
Abstract
PURPOSE:
The objective of this study was to analyze the effects on patient access by decreasing missed appointments after hiring a clinic coordinator using medical informatics.
METHODS:
A single-center retrospective analysis of the rates of missed appointments before and after hiring a clinic coordinator in a multidisciplinary spinal differences clinic were analyzed using a commercially available business software system (SAP® Business Objects). The total number of clinic visits was collected for each month to determine the access available for patients.
RESULTS:
The median number of missed appointments per clinic by month before employing the clinic coordinator was higher than in the two years following implementation (p < 0.0005). No differences were seen in the number of available appointment slots per month indicating no new clinics were needed to improve patient access (p = 0.551). Projected billing amounts prior to hiring the clinic coordinator indicated that $91,520 was lost in the 2 years prior to hiring this coordinator compared to $30,160 lost during the 2 years following the creation of this position (p = 0.0009).
CONCLUSION:
Hiring a clinic coordinator decreased the rate of missed appointments and was a cost-efficient intervention to improve patient access and provide effective patient care in a multidisciplinary setting.
Keywords
Introduction
Missed clinical appointments contribute to difficulties with patient care and poor health outcomes. Unused clinic slots due to missed appointments limit access for other patients. Clinics have responded to this crisis by ‘overbooking’ leading to increased wait times for patients and provider overtime [1]. Furthermore, patients who miss appointments have a higher hospitalization rate, lack preventive care, and have increased mortality [2–4]. High rates of missed appointments limit opportunities to improve patient health and decrease access to those patients desiring care. During unprecedented times, such as the global COVID-19 pandemic, reducing the need for multiple trips to a hospital for specialist visits reduces the risk of exposure. Multidisciplinary clinics benefit patients with complex health conditions. In adult medical conditions such as congestive heart failure and diabetic foot care, these multidisciplinary care models resulted in decreased readmissions, a reduction in overall hospital days, and decreased adverse outcomes [6, 7].
Spina bifida is a complex disorder which impacts physical, psychological, and social function. Multidisciplinary care models provide optimal treatment for patients with this condition [5]. Due to abnormalities in the spinal cord of patients with spina bifida, there is a higher risk for functional decline, orthopedic deformities, urological complications, and neurologic conditions [5]. A team-based approach allows families to have input from multiple specialists, including pediatric physiatrists, orthopedists, urologists, neurosurgeons, physical and occupational therapists, nutritionists, and specialized nursing care all in one visit rather than separate individual appointments. The provider specialties associated with the multidisciplinary spina bifida clinic and their roles are displayed in Table 1. Unfortunately, patients with spina bifida may travel long distances to see specialists who treat spina bifida. By grouping their appointments into one clinical visit, the burden on families decreases, including travel time, missed work, and time out of school. Despite the convenient, integrated care model of the multidisciplinary spina bifida clinic, the frequency of missed appointments remains high for this population.
Medical Specialties Available to See Patients in the Spina Bifida Clinic
Medical Specialties Available to See Patients in the Spina Bifida Clinic
Kaufman and others explored the impact on patient health and well-being after a multidisciplinary spina bifida clinic was disbanded. Access to regular medical and specialty care was significantly reduced after the closure [8]. In this study, 45–66%of patients who previously received care in this clinic were unable to receive the same level of care, even if they continued to be followed at the same location [8]. Patients with the least follow-up had an increased rate of significant complications including amputation and nephrectomy. Furthermore, neither the patient nor the primary care physician assumed ownership of the duties of scheduling necessary subspecialty providers. When care was not coordinated, outcomes suffered, even when the collaborating providers were at the same institution [8]. Multidisciplinary clinics are less common for adult patients with spina bifida, and 47%of hospital admissions in the spina bifida population were due to preventable complications such as urologic infections, renal calculi, pressure ulcers, and osteomyelitis [8]. Besides the morbidity associated with these admissions, the economic impact was also impressive. After excluding professional fees, the total costs for 166 specific preventable admissions in the spina bifida population seen at this center totaled $860,502 over the three year period from 1990 to 1992 [9]. Therefore, improved care coordination reduces preventable complications and avoids economic costs associated with these admissions in patients with spina bifida.
With traditional clinic scheduling, one missed appointment with one provider equated to one missed appointment; however, missing an appointment in a multidisciplinary clinic appointment is similar to missing 5–7 regular appointments. To reschedule each of these missed appointments with an individual provider (rather than back into a future, less accessible multidisciplinary clinic slot) the scheduler faces a variety of barriers, as each provider is on a different scheduling template and may be at different clinic locations in a given week. Most importantly, care for the patient is delayed. For families who travel great distances to attend appointments, this rescheduling may require multiple days of travel. Thus, the risk for uncoordinated care and suboptimal communication is high. Noting consistently high rates of missed appointments over the two-year period from 2009 until 2011, a clinical coordinator position was created for a multidisciplinary spina bifida clinic to improve care coordination and provide a value-added experience for patients by deliberate communication. The clinic coordinator position was implemented in March of 2011 and was filled by a registered nurse (RN) with historical knowledge of spina bifida due to her role on the inpatient wound care team. Their responsibilities were to coordinate tests for patients before their upcoming appointments, serve as a primary contact for patients entering this clinic, and act as a liaison between providers and patients for longitudinal care.
The study evaluated the effectiveness of this clinic coordinator by examining the specific impact of this position on the number of missed appointments. It was hypothesized that by hiring a specialized clinic coordinator for a multidisciplinary clinic, the rate of missed appointments would be reduced compared to the time prior to this intervention. It was anticipated that the clinic would function closer to full capacity by serving the maximum number of patients without increasing the number of appointments.
Patient appointments between March 2009 and March 2011, which was prior to the hiring of the clinic coordinator, and April 2011 and March 2013, the time period immediately following the hiring of the coordinator, were included in this retrospective cohort analysis. The clinic coordinator was hired and trained in the specific communication strategies in March of 2011. Therefore, this month was included in the pre-intervention phase for analysis. Training for this position included evaluating for transportation needs, coordinating diagnostic studies, and arranging the appropriate provider schedules to maximize the multidisciplinary clinic experience. No other programmatic changes occurred during this time period with regard to clinic structure, personnel, or clinic design.
Clinic appointment statuses were evaluated in this study. All of the patients seen had either spina bifida or another spinal abnormality requiring multidisciplinary care. This clinic was held every other week for half a day. Patients attending this clinic are of pediatric age (0–21 years), generally comprised a catchment area of approximately 3 hours from the clinic, and all of whom had a spinal difference (i.e., myelomeningocele, lipomeningocele, caudal regression syndrome, etc.). Patients were identified based on appointment scheduling type.
This study is a retrospective analysis using analytics software evaluating the impact of a specially trained clinic coordinator on missed appointments in a multidisciplinary clinic. These hypotheses were evaluated using medical informatics and de-identified data; therefore, this study did not require direct access to patient charts and received a “not human subjects” determination from the Institutional Review Board. Data from subjects were captured using a commercially available software program (SAP ® Business Objects) which can assess kept and missed appointment numbers retrospectively in a de-identified manner. Total numbers of clinic appointments per month were recorded. A clinic appointment was able to be classified as kept or missed, which was an indication of access for patients. Additionally, the average professional charges from all of the providers’ charges per clinical appointment were obtained from an analysis from the billing department. As varied numbers of professional providers saw patients during a clinic encounter, this represented the average total cost billed per patient without consideration toward the number of providers seeing each patient. This allowed for a more accurate cost-analysis per available clinic appointment slot along with the financial impact of a missed or empty appointment slot. This was factored in for a cost analysis of this clinic coordinator’s impact, to determine whether this type of position would be feasibly reproducible on a larger scale or in other clinics of similar size and complexity.
Comparison of the mean number of missed appointments per month before and after implementation of a clinic coordinator position was performed with Mann-Whitney U tests. A two-tailed α-value was set at 0.05. The number of total appointments offered between before and after the creation of this position was analyzed by using independent t-tests. Total amount saved as a result of the creation of the clinic coordinator position was represented as a cumulative summation of the difference between lost billing due to missed clinic appointments. Statistical analysis was performed using IBM® SPSS® 23.
Results
The median number of missed appointments per clinic by month before employing the clinic coordinator (median 3, range 1–14) was higher compared to the two years following implementation (0.5, 0–7, p < 0.0005). The total number of missed appointments per combined three-month period compared to the number of kept appointments is compared in Fig. 1. Additionally, there was no difference between the number of available clinic appointments during this study period (p = 0.551), indicating that new slots would not be needed to increase access.
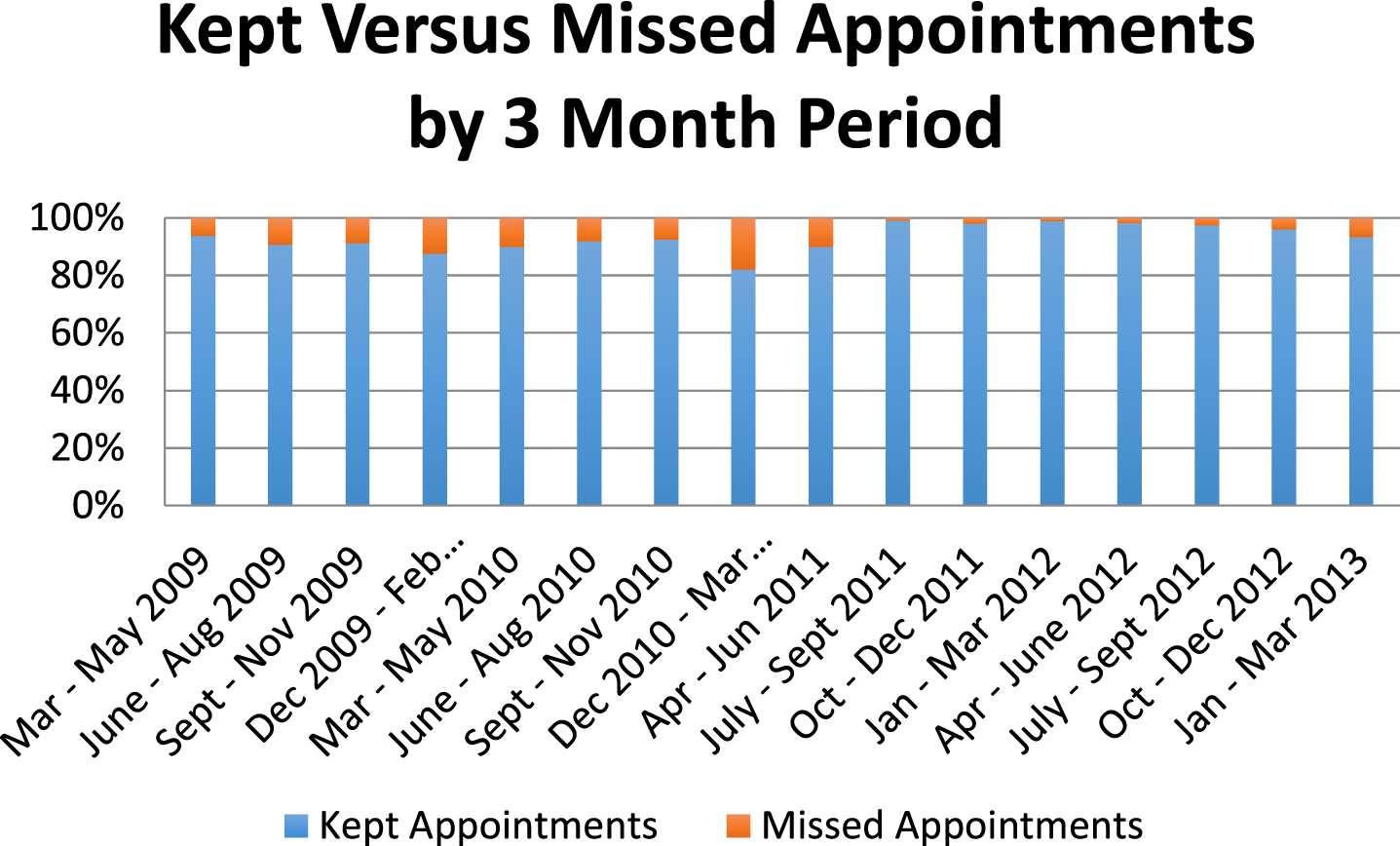
Frequency of Kept Versus Missed Appointments by 3 Month Period. This illustration demonstrates the percentage of kept versus missed appointments during the study period. The clinic coordinator position was implemented in March of 2011. By evaluating the number of missed appointments for two years after this position was implemented, long-term effects were able to be analyzed.
On average, the average amount billed per patient encounter in this clinic was $1,040, including both the professional and facility fees charged during a traditional visit in this clinic. During the period prior to hiring the clinic coordinator, a potential of $91,520 of total lost billing was identified. After the introduction of the clinic coordinator, $30,160 was lost over the next two-year period. The total hypothetical amount saved after hiring a clinic coordinator was $61,360 over a two-year period, which was statistically significant compared to the two years before implementation of this position (p = 0.0009). This does not include indirect costs from laboratory tests, radiology images performed, or subsequent referrals within the hospital system.
This study shows the positive impact of a clinic coordinator in improving patient access to the multidisciplinary spinal differences clinic by reducing missed visits during the two years following implementation of this position. The total median number of missed appointments per month decreased from 3 to 0.5 missed appointments out of approximately 35 available clinic slots per month. This statistically significant difference reflects the benefit of this key position. Additionally, this change was accomplished using the same clinic schedule without adding additional clinics. A steady, rather than variable, number of patients were seen in each clinic, optimizing flow and capacity of providers. In a traditional hospital setting where clinic space and provider availability are limited, the ideal impact of a coordinator position is to improve access without increasing systematic or personnel demands.
The role of the clinic coordinator actively targeted two key areas cited as reasons patients miss appointments: forgetting about the clinic visit and lack of knowledge or communication about the reasons for the visit [10]. By calling patients and families to verify that they were planning to come, this created a reminder and established a personal connection between the families and the clinic. By deliberately discussing the upcoming visit and identifying any specific concerns or questions, this potentially strengthened the connection and represented an investment on behalf of both parties involved. The clinic coordinator validated concerns or questions from the family, and responded with changes to the care plan to assure the patient would get the most from their visit, including arranging for diagnostic tests (such as labs, urodynamics, renal ultrasounds, or radiographs), engaging other specialists, linking with durable medical equipment providers, or contacting needed orthotists. These plans were then shared with the multidisciplinary team to ensure the needs of the patients would be met during the clinic encounter. Improved and more efficient care was delivered due to the involvement of this coordinator.
Unlike a traditional clinic model where studies are ordered at the time of the visit, the results of testing are available at the time of the visit in this model of care delivery, which moves the care plan forward with direct input from the ordering specialist and team. The patient and family receive results in a timely manner, and in the context of the multi-disciplinary team where care plans can be directly discussed and modified. This expedited method of delivering results saved physicians time, as they did not have to allot additional time to call the family. Although there were efforts to perform this type of care delivery prior to implementing a clinic coordinator position, widespread adoption of these practices was feasible only after hiring the coordinator.
Compared to interventions cited by other clinics to reduce missed appointments, such as text message reminders or online scheduling, the use of a clinic coordinator represented a more active and engaging intervention [11, 12]. Passive reminders prohibit discussion as to why an appointment might not be kept or the reason behind rescheduling one. An additional benefit of the clinic coordinator was timely identification of patients who were not planning to keep their appointment. Known open appointments can be rescheduled and filled with another patient, which improves access to patients with urgent needs or those who can come on shorter notice. Finally, access for new patients entering this type of clinic presents a challenge when a large cohort of patients with spina bifida are already scheduled and followed in this clinic with a finite number of appointment slots. By knowing which patients are pending entrance into the clinic, the clinic coordinator serves as an advocate within the hospital to assess urgency, schedule appointments appropriately, and obtain medical records for review prior to clinic visits. While multiple phone calls can be time-intensive for a clinic coordinator in a multidisciplinary model, the decreased number of missed appointments would support this increased effort by the clinic coordinator by providing improved care in a cost-effective manner.
Despite the positive findings in this study, some inherent limitations in the study design remain. Because this study was performed using de-identified data, detailed reasons for kept or missed appointments could not be ascertained on an individual patient level. However, this does not change the level of increased efficiency demonstrated by decreasing the number of missed appointments. Another significant limitation is that due to the nature of this type of research, causality cannot be implied and only associations between the rates of missed appointments can be made. Additionally, the findings were demonstrated in one type of multidisciplinary clinic. Multidisciplinary clinics with only two or three providers may not be able to demonstrate the same level of financial justification needed for this type of position; however, other types of large multispecialty clinics could benefit from a clinic coordinator to improve access and decrease missed appointment rates.
Conclusion
High rates of missed appointments significantly impact the ability of a clinic to function at the optimal capacity allowable based on personnel, time, and space. This study showed a decrease in the overall number of missed appointments for the two years after hiring a specifically trained clinic coordinator. Care coordination remains an essential part of optimizing the potential of the pediatric-aged patient with spina bifida and the families of these children [13]. This coordinator took an active approach to individual patient’s care by engaging families in discussions about their upcoming clinic visit, thereby, reduced the rate of missed appointments. Overall, this specialized clinic coordinator was shown to decrease the number of missed appointments, which allows the clinic to operate at a higher capacity without increasing the number of clinics needed.
Conflict of interest
The authors have no conflicts of interest to report.
Funding
Matthew McLaughlin, MD, MS receives funding from the National Institute of Child Health and Human Development K12HD093427.