
Abstract
PURPOSE:
The objective of this study was to describe the knowledge, attitudes, and practices related to caring for youth with SB within a statewide pediatric primary care medical home network.
METHODS:
Health care professionals who were members of the Pennsylvania Medical Home Program (PAMHP) statewide network were surveyed on sociological demographics, confidence in and knowledge of topics that impact the spina bifida (SB) population, education on SB, designating responsibility of care, tasks completed in the office, and transition from pediatric to adult care from October 2016 through November 2016.
RESULTS:
Among 67 respondents, 78%believed counseling families/caregivers about the impact of SB on everyday life was a shared responsibility between primary care physicians (PCP) and SB clinics. Eighty five percent of participants indicated they had exposure to SB through clinical courses or didactics in training but only 54%of participants felt knowledgeable on the impact of SB on everyday life.
CONCLUSION:
Findings suggest a need for increased educational efforts, improved awareness of SB, and access to evidence-based guidelines for PCPs to promote accessible and coordinated care to individuals with SB.
Introduction
The Patient and Family Centered Medical Home (PFCMH) approach to care is the standard of primary care delivery built upon the framework of accessible, continuous, comprehensive, family centered, coordinated, compassionate, and culturally effective care [1]. The goal of the PFCMH is to provide comprehensive primary care that facilitates partnerships between individual patients and their personal physicians, and when appropriate, the patient’s family [1]. Coordination of care through the PFCMH is associated with improvement in the patient and family care experience, decreased health care costs, and reduction in fragmented care [2].
The PFCMH seeks to provide effective and efficient health care for all children including children and youth with special health care needs (CYSHCN). CYSHCN (0–21 years old) are defined as “children with special health care needs who have or are at increased risk for chronic physical, developmental, behavioral, or emotional conditions and who require health and related services of a type or amount beyond that required by children generally” [3]. Nearly 20%of U.S. children under 18 years of age have a special health care need [3]. CYSHCN are a diverse group of children including those diagnosed with intellectual and physical disability. Examples include Down syndrome, cerebral palsy, and spina bifida (SB).
SB is the most common permanently disabling birth defect that is compatible with life in the United States, with an incidence of 1,500–2,000 births per year [4]. SB is a neural tube defect resulting in incomplete closure or development of the spinal cord and surrounding structures, leading to varying degrees of intellectual and physical disability [4]. A child with SB will need care not only from primary care physicians (PCPs), but also from specialists such as physiatrists, neurosurgeons, orthopedic surgeons, and urologists as well as supportive services from physical and occupational therapy, social work, nurse care coordinators, community health workers, dietitians, and medical equipment providers. Due to the need for complex and coordinated care, these children often receive care in multidisciplinary clinics and programs, many of which are affiliated with urban teaching hospitals.
Despite the need for both primary care and specialty care, many adults with SB lack access to both complex and coordinated care. A retrospective study examining hospitalizations of individuals with SB in 2004–2005 demonstrated that 76%of patients with SB who were hospitalized did not have or could not identify a PCP [5]. Currently, the majority of individuals living with SB are now older than 18 years of age. Over half of adults with SB reside in states lacking practices/clinics specializing in the care of people with SB [6]. Lack of access to care may result in complications from secondary conditions that are otherwise preventable. Approximately one third of hospital admissions of adults with SB are a result of potentially preventable conditions, primarily infections [5]. A slightly higher proportion (35.7%) of hospitalizations resulting in death have a primary diagnosis of a potentially preventable condition [5]. The inability to prevent secondary medical conditions is contributing to the morbidity, mortality, and cost of health care and may therefore justify the implementation of the PFCMH [5, 7].
Given the medical, community, educational, and support services necessary to care for individuals with SB, responsibilities of care should be shared and cohesive between the specialty clinicians, PCP, and other care team members. The sharing of responsibilities requires team-based goal setting across multiple providers using appropriate resources to provide multi-disciplinary care. There is a paucity of research evaluating the perspectives of PCPs and other providers for caring for children with SB.
The Pennsylvania Medical Home Program (PA MHP) is a statewide medical home primary care network housed at the Pennsylvania Chapter of the American Academy of Pediatrics [8]. A medical home is a model of care delivered or directed by well-trained physicians who provide primary care and help to manage and facilitate essentially all aspects of pediatric care while developing a partnership with the patient and family [1]. Members of PA MHP practice network include over 80 primary care practices across Pennsylvania engaged in quality improvement activities, behavioral health, and care coordination [9, 10]. The PA MHP practice network frequently engages in educational activities including monthly webinars, bi-yearly conferences, and technical assistance on a variety of topics including but not limited to quality improvement, autism, family centered care, cultural effectiveness, epilepsy, and many other topics relevant to caring for children and youth. Little is known about the educational needs and other resources desired by practitioners in primary care settings who care for children and youth with SB. As such, the purpose of this study was to use a cross-sectional design to describe the knowledge, attitudes, and practices regarding facilitators and barriers to caring for children and youth with SB in pediatric primary care settings among the members of PA MHP.
Methods
PA MHP is a statewide quality improvement program developed in 2001 and has trained staff at over 170 pediatric and adult primary care practices throughout the Commonwealth of Pennsylvania in the adoption, implementation, and evaluation of medical homes. [11] This project was determined to be an exempt study and approved as a quality improvement project by Drexel Institutional Review Board. Approval was obtained from the Quality Improvement Committee to publish the results. Health care professionals who were members of the PA MHP statewide network were surveyed [See Appendix A] from October 2016 through November 2016. Participants were contacted through email and were able to complete the survey online as well as in person at the PA MHP conference in Harrisburg, PA in October 2016. The survey collected data on sociological demographics, confidence in and knowledge of topics that impact the SB population, education on SB, designating responsibility of care, tasks completed in the office, and transition from pediatric to adult care. Email reminders were sent out three times to members of the PA MHP practice network.
Measures
Demographics
Respondents indicated their role in healthcare, location of their practices, and type of practice (private, community health center, federally qualified health centers (FQHC), rural health clinic (RHC), academic center, hospital system owned, or other), years of training, and distance from a tertiary or quaternary pediatric hospital.
Knowledge and confidence on topics related to SB
Respondents were asked to rate both their knowledge and confidence in caring for a child with SB (very knowledgeable, knowledgeable, not very knowledgeable, and not at all knowledgeable).
Educational history of SB
Respondents described the education they received on the topic of SB as well as their clinical experience in providing care to individuals with SB. They were also queried on the timing and setting of this education.
Designating responsibility of care
Respondents reported which clinician or organization they believed should be primarily responsible for certain activities involved in treating a child with SB. The options were PCP office, SB clinic, shared responsibility between PCP and SB clinic, and “other” which included Spina Bifida Association (SBA) or Pennsylvania Chapter of the American Academy of Pediatrics (PA AAP).
Transition of care
Respondents detailed their processes in place for transition of care from childhood to adult care. Participants also reported challenges that exist in the transition process. In addition, respondents were asked whether they used the Guidelines for Spina Bifida Health Care Services throughout the Lifespan.
Future education
Respondents indicated their preferred method of receiving future educational materials using the following: online continuing medical education activity hosted on central website, webinar, in-person community lecture, updates on practice guidelines, handouts/materials delivered to practice, and “other.” Also, they were able to select all that applied.
Analysis
A descriptive analysis was used to report results of questions as counts and frequencies. Responses to the question about knowledge of and confidence in topics related to SB were collapsed into binary categories for reporting in tables.
Results
Demographics
A total of 67 out of 120 respondents completed the survey (56%response rate). Most were physicians (39%) and worked in a private practice (44%). Respondents identified as nurse practitioners/physician assistants (4%), nurses (24%), and other (33%). Those who reported as ‘other’ identified themselves as case or social workers, medical assistants, care coordinators, and office managers. The majority of practices were located in urban (36%) or suburban (36%) areas and located within 30 miles (60%) of tertiary or quaternary pediatric hospital centers (Table 1).
Demographics of Respondents (n = 67)*
Demographics of Respondents (n = 67)*
*Missing responses excluded
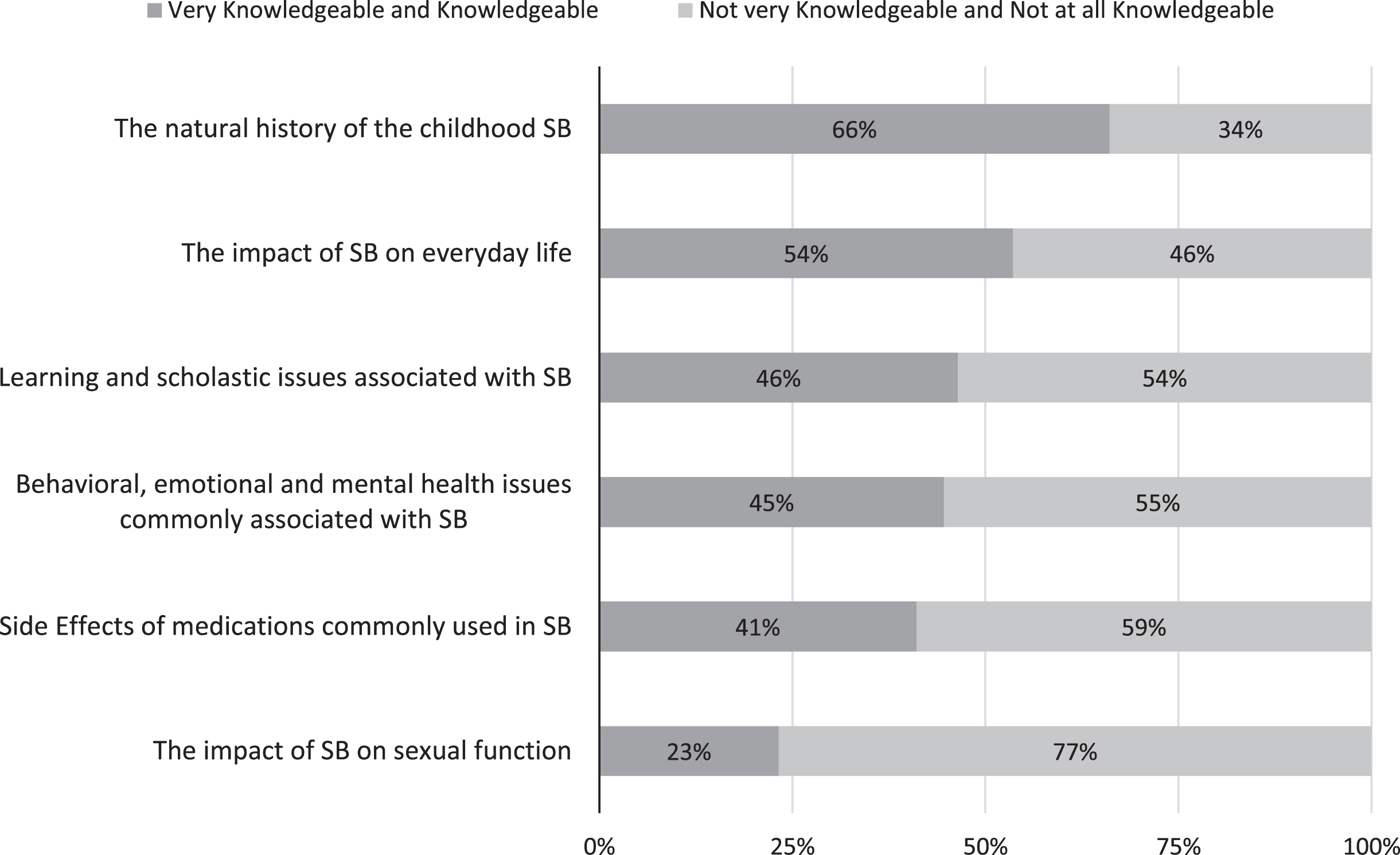
Responders’ Knowledge of Topics Related to SB.
The natural history of childhood SB and the impact of SB on everyday life were the best understood topics with 66%and 54%, respectively, reporting either “very knowledgeable” or “knowledgeable.” The impact of SB on sexual function was the least understood topic with just 23%reporting either “very knowledgeable” or “knowledgeable” (Fig. 1).
Respondents reported they were “very confident” or “confident” the most often for their ability to carry out screening for behavioral, emotional, and mental health issues (83%), assessing for school and learning problems (83%), and providing primary care (81%). Respondents reported feeling “very confident” or “confident” the least often for their ability to link families to support groups or to other families who have children with SB (49%), to discuss contraception and sexuality (48%), and to communicate with families and caregivers about the impact of SB on everyday life (45%) (Fig. 2).
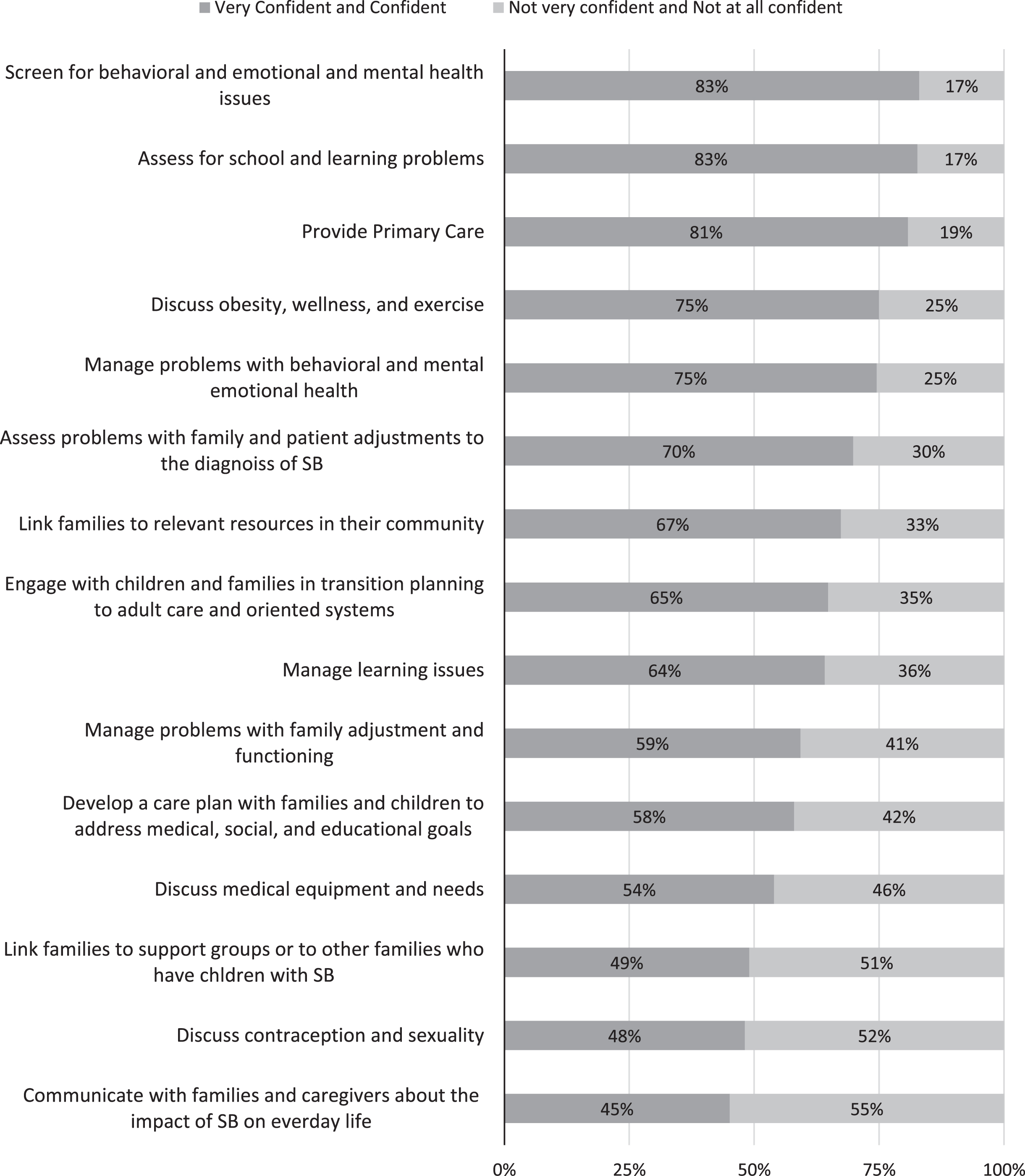
Responders’ Confidence on Topics Related to SB.
Most respondents reported they learned about SB during their education (66%). This was either through formal didactics, clinical rotations, or both. About one-third (34%) reported they had not learned about SB at any point in their education. For those who responded that they had learned about SB through means that were not clinical rotations or formal didactics, the following explanations were indicated: fellowship in special needs, through the care of a large number of children with SB, and during work on inpatient hospital units.
Designating responsibility of care
Over 50%of respondents reported that all activities listed should be shared responsibilities between the PCP and SB Clinic. The activities reported most frequently as shared responsibilities were: counseling families and caregivers about the impact of SB on everyday life (78%), counseling families about adjustment issues after SB diagnosis (72%), discussing patient plans for transition and related issues (71%), and discussing/helping patients plan for transition and related issues (71%). For respondents who indicated activities were the sole responsibility of either the PCP or the SB clinic, the following was reported: “discussing sexuality and contraception” (34%PCP and 10%SB clinic) and “educating professionals in schools or other settings about a child’s condition and support needs in school” (21%PCP, 21%SB Clinic, 5%SBA or PA AAP). Further details can be found in Table 2.
Designating Responsibility of Care
Designating Responsibility of Care
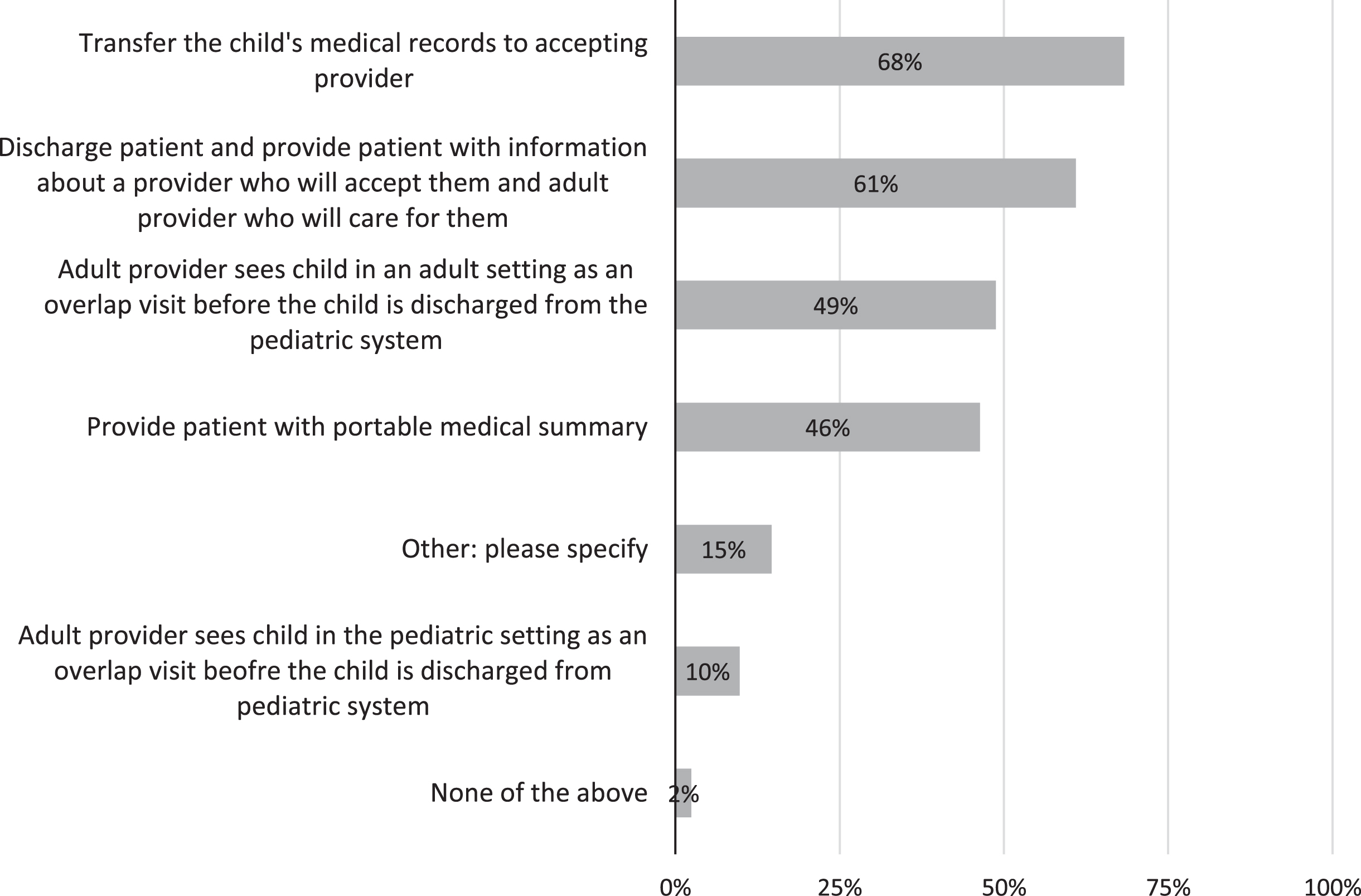
Services Provided in Transition from Pediatric to Adult Care.
The transition process from the pediatric care setting to the adult care setting was described as including the following: “transfer the child’s medical records to accepting provider” (68%of respondents), “discharge the patient and provide patient with information about a provider who will accept them and care for them” (61%), “adult provider sees child in an adult setting as an overlap visit before the child is discharged from the pediatric system” (49%), and “provide(s) patient with portable medical summary” (46%). A small number of responders indicated they did not have a transition process in place (2%).
Challenges faced when transitioning a child to adult care include finding a provider willing to accept young adults with SB when they need to leave the care of pediatric clinicians. The following comments were collected when asked about challenges: “finding an adult provider who is familiar with the population,” “adult practitioners willing to take over care,” “finding providers who are willing to accept patients,” “adult providers who are willing to work with pediatricians in that transition process,” and “finding compassionate, educated physicians in community that care for special need clients” (Fig. 3).
A total of 14%of participants indicated the use of Guidelines for Spina Bifida Health Care Services throughout the Lifespan. However, several participants indicated they were not aware of this resource (43%) while the others reported not using it (14%) or being unsure of whether they use it (29%).
Future education
Participants indicated interest in a continuing medical education activity hosted online on a central website (56%) and webinar (60%) more frequently than in-person community lectures (42%). Respondents also reported interest in both updates on the practice guidelines (56%) and handouts/materials delivered to their practice (56%).
Discussion
Updated guidelines (Guidelines for the Care of People with Spina Bifida) have been published by the SBA since this survey was conducted. These guidelines can provide immediate knowledge, direction, and guidance to PCPs [11, 12]. They include information on prenatal counseling, family functioning, transition to adult care, sexual health and function, and educational needs related to intellectual and developmental disabilities. The SBA also offers other educational opportunities and events for professionals such as a professionals’ listserv, the World Congress on Spina Bifida Research and Care, and the Spina Bifida Clinical Care Meeting.
Additionally, the SBA has implemented a Clinic Care Partner program. Clinics that receive designation as an SBA Clinic Care Partner must demonstrate that they implement best practices and can serve as resources and partner with primary care practices to share responsibilities for care [13]. A shared plan of care has been shown to improve patient and family relationships with clinicians, support provision of patient and family-centered care, and improve delivery of health care services that meet the medical and social needs of children, youth, and their families while patients are transitioning to adulthood [14].
The results of this study highlight the barriers and needs of PCPs when caring for and accepting children and adults with SB within their practice. Education on the topic of SB was identified as a critical need and desire among PCPs [2]. Over 40%of the sample were unaware of the existence of healthcare guidelines for this population despite 82%stating that they were confident in providing primary care to children with SB. Respondents reported a lack of understanding regarding several topics such as the impact of SB on sexual function and everyday life, contraception, and social support. However, low confidence in these topics did not prevent participants from identifying them as areas that PCPs should either possess full responsibility for or share the responsibility with the SB clinic. The PFCMH offers support for PCPs in providing care for children and adults with SB, transitioning patients to adult clinics, and building relationships with patients and their families when necessary.
Implementation of the PFCMH also addresses the cost of provision of care to CYSHCN. Half of Medicaid spending on hospital care for all children can be attributed to children with medical complexity, and this proportion is increasing over time [15]. An evidence-based wellness program for those with SB that utilized recommendations set forth by the PFCMH resulted in a small positive return on investment (ROI) in year 2 [16]. Scaling the program to larger numbers may result in an overall positive ROI [16].
In the present study, respondents identified the method by which they wanted to receive further educational materials which included virtual resources available through online handouts or webinars. Current resources already in the preferred virtual format include the updated guidelines from the SBA and PFCMH resources which can be found at the National Resource Center for Patient/Family-Centered Medical Home [17]. The resources available through the PFCMH include information for practices, families, and caregivers on topics such as building a medical home, resource tutorials, and care coordination. The PFCMH provides an opportunity to partner with pediatric primary care networks and organizations like the SBA to provide educational materials and guidelines on proper primary care practices for children, including those with disability. Coordinated care for CYSHCN and their families has been favorably associated with improved family-provider relations, child outcomes, and report of provider participation in shared decision making [18]. Shared decision-making allows for the engagement of youth in their care which optimizes outcomes and has excellent potential to support high-quality care [19]. The six core elements of transition consist of 3 phases: preparation, transfer, and integration into adult health care [20]. This can be customized for youth transitioning to adult care providers in the community [20]. A health care transition to adult clinics is of high importance for young adults with SB because they are a vulnerable population with high rates of behavioral health risks as well as chronic health issues [20].
Concerning observations include the inconsistencies in the transition of children with SB from pediatric to adult care and the inability of providers to find a clinician to assume the care of young adults as they age out of pediatric care. The Guidelines for the Care of People with Spina Bifida provide recommendations for transitional care [10, 11]. The dearth of providers willing to accept care of young adults remains a pervasive issue in the US healthcare system [21]. Several participants in the study indicated care was provided by the pediatric caregiver well into adulthood.
Thibadeau et al. describe various models that have been used to promote successful transition that can leverage relationships between primary care providers and SB clinics including the multidisciplinary model which has been adopted without considering processes that are necessary to provide the complex care that is needed for individuals with SB [21]. The first encounter with a physician for a child with SB is often a procedure-based physician such as a neurosurgeon. However, as one ages primary care grows in importance. These needs can be met with care in a medical home model supported by the Patient and Family Centered Medical Home Initiative, providing care coordination with patients and the local primary care providers [21]. Care coordination requires well delineated responsibilities among the PCP, SB clinics, and patients/family. This is something that has yet to be achieved among the participating health care providers in this study. Care coordination represents an area of opportunity for future education and support for the PA MHP and primary care physicians across the US to understand this population, especially given the recent updated guidelines and recommendations [10, 11].
This cross-sectional survey has some key limitations. The small sample size and representation of health care professionals from one state-wide quality improvement program may limit the generalizability of these results. Despite these limitations, this is one of the first studies to explore primary care provider knowledge and confidence in care for children with SB and its results warrant further exploration and discussion.
Conclusions
This study suggests a need for increased educational efforts, improved awareness of SB related issues, and access to evidence-based guidelines for PCPs to promote more accessible, continuous, comprehensive, patient-centered, and coordinated care across the lifespan (including the transition to adulthood) for individuals with SB. Currently, PA MHP at the PA Chapter of the American Academy of Pediatrics is utilizing several modalities to share information and help educate the network of practices across the Commonwealth of Pennsylvania. This includes but is not limited to: monthly virtual webinars with the learning community, maintenance of certification programs, Extension for Community Health Outcomes (ECHO), and learning communities to promote the integration of guidelines. In addition to year-round access to technical assistance, clinical practice guidelines, resources on transition of care, and resources on coordination of care on both the PA MHP and PFCMH website, the PA MHP offers an annual educational virtual half day conference with continuing educational units and continuing medical education credits focused on various topics. It is important for providers to understand the most recent evidence and clinical practice guidelines. In addition, access to experts from the local specialty clinic are available to address any questions or concerns when caring for the adult SB population. PA MHP is helpful in promoting up to date treatment recommendations and maintaining knowledge of those who are PA MHP practice team members.
Footnotes
Acknowledgments
This project was supported by the team housed at the PA Chapter of the American Academy of Pediatrics. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies.
Data from this manuscript was presented at the 2017 American Public Health Association Annual meeting in Atlanta, GA, USA.
Conflict of interest
Financial disclosure statements have been obtai-ned, and no conflicts of interest have been reported by the authors or by any individuals in control of the content of this article. The authors report no financial benefits.