
Abstract
PURPOSE:
This pilot study sought to describe the perspectives and experiences of survivors of pediatric traumatic brain injury (pTBI), their caregivers, and the medical professionals who serve them.
METHODS:
Thirteen people participated in semi-structured interviews: five survivors of pTBI, their primary caregivers, and three medical professionals who work with persons who have sustained pTBI. The study involved a prospective, qualitative, participatory action research model with convenience sampling. All interviews were transcribed and thematic analysis identified central concepts within and between groups. Additionally, the Consolidated Criteria for Reporting Qualitative Research (COREG) were applied.
RESULTS:
This study found that survivors of pTBI and their caregivers commonly noted later developing issues, social challenges, and difficulty in post-rehabilitation transitions. In addition, both caregivers and medical professionals reported the need for improved follow-up with survivors, evidence-based research, and medical and therapy providers with specific training on pTBI.
CONCLUSIONS:
The perspectives provided by key stakeholders in this pilot study identify common themes that should be central to driving innovation in rehabilitation research and clinical care.
Introduction
Traumatic brain injury (TBI) is widely accepted as the leading cause of acquired disability for children in the United States [1, 2]. An estimated 29,000 new children in the US each year demonstrate persistent and significant changes in social, behavioural, cognitive, and physical functioning following a TBI [3, 4, 5]. These persistent changes are associated with difficulties in long-term health, engagement in functional community roles, and integration into society [6, 7]. In addition, research now suggests that sequelae of TBI may represent a chronic, continually evolving disease process rather than simply an acute injury that resolves over the short-term [8, 9, 10]. This is especially concerning for individuals injured during childhood and adolescence given that these survivors must manage the long-term impact of their TBI over the course of their lifespan.
Gaps in identification and service utilization show that our current system of care is not sufficiently working for children who sustain TBIs, thus diminishing the likelihood of long-term health and function for these individuals [10, 11]. Past studies have shown under-identification of children and adolescents admitted to the hospital with TBI and/or that these patients and families are not linked with appropriate services when they are hospitalized [12, 13, 14]. Additionally, families do not consistently return for recommended follow-up visits following an admission for pediatric TBI (pTBI [15]. Further studies have identified under-utilization of support services that can help to promote health and function for children and adolescents with TBI and their families, particularly in the chronic stages of injury [16, 17, 18, 19, 20, 21]. Children with TBI are also dramatically under-identified in our school systems [10, 21, 22]. Current literature indicates that less than half of students who have survived a pTBI are receiving educational supports [22, 23, 24, 25].
Additionally, for medical professionals who care for children and adolescents with TBI, evidence-based practice guidelines are limited [26, 27, 28] and inclusion of key stakeholders to develop intervention and research priorities is uncommon [29, 30, 31, 32, 33, 34, 35, 36, 37]. A group of papers from Roscigno and colleagues [30, 31, 32] described an ethnographic study that collected data from survivors of pTBI and their parents. These semi-structured interviews identified themes related to survivor experiences, perceptions, and quality-of-life, and they demonstrated that children as young as 8-years-old can share experiences related to their TBI [34]. Roscigno et al. also collected and described parent perceptions related to school reintegration [31], changes to the family unit [30], and medical professional-parent communication [32]. Roscigno and colleagues concluded that extensions of their work were needed that included the experiences of children injured at younger ages, perceptions of recovery and needs further-post injury, larger samples, and medical professionals as key stakeholders. This important body of work established a foundation for stakeholder-driven research related to pTBI.
When individuals do not receive appropriate rehabilitation services post-injury and experience barriers that prevent their adherence with rehabilitation recommendations, the long-term health and function for those survivors could be negatively impacted [38]. Due to the fact that the voices of survivors of pTBI and their families are rarely heard in the literature [30, 31, 32, 33, 35, 36, 37, 39], we are not able to account for the most ecologically valid, stakeholder-driven needs related to long-term rehabilitation following pTBI. The perspectives of key stakeholders will help to define the most salient factors related to medical management and rehabilitation, identify where gaps exist in service provision, and ensure that these perspectives inform future clinical research. As a result, the negative impact to overall quality-of-life caused by a pTBI may be minimized. The theory driving this research is consistent with the recommended shift in focus from impairment-based dysfunction to participation-focused intervention [40]. Currently, this perspective is largely missing from the overall approach to pTBI rehabilitation [41, 42].
The objective of the current study was to collect pilot data to inform a more comprehensive look at the perspectives and experiences of key stakeholders related to pTBI (survivors, their caregivers, and medical professionals) in order to examine areas for innovation in research and clinical service delivery. Researchers were interested in understanding the perspectives of these key stakeholders as related to their experiences surrounding pTBI. The objectives motivating this study were to:
Describe the perceptions of caregivers and survivors of pTBI based on experiences since the time of the injury. Describe the perceptions of medical professionals who work with the survivors of pTBI.
This exploratory study primarily used a qualitative, participatory action research model with convenience sampling. The methods reported are consistent with the Consolidated Criteria for Reporting Qualitative Research (COREG) [43].
Participants
Approval from the Institutional Review Board was obtained before any research activities were conducted. To recruit survivors and caregivers, five families that include a child with TBI and had previously expressed interest in research activities were contacted via phone to participate. The first author provided survivors and their families with information regarding the purpose of the study and clearly stated the interests of the researchers. All participants agreed to be included in the study, and therefore recruitment did not yield non-participants. All persons signed the appropriate consent/assent forms prior to participation.
Demographic and injury data for survivors and caregivers
Demographic and injury data for survivors and caregivers
Medical professional history
To be included, the survivors of pTBI were between the ages of 7 and 25-years old at the time of enrollment, had a diagnosis of moderate-to-severe TBI that required hospitalization of at least one night, and were injured between the ages of 1 and 18 years. Hospital admissions for all five participants included inpatient rehabilitation. To be included, a caregiver had to have been actively involved throughout the recovery and rehabilitation process for the survivor (see Table 1 for demographic information for all survivors and caregivers).
To recruit medical professionals with specialty in pTBI, the pediatric rehabilitation team at a large pediatric hospital was contacted about the opportunity to be interviewed for this study. The first three medical professionals who responded were included. Medical professionals were required to provide assessment and/or treatment for survivors of pTBI as part of their clinical responsibilities within the last year. A speech-language pathologist, recreational therapist, and registered nurse were included in this study (see Table 2).
The semi-structured interview format used in this study consisted of open-ended questions, probes, and follow-up questions (see Table 3), which ensured the interview was driven by the participants’ experiences and not biased by the researcher [44, 45]. The interviews were designed to examine participants’ responses regarding their care plan and needs related to cognitive, behavioural, and social supports in greater depth and without potential bias imposed by the wording of interview questions. Interviews were conducted by the first author, a researcher-clinician with over ten years of experience providing clinical services to the pTBI population. All participants were known to the interviewer via the rehabilitation process. Interviews were audio recorded and later transcribed. To ensure inter- and intra-rater reliability of transcription, sampling transcription checks (20% of interviews) via re-transcription were completed.
Prompts for semi-structured interviews, by stakeholder group
Prompts for semi-structured interviews, by stakeholder group
Thematic content analysis.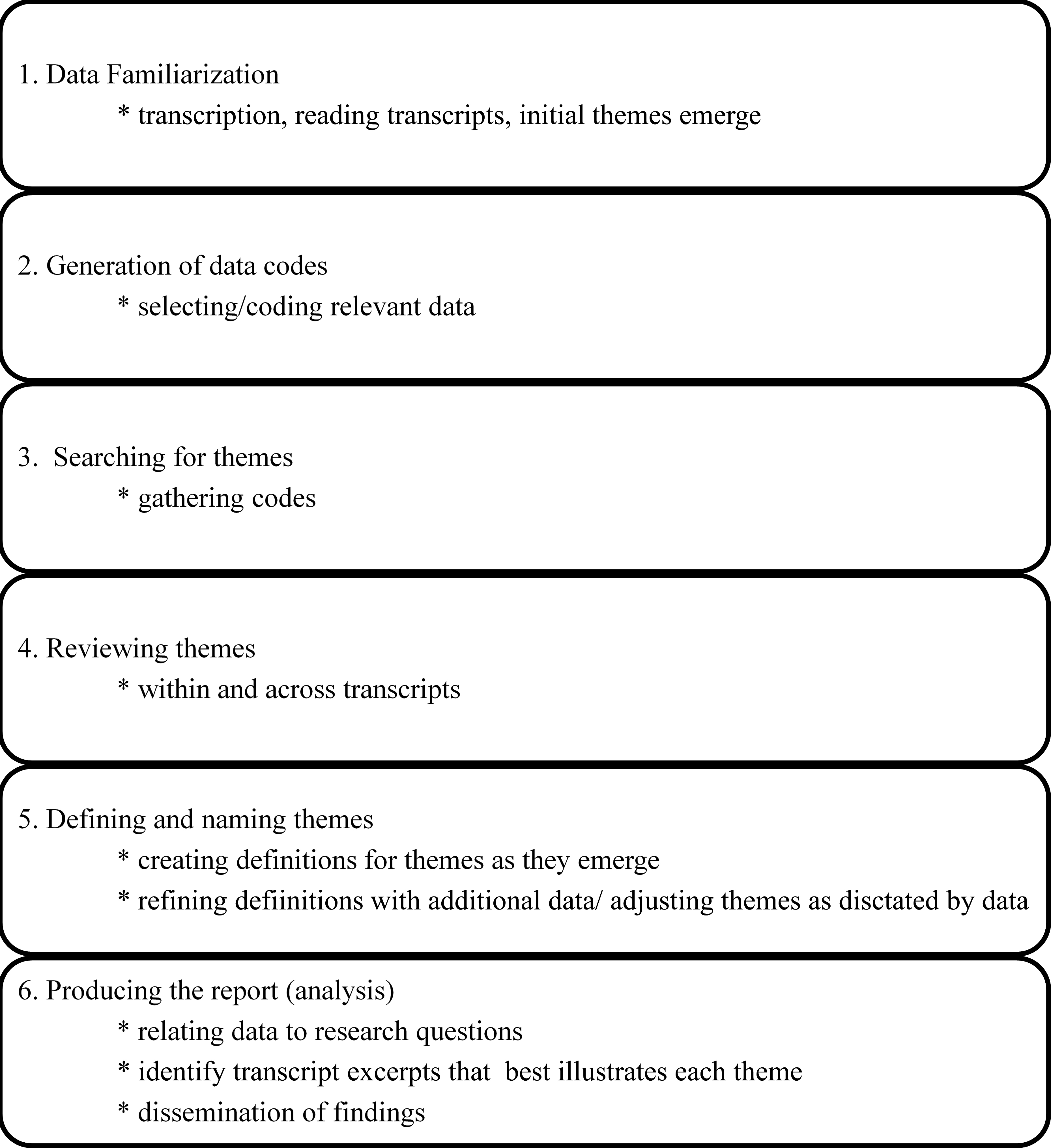
After transcription, two second-year graduate students in speech-language pathology independently reviewed transcripts and grouped comments into categories based on initial perceptions of similarity using thematic content analysis. Closely linked to grounded theory, thematic content analysis is a qualitative data analysis approach that provides a framework for identifying, analyzing, and reporting patterns within a dataset [46, 47]. Reviewers identify patterns in the dataset, based on the importance or prevalence of the data, and combine them to create themes [46, 48]. Thematic analysis is used to examine the perspectives of participants, specify their similarities and differences, and elicit unanticipated information from the participants [47]. In the current study, thematic content analysis was conducted using the six-phase approach outlined by Braun and Clarke [46] (Figs 1 and 2).
Transcription procedure and reliability.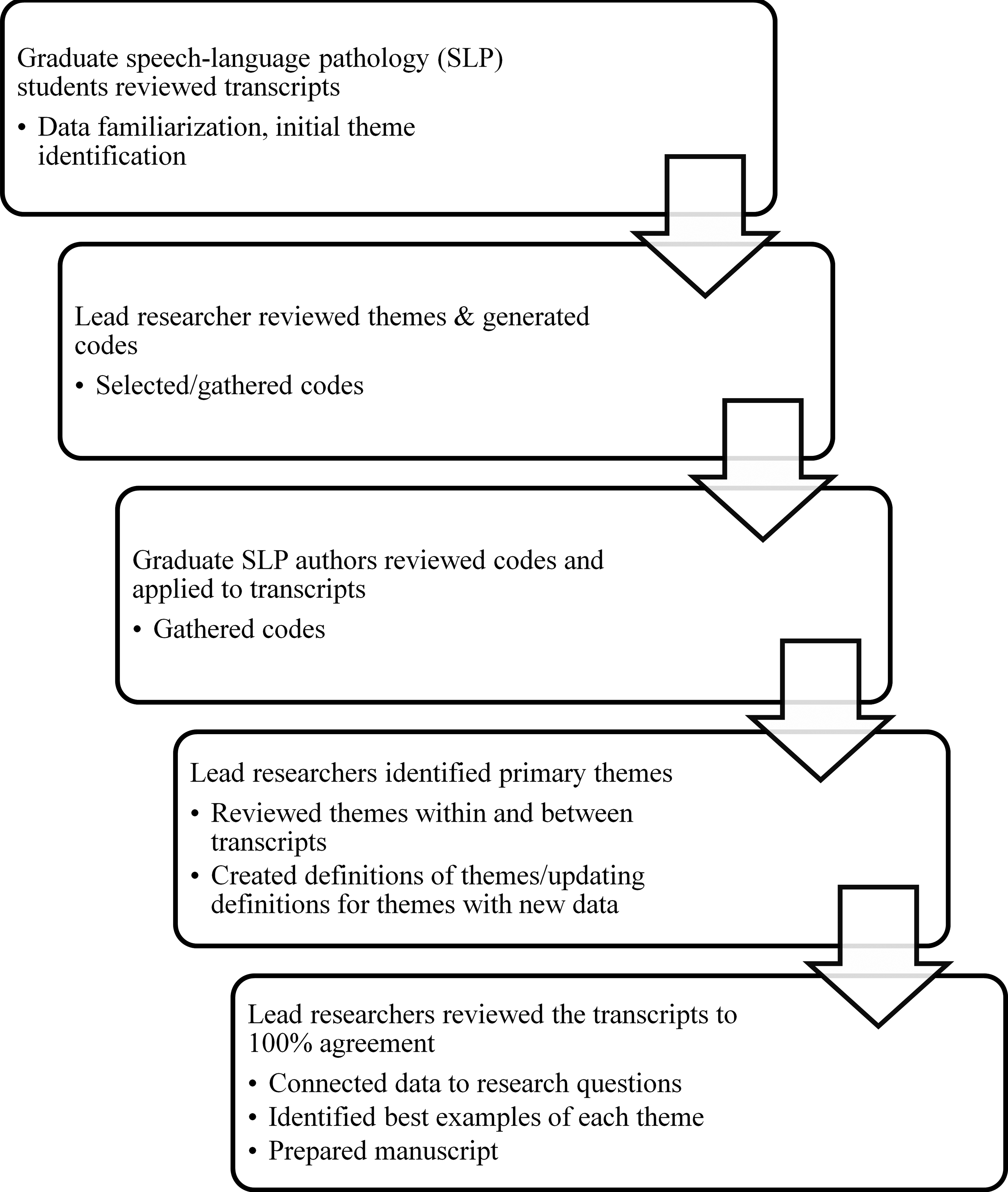
The last author, a female Ph. D. researcher-clinician with a twenty-year history of working with the TBI population, then labeled initial categories into preliminary themes. Each of the graduate students then re-analysed utterances from each transcript to fit them into these five themes, along with a category for miscellaneous statements. Then, the two lead researchers (first and last authors) created a seventh theme that was not identified in the preliminary reviews. The lead researchers independently reviewed, then conferenced to compare the transcripts utterance-by-utterance, reaching 100% consensus on how utterances were labeled.
Following the analysis of all interview transcripts, the following themes were identified for both caregivers and survivors: experiences with medical personnel, later developing issues, hope versus reality, next steps, social issues, discharge, and miscellaneous. The following themes were identified for medical professionals: population characteristics, evidence-based patient centered care, staffing/teamwork, follow-up, and miscellaneous. Figure 3 shows the coding tree for these themes.
Coding tree for interviews.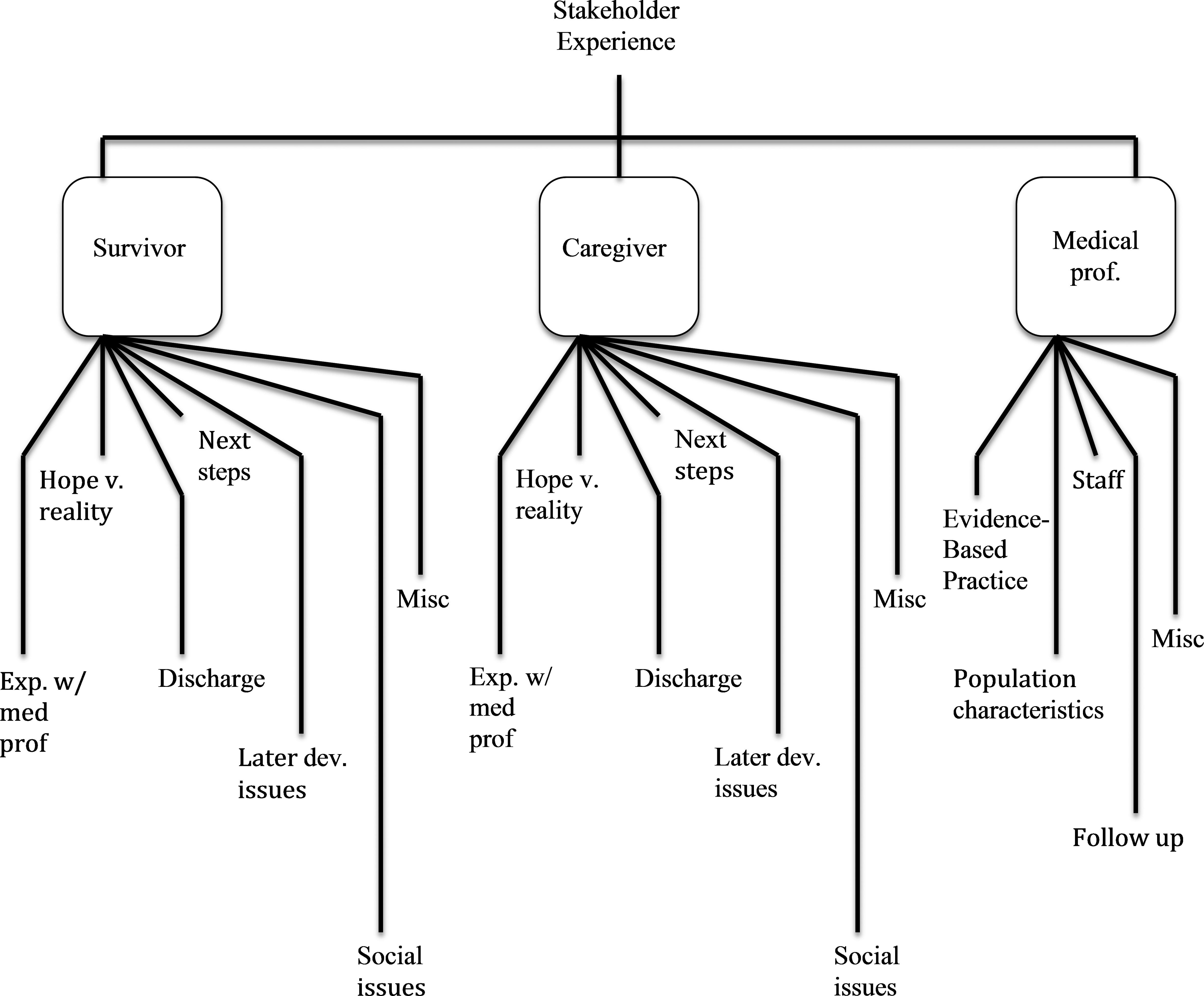
Examples of caregiver quotes for each identified theme
Examples of survivor quotes for each identified theme
Experiences with medical personnel
[References to caregiver and survivor quotes refer to Tables 4 and 5 respectively. See also Figs 4 and 5.] Caregivers most frequently discussed their experiences with medical personnel, accounting for 18.1% of total comments (range
Caregiver comments by theme.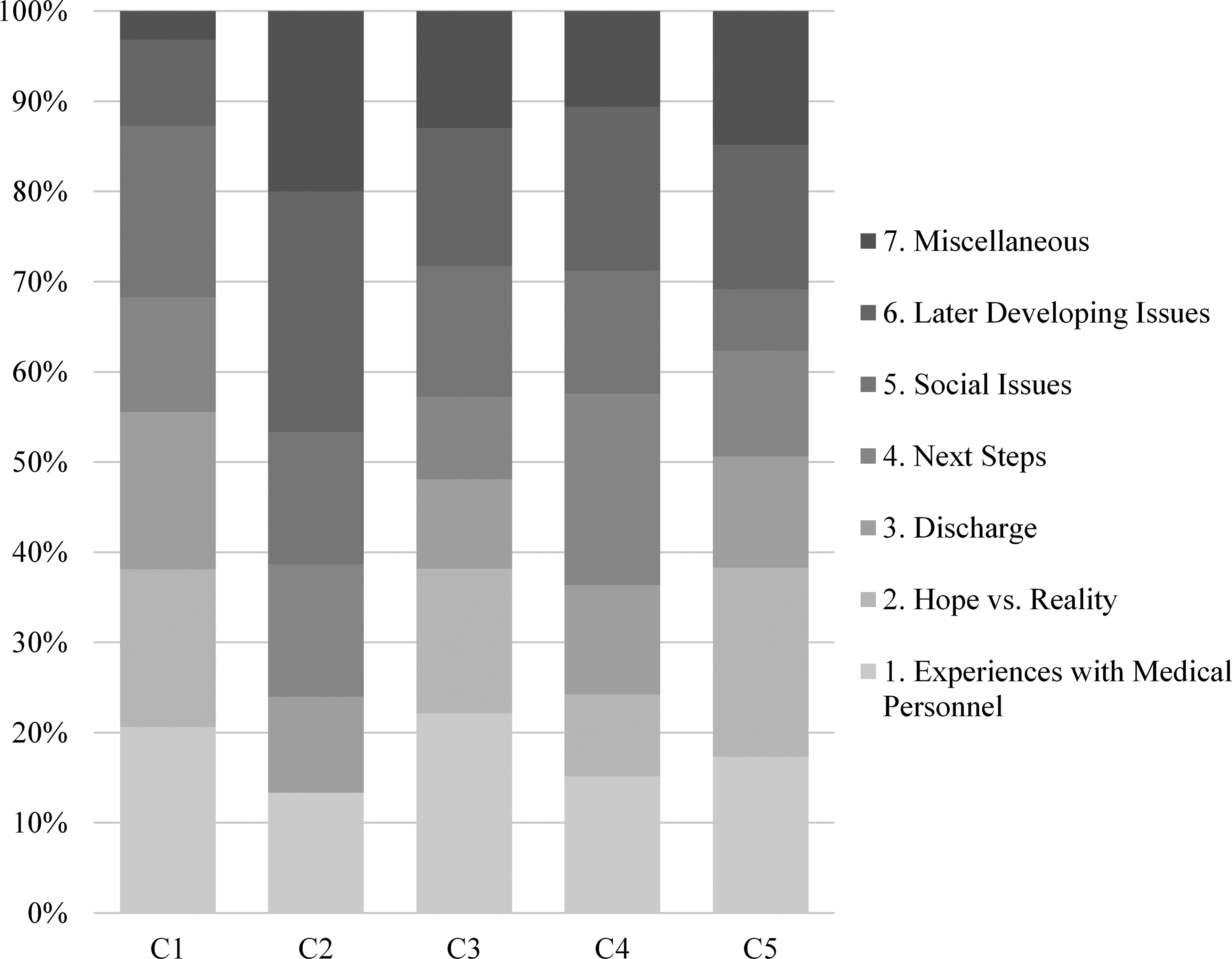
Survivor comments by theme.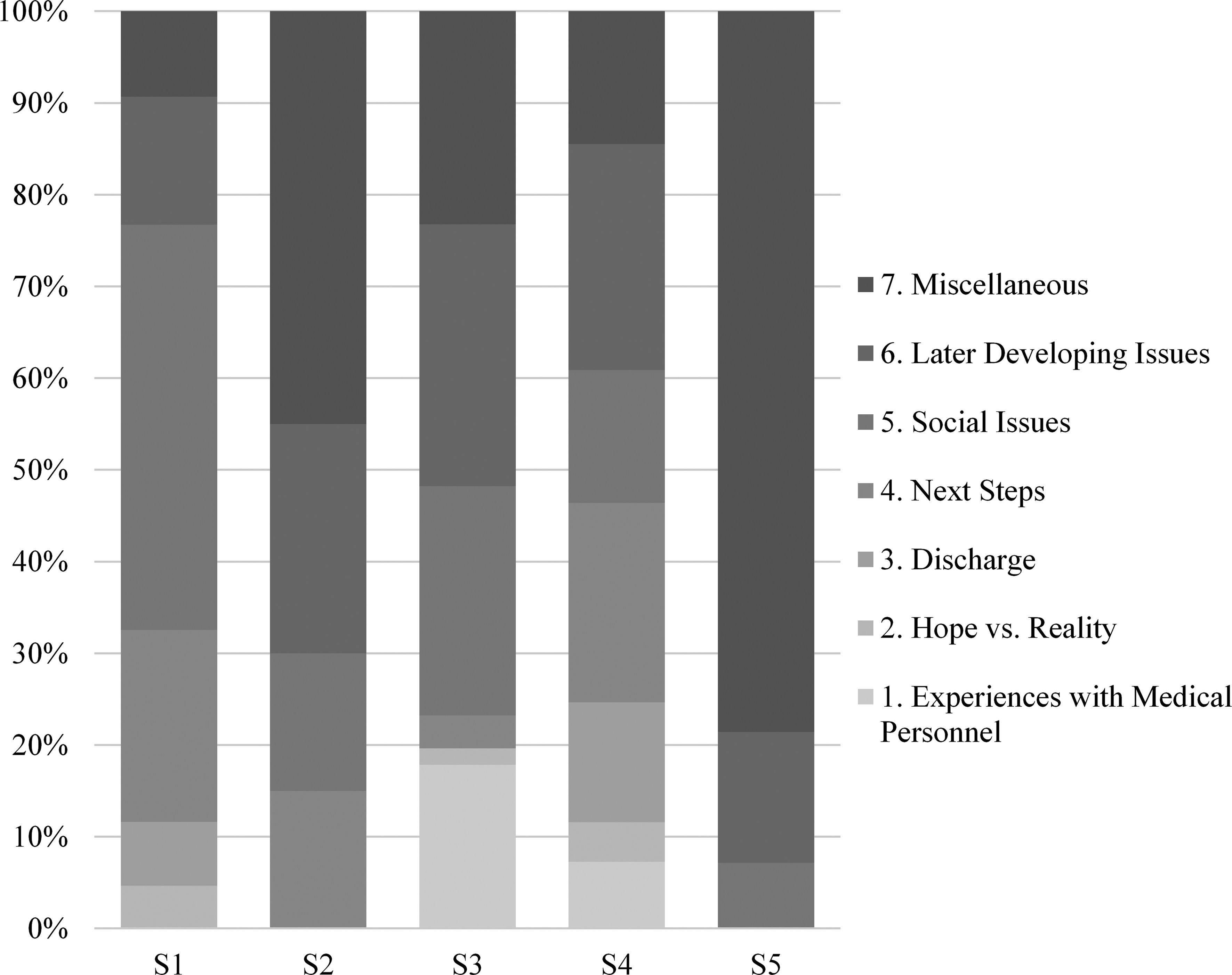
Survivors discussed their experiences with medical personnel less frequently. Survivors often commented that they did not remember the early part of their hospital stay, but did comment on interactions with the rehabilitation staff with primarily positive regard. This was the fifth most common theme expressed in survivor interviews, accounting for 7.4% of all comments (range
Examples of medical professional quotes for each identified theme
For caregivers, the second most frequently discussed theme related to issues that developed well after discharge from inpatient rehabilitation. This theme accounted for 16.9% of total caregiver comments (range
For survivors, later developing issues experienced after pTBI were the third most commonly discussed theme, accounting for 22.8% of total survivor comments (range
Hope versus reality
The third most common theme discussed by caregivers related to the competing experiences of hope and reality. Caregivers commented frequently on the impact of receiving difficult news from the medical staff (C1[a]) and the need to continue to hope for the best possible outcome for their child despite indications to the contrary (C1[b] and C4). Caregivers also spoke about how medical professionals could provide hope while also remaining realistic (C3 and C5). This theme accounted for 14.5% of total caregiver comments (range
For survivors, on the other hand, hope versus reality was the theme discussed with lowest frequency. Comments addressing this theme accounted for only 3.0% of total survivor comments (range
Next steps
Caregivers discussed issues related to transitioning from inpatient rehabilitation to home and school in 12.9% of total comments (range
Survivors discussed these issues in 14.4% of total comments, making it the fourth most commonly discussed topic (range
Medical professional comments by theme.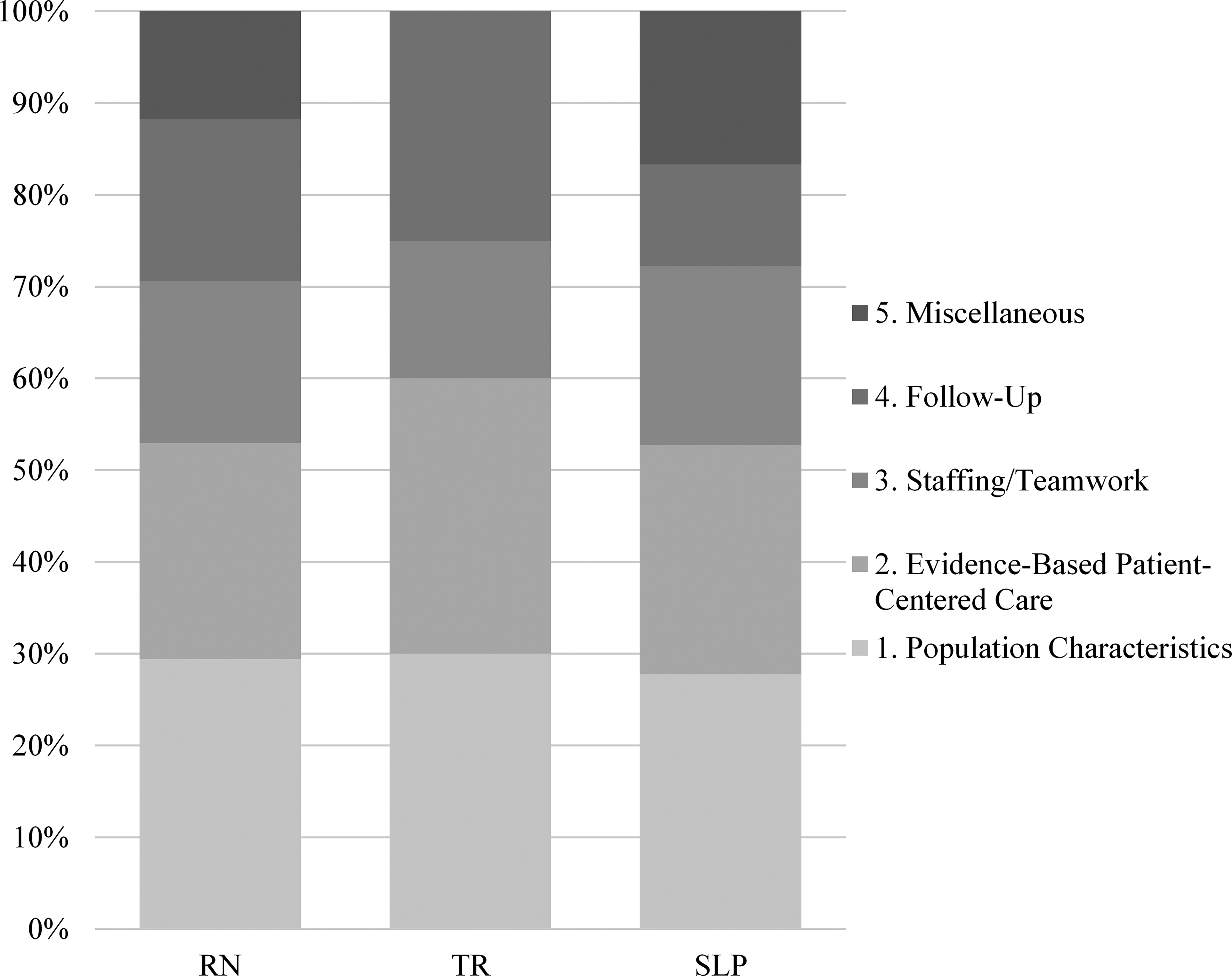
Social challenges related to pTBI were raised in 12.5% of caregiver comments, making this theme the sixth most commonly discussed issue (range
Survivors, on the other hand, discussed social issues related to pTBI most frequently. Nearly one quarter of all survivor comments related to this theme (23.3%; range
Discharge
Issues and topics related to discharge from inpatient rehabilitation were the least common topic discussed during caregiver interviews. Discharge-related comments accounted for 12.1% of all caregiver comments (range
Only two survivors made discharge-related comments that focused on the therapy staff preparing the survivor to go home. This was the second-to-least frequent theme mentioned by survivors and accounted for only 5.9% of their total comments (range
Miscellaneous
Caregivers and survivors provided a range of comments that did not occur frequently enough to create distinct categories. Caregiver comments were designated as miscellaneous in 13.1% of cases, making it the fourth most commonly occurring theme (range
For survivors, miscellaneous comments were the second most commonly occurring theme, at 23.3% of total comments (range
Medical professionals
Population characteristics
[See Table 6 and Fig. 6.] For medical professionals, the theme most commonly occurring during interviews related to the challenges and rewards of working with survivors of pTBI and their families. Providers uniformly discussed the energy that they derive through witnessing the progress made by many pTBI survivors during their relatively short hospital and rehabilitation stay. This theme accounted for 28.8% of total comments (range
Evidence-based patient centered care
Across disciplines, the perceived lack of evidence-based approaches for assessment and treatment of pTBI was highlighted, making it the second most discussed theme for medical professionals. These comments accounted for 26.0% of all interview comments. By profession, these comments accounted for the following frequencies: Registered Nurse (RN)
Staffing/Teamwork
During interviews with medical professionals, 17.8% of total comments related to staffing and issues surrounding the interdisciplinary rehabilitation team (range
Follow-up
The providers uniformly commented on the desire to understand what happened with survivors and identified the need for creative approaches to be able to follow survivors after discharge. Follow-up was discussed in 16.4% of total interview comments (range
Miscellaneous
There were few miscellaneous comments within the medical professional group, which often related to the professionals’ description of their work experience. For medical professionals, comments were determined to not fit the established themes in 11.0% of cases (range
Discussion and clinical implications
When a child experiences a TBI, there is significant stress within the family unit [49]. Past research has identified several familial psychosocial factors that can impact the overall outcomes for survivors of pTBI, including family stress [50, 51], access to resources [50, 52], and parental coping style [51, 53]. By extension, if psychosocial risk influences outcome, it would be reasonable to consider that the actual lived experience of the caregiver and survivor of pTBI might influence the ultimate outcome of the survivor. For example, a person’s feelings about their medical experience or the information received about pTBI might impact the likelihood of seeking services once the child returns to school. Yet, there is little discussion in the literature about the survivor and family experience following pTBI and how these experiences might relate to unmet needs [34, 36, 37]. In the current study, nearly 50% of caregiver comments fit into the first three themes: experiences with medical professionals, later developing issues, and hope versus reality. These findings are consistent with past reports suggesting that families require significant support not just during the acute stages of recovery following pTBI, but during the chronic stage as well [2, 18, 19, 54].
Discussions about later-developing issues were pro- minent for both caregivers and survivors. Caregivers specifically discussed how these issues created challenges, often related to not knowing when, where, or how to seek help to address identified needs. The frequency of these comments by both groups of stakeholders is consistent with past research discussing unmet needs following pTBI [10, 17, 18, 19, 23]. Survivor comments from these interviews also emphasize the importance of the social implications of pTBI on the survivor, especially during adolescence. Since there are few evidence-based interventions to assist teens in this realm, the frequency of these comments highlights how research and clinical practice are not addressing a need that is important to the stakeholders. As the lived experience of key stakeholders matches the growing body of literature demonstrating that children with pTBI may demonstrate delayed consequences of the injury on later developing skills, the medical and educational communities must respond with improved care pathways that improve both access to and receipt of services for children with pTBI and their families.
Consistent with gaps in care identified in the 2018 Report to Congress on the Management of TBI in Children [19], caregivers and medical professionals interviewed for this study stressed that consistent care providers and those with specific knowledge of pTBI are optimal to assist families and survivors of pTBI during all stages of recovery. The complex issues associated with long-term recovery following pTBI indicate how implementation of a medical home concept might improve the long-term care following pTBI. Previous literature examining other pediatric chronic conditions [54, 55] suggests that a consistent medical care team that includes supports for the family decreases unmet needs and facilitates transitions into adulthood. Since unmet needs are a particular challenge following pTBI, improvements to the continuum of care following pTBI would be a direct response to the stated needs of key stakeholders but also help to ameliorate existing problems related to service provision and access.
Additionally, the inclusion of stakeholder perspectives could be a critical and missing ingredient to identifying best-possible evidence-based practice approaches in pTBI. Medical professionals from different disciplines interviewed for this study all identified the lack of evidence as a particular challenge to providing good care to children with pTBI. These comments are supported by studies that demonstrate variability in the services available to children and the quality of those services [56]. Also, despite having only three disciplines represented in this pilot study, these comments echo findings from a recent Canadian study where 15 individuals from six healthcare professions expressed similar thoughts in focus group meetings [57]. The perspectives of key stakeholders should help researchers and clinicians identify the most salient and impactful directions for future work.
Limitations and future directions
While designed as a pilot study, the generalization of the findings presented here is limited by small sample size. Enlarging the sample would allow for greater characterization of comments that were included as miscellaneous in this study and allow for minor theme identification per COREG suggestions [43]. In a larger study, it will be critical to include persons from minority groups to allow for greater diversity of perspectives. It is likely that persons from non-white groups might report different experiences and perceptions of care following pTBI, as disparities in care and disability have been found in non-white patient groups [58]. Future research should also include representation from other disciplines involved in caring for children with pTBI. Additionally, since research shows that children admitted to inpatient rehabilitation are more likely to have hospital-to-school transition planning and establishment of outpatient therapies [59], we must expand this work to include those patients who do not receive acute rehabilitation. This is especially critical because it is estimated that only 4% of children who sustain a pTBI are admitted to an inpatient rehabilitation unit [60]. Lastly, as we move forward and increase sample size, we will incorporate the iterative process of allowing participants to review their transcripts and provide feedback on the findings.
Conclusions
The consideration of the perspectives of key stakeholders affected by pTBI gives depth to the trends that are present in the literature and provides insights into how our current system of care can be improved for all stakeholders. Specifically, caregivers and survivors are in need of an improved continuum of care that supports later developing challenges that arise long after hospital discharge. Additionally, survivors require greater support in managing the social challenges they may face following a TBI, and medical professionals are in need of a stronger evidence-base to support their clinical practice. Despite the wide variations in age and injury severity of the participants included in this pilot study, there are commonalities that appear when taking into consideration stakeholder perspectives related to pTBI. These perspectives should be central to driving innovation in rehabilitation research and clinical care.
Footnotes
Acknowledgments
The authors wish to thank the participants who shared their experiences and perspectives for this work, and Allison Gonzalez for her assistance with data management.
Conflict of interest
The authors have no conflict of interest to report and there is no funding associated with this work.