evidence suggest that the sports participation of children with physical disabilities, including limb deficiencies, is lower compared to typically developing children [13, 14]. Although most children with LLD can be fitted with appropriate prostheses to optimize their functional abilities, they still encounter certain challenges when participating in sports [4]. Overall, children with LLD seem to experience limitations and challenges in more complex movements like running and keeping up with their peers in regular sports, due to their prostheses [15]. Furthermore, children with LLD are faced with stigma and reactions from the social environment due to the appearance of the deficient leg(s) [16].
Although the participation in leisure activities of Dutch children and adolescents with LLD is comparable to peers [17], no data are available on their actual participation in sports. The primary aim of this study was to describe sports participation (type, frequency, and preference) of children and adolescents with LLD in the Netherlands. Differences between various degrees of limb loss and different prostheses were explored. The secondary aim was to investigate the opinions of children and adolescents with LLD regarding perceived limitations concerning sports participation.
Methods
For this cross-sectional, exploratory, and descriptive study, data was obtained in 2014 via a study-specific questionnaire on participation in sports for children with LLD. In 2018 and 2019, additional data was collected in order to broaden the sample. The questionnaire was handed out to children and adolescents with LLD, aged 8–18 years. All participants completed the questionnaire once. The research protocol was reviewed and complied with the ethical guidelines of De Hoogstraat Rehabilitation in Utrecht, the Netherlands. The questionnaire used to collect data required minimal time to complete and was considered to not bring emotional burden to the participants. Participation in this study was voluntary, and anonymity after submitting the questionnaire was guaranteed.
Participants
A convenience sample of children and adolescents with LLD was recruited from a patient database at the Hoogstraat Rehabilitation Center in Utrecht, the Netherlands. The inclusion criteria were LLD with or without upper limb deficiency and age between 8 and 18 years. Excluded from the study were children with cognitive impairment or syndromal disorders.
In 2014, most of the children were contacted during their regular visit to the rehabilitation centre where they could fill in the questionnaire on paper. In addition, children were contacted via an email to their parents with information about the study and a request to complete the questionnaire. If no email address was available, the questionnaire and information about the study were sent by post. In 2018 and 2019, children were recruited via email with a link to a digitalized version of the self-report questionnaire using the platform ‘Survio’ [18]. Parents were asked to have their child complete the questionnaire on their own, if possible. One reminder email was sent if no response was received within six weeks.
The participants who completed the questionnaire were grouped by age, either as children (under twelve years of age) or adolescents (twelve years or older). Medical diagnosis including degree of limb loss and type of prosthesis was obtained from the medical records of the Hoogstraat Rehabilitation Center. For this study, the degree of limb loss was recorded as unilateral LLD, bilateral LLD, and LLD in combination with upper limb deficiency. The various prostheses the children used were described as follows: Below Knee (BK), Above Knee (AK), lengthening prostheses (see Fig. 1), rotationplasty, hip disarticulation (see Fig. 2) and stubby prostheses (see Fig. 3). Children with orthotic devices like foot orthoses or shoe raises were combined in the non-prosthetic group.

Lengthening prosthesis.

Hip disarticulation prosthesis.

Stubbies.
Participation in sports was measured using a self-constructed questionnaire (see translated version in the Appendix). The questionnaire is a self-report survey regarding participation, type, frequency, preference and perceived limitations in sports; participants and their parents could also indicate a need for information about specific sports. It takes 5–10 minutes to complete. The questionnaire contains five closed questions (yes or no) followed by open-ended questions about types of sports, frequency, preference of sports and experienced limitations. Comparative data on the frequency of sports participation of typically developing children in the Netherlands was obtained from national records [19].
Statistical analyses
Descriptive statistics (frequency, percentages) were used to describe the sample and children’s participation in sports. The actual sports participation levels of children (8–11 years old) and adolescents (12–18 years old) with LLDs were compared using a Pearson Chi-square test. Comparisons in sports participation in all children and youth with different degrees of limb loss (unilateral, bilateral and combinations of limb deficiencies) and use of different prosthesis were assessed using Chi-Square analyses. Values of p < 0.05 were considered statistically significant. All data were analysed with SPSS version 26.
The open-ended questions regarding preference and perceived limitations in sports were analysed using content analysis [20]. The responses to the open-ended questions were coded and categorised by the first author. The co-authors (paediatric physical therapist, senior researcher, and paediatric rehabilitation physician) reviewed the categories to reach consensus. Subsequently these categories were subdivided into the following International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) domains [21]: physical performance (PP), physical endurance (PE), body function (BF) and social participation (SP).
Results
One hundred and forty-two (142) children and adolescents were invited to fill in the questionnaire: 94 in 2014 and 48 in 2018/2019. One hundred and three children (73%) returned the questionnaire (62 in 2014 and 41 in 2018/2019). Of the participants, 58% were boys, and the mean age of all participants was 11.7 years. Most of the children (69%) had a unilateral LLD and 91% used prosthetic devices during activities of daily living. One participant was dependent on a wheelchair for mobility. LLD in combination with upper limb deficiency was present in 18 children (17%), varying from absent forearm (transversal defect) to missing rays of the hand (longitudinal defect) and dysplastic or deviated fingers. None of the children used an arm prosthesis or adaptive devices in sports. The demographic characteristics of the participants with LLD are summarized in Table 1.
Demographic characteristics of participants with LLD (n = 103)
Demographic characteristics of participants with LLD (n = 103)
LLD: Lower Limb Deficiencies, *Bilateral prosthetic use.
Eighty (78%) children and adolescents with LLD (8–18 years old) participated in a variety of sports. No statistical differences were found between children (8–11 years old) and adolescents (12–18 years old) or between the different degrees of limb loss. Children and adolescents with LLD using different prosthetic devices showed no differences in their levels of sports participation, except children who used an AK prosthesis or rotationplasty prosthesis had a lower percentage of participation in sports activities. See Fig. 4 for participation in sports levels for children with LLD using different prostheses.
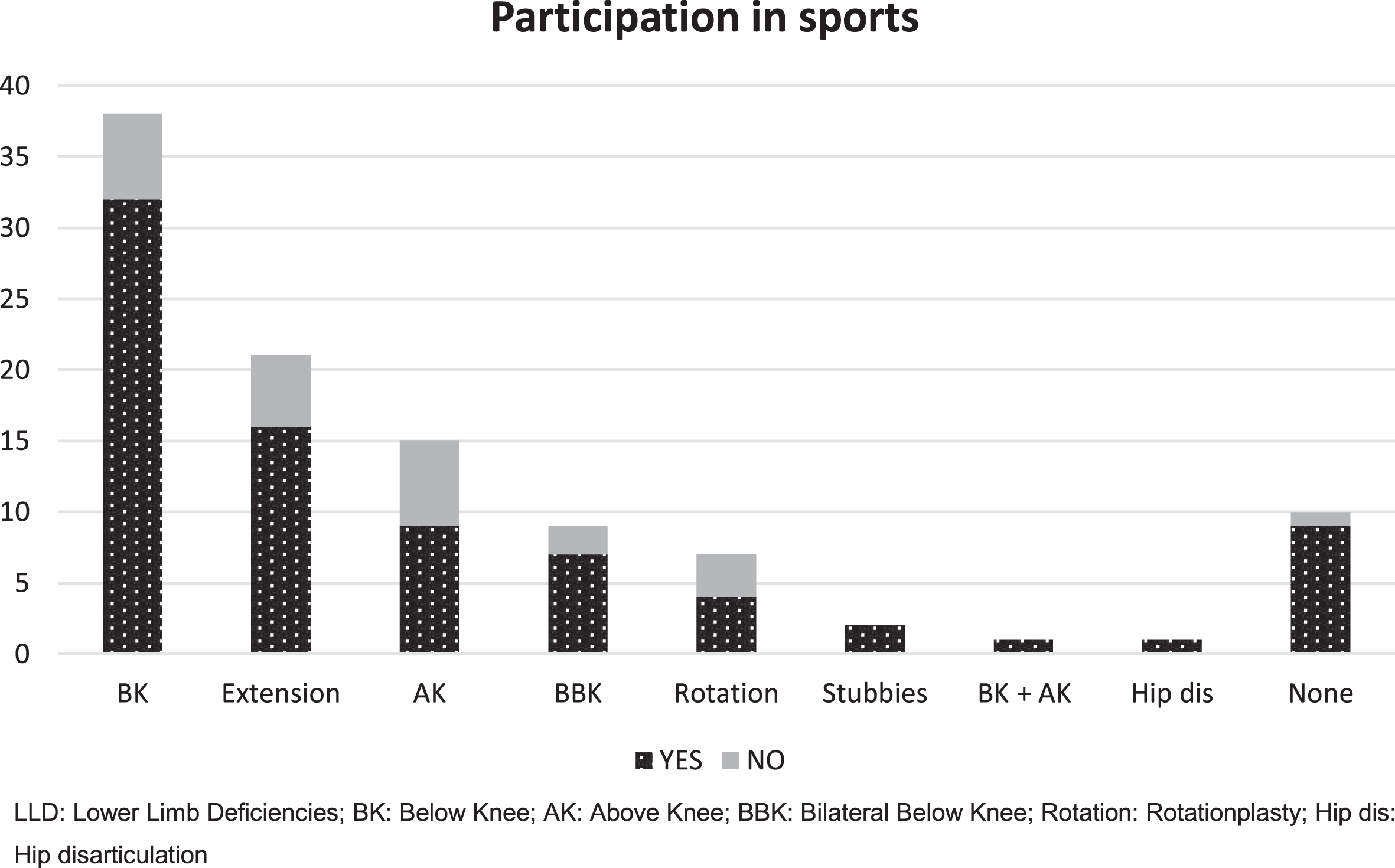
Participation in sports of children with LLD using different prosthesis (n = 103).
The reported frequency of sports participation was once or twice a week for most of the children (51%). The most practiced sports were soccer (18%), swimming (10%), hockey (6%) and dancing (6%). Seven (7%) children participated in adapted sports (wheelchair tennis, sitting volleyball, wheelchair basketball, wheelchair hockey, and soccer for children with disabilities). Twenty-three (22%) children did not participate in sports at the time of the study. Four of them did participate in sports in the past but indicated that they had since quit sports. An overview of the types of sports of the participants with LLD is summarized in Fig. 5.
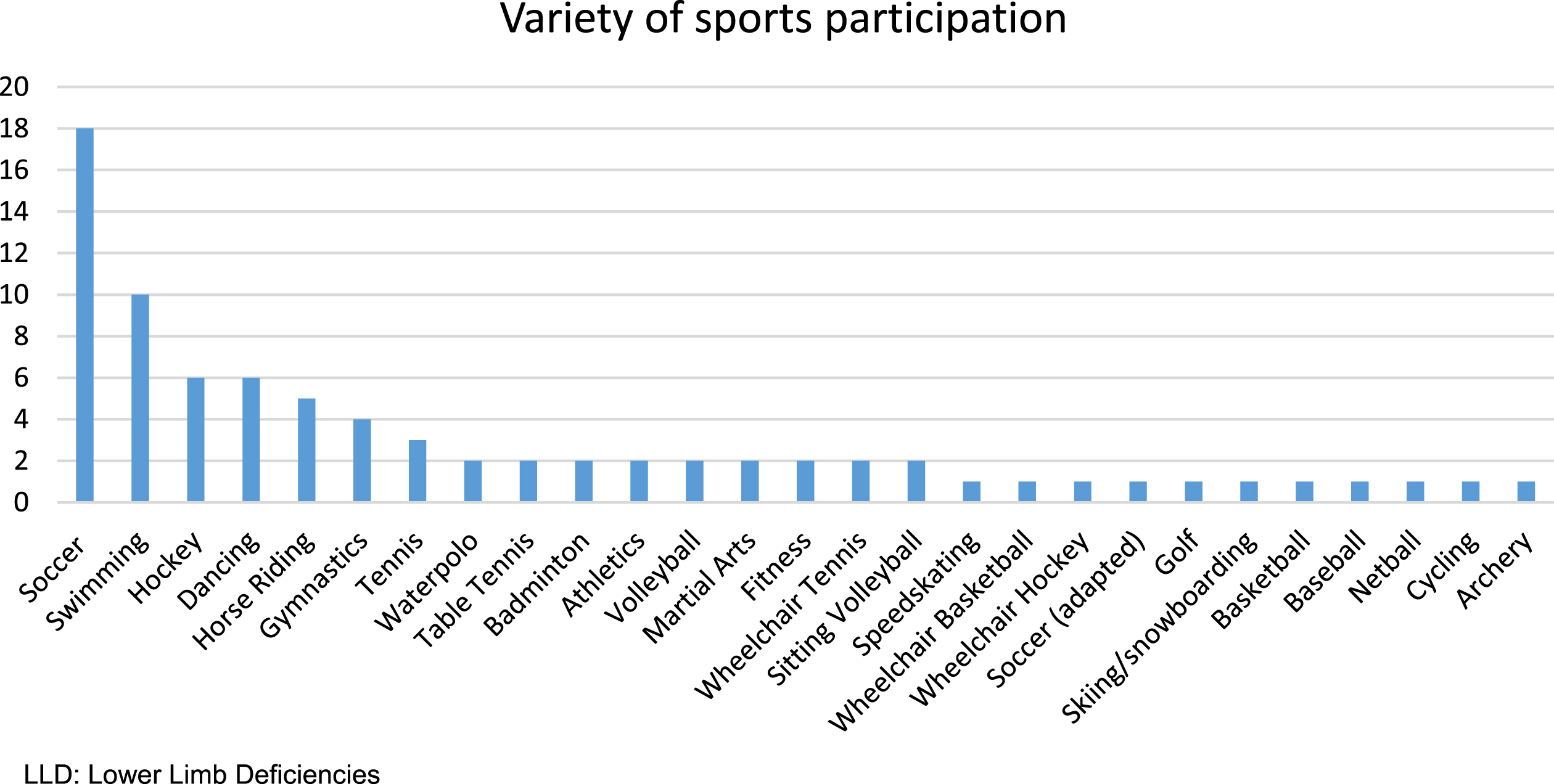
Variation of sports participation of children with LLD (n = 103).
Approximately one-third of the children (32%) and the parents (35%) indicated a need for information on specific sports that children should be able to do.
The results of the participants are shown in Table 2.
Results of participants with LLD
LLD: Lower Limb Deficiencies; yrs:years.
Most children and adolescents (68%) participated in a sport of their preference. Forty-six children (45%), of which thirty-four were already participating in sports and twelve were non-sporting children, indicated an interest in certain sports that they would like to do but did not do. The sports of most reported interest were soccer (16%), martial arts (5%), dancing, volleyball, and tennis (all 3%).
Perceived limitations
Half (52%) of the children and adolescents with LLD in this study believed they could not perform every sport they liked. The most frequently rated sports that children thought they were not able to participate in were soccer (14%), running/athletics (9%), (speed)skating (6%), and gymnastics (5%).
The answers to the open-ended questions were analysed and described in four domains. The questions were ‘Are there sports you would like to do (but do not do); why not?’ and ‘Do you think there is a sport that you cannot do; why not?’
PP Domain
Most responses on both questions fit within the PP category. Two children mentioned their disability as a reason for not participating in the sport of their interest. Also, 10 children mentioned their disability and eight children their prosthesis as an obvious reason for not being able to do certain sports. Inferior performance in running was reported by eight children. Three children experienced an inability to jump, and two children were limited in sports participation due to issues not related to the LLD but to a short arm.
PE Domain
Sixteen children were interested in sports other than the one they were participating in: eight children stated that the sport of interest required too much running and another eight children perceived their sport of interest as too physically demanding. In the PE theme, 10 children reported too much running and exhaustion as reasons for not being able to do certain sports.
BF Domain
Seven children reported non-specific pain, knee, or foot problems. Six of these used a BK prosthesis, five of which were participating in sports. One sporting child reporting pain problems was dependent on a lengthening prosthesis. The non-sporting child had a BK-prosthesis and reported knee problems.
SP Domain
Some children (16%) and adolescents (11%) reported having no time for the sports of their interest due to participation in other sports. For five children, there was no club available in their community. One child was too young, and two adolescents were not permitted to join the sport of their preference (soccer) due to their prosthesis (increased risk of hurting other children).
Discussion
The results of this study indicate that the majority (78%) of children and adolescents with LLD (aged 8–18 years) participate in sport activities. This equates to the Dutch norm (78%) of sport participation in children who are typically developing (age range 5–18 years) [19]. Age groups (8–12 years; 12–18 years) and degree of limb loss did not affect the levels of sports participation. However, the sports participation of children and adolescents with AK and rotationplasty prostheses was found to be less than in other types of prostheses. Despite proper engagement in sport activities, half of the included population perceived an inability to participate in specific sports. PP and PE were mentioned as the most limiting factors to participation in certain sports. A notable finding is that a substantial percentage of the children with LLD (34%) were involved in high-level sport activities that require running. On the other hand, some children with LLD claimed not to be involved in sports in which running is a major component. The ability to run is of huge importance for participation in a wide range of sports in which running is a basic component. Running is also considered to be an essential factor in active play and in peer interaction [11]. Furthermore, running can be a method to improve or maintain fitness levels and improve physical and psychological well-being. To the authors’ knowledge, there are limited published reports on the running performance of children with LLD. It would be interesting to know if specific training could enhance running performance in children and adolescents with LLD and if this could lead to increased sports participation for those who experience performance and endurance limitations. This should be investigated in future research.
Compared to Dutch children and adolescents with a chronic disease or disability who have a 26% participation rate in sports, the sports participation of children with LLD is much better, which suggests that they are less restricted [22]. Furthermore, in comparison to Dutch adults with lower limb amputations, the difference in sports participation is even more striking. Their engagement in sport activities is lower (15%), most often due to comorbid factors [23, 24]. The results of the current study suggest that 73% of children with LLD are active and have full potential to be able to participate in different sports with the expectation of maintaining active and sportive lifestyles in adulthood. It is important to watch the continuation of sports participation closely because, if children cannot participate in the sports of their preference, there is a chance that they will eventually stop participating in sports.
In this study, children using AK and rotationplasty prostheses engaged less frequently in sports activities. Whilst children with BK prostheses walk as fast as their healthy peers, children with an amputation level above the knee walk more slowly and at a greater energy cost [25]. As in adults, it is suggested that there is a graded decline in physical function and sports with level of amputation, which may become evident in higher level physical activities such as sports [25, 26]. This may explain the lower rates of participation in sports in children with an AK prosthesis. In rotationplasty, the lower limb is rotated to use the ankle and foot as a functional knee joint within a prosthesis [27]. Rotationplasty is an intervention applied to children with osteosarcoma and to children with congenital proximal focal femoral deficiency. In this study, five out of the seven children using rotationplasty prostheses did so due to proximal focal femoral deficiency. While children and adults with rotationplasty due to osteosarcoma report proper levels of function and active engagement in sports [28–30], children with rotationplasty in proximal focal femoral deficiency present significant differences in gait and posture and decreased walking speed due to reduced hip range of motion and strength [31]. This may explain the lesser participation in sports among the participants in this study.
Only a few children reported pain, knee, or foot problems, and most of those who did were participating in sports despite the discomfort. Encouraging results have been shown in studies in which adults with congenital fibular deficiency experience similar lower limb function compared to their peers [32, 33]. In general, children and youth with LLD present a wide variety of physical function. This is shown in the results of a study involving young Norwegian adults with congenital LLD who performed reduced levels of physical function, although a wide range between the participants was noted [34]. The large diversity in function among children with congenital LLD has also been noted in the study by Pate, in which some children and youth with longitudinal fibular deficiency functioned at levels comparable to unaffected peers and others did not [35]. A better understanding of the differences of functional levels in children and adolescents with LLD is necessary. Motivation and experiencing enjoyment in combination with the skills needed to participate in sports of preference are most likely key factors.
The top five sports practiced in the population in this study corresponds to the top five sports practiced by typically developing children (5–18 years old) in the Netherlands [19]. All of the children in this study participated in sports with their daily prostheses, and none used a sport-specific prosthesis. Children with LLD can perform sports with their regular prostheses, but with increasing age (and height) this may become more difficult depending on the kind of sport. With more advanced prostheses or a sport-specific prosthesis, persons with limb deficiency can compete at high levels in different sports [11]. Unfortunately, these prostheses involve considerable costs, which can be considered a potential barrier to sports participation [24, 36]. Hopefully, in the future it will be easier for sport-motivated children and adults to acquire a more advanced prosthesis adjusted to their sports preferences.
Finally, in this study, one-third of the children and parents reported interest in receiving information about sports. This underscores the vital role rehabilitation professionals play in emphasizing the psychosocial benefits of sports and in providing the necessary information to meet the needs of the child. For children with limb deficiencies, the recommendations for sport participation must be individualized [12]. In addition to providing essential information on physical abilities and sporting opportunities, individualized recommendations also involve tailored advice on specific (sport) prostheses.
Limitations
Although a considerable number of children with LLD in the Netherlands were investigated regarding their sports participation, the results of this study should be interpreted with some caution due to the heterogeneous sample. Generalisation of the study results may be hindered due to a selection bias within the sample since the more active and fitter children with LLD expressed a higher interest in participating in this study. The questionnaire used was not validated beforehand. Therefore, comparison with other studies should be done with caution. The questionnaire contained simple yes-no questions which were easy to answer for all participants. Concerns may be raised regarding the specificity of the answers as the information disclosed by participants was voluntary without prompting. The answers could have been more detailed if the questions had been more specific. Another concern is that it is not known to what extent parents helped in completing the questionnaire.
Conclusion
This study indicates that the sports participation of Dutch children with LLD is comparable to healthy peers and appears not to be restricted due to the prosthetic dependency of most of these children. The majority of children and adolescents participated in the sports of their preference, with the caveat that some children experienced limitations in PP (running) and PE (endurance) with a negative influence on their sports participation. These findings warrant further research into interventions improving PP in children and youth with LLD, including the possibilities of using an advanced (sport) prosthesis. The bottom line remains that encouraging sports participation is a crucial element of medical rehabilitation in children with LLD given the psychological and physical benefits. A comprehensive approach also includes communication and collaboration with school physical educators and coaches about ways to include children with prostheses and orthoses in gym class and sports.
Footnotes
Acknowledgments
Our gratitude goes out to the children and adolescents who participated in this study. We would like to thank prof. dr. J.W. Gorter for editing the manuscript. All parents and children in the figures have given permission for their photos to be published.
Conflict of interest
The authors have no conflict of interest to report.