
Abstract
Virtual reality (VR) technology has seen increasing use in physical rehabilitation and in the management of acute and chronic pain. Functional movement disorders (FMDs) are a source of disability with no known association to neurologic pathology, and patients are generally offered multidisciplinary treatment approaches to improve functional movement. However, patients who are not compliant with rehabilitation may have persistent FMD and long-term disability. Given VR’s use in physical rehabilitation, it may serve as a useful adjunct for the management of FMD. Utilizing an application called MovementTM to create a playlist of targeted applications for the restoration of motor function and balance, this case study presents the application of VR as a tool to engage patients in physical therapy for the management of FMD. The VR games were selected to encourage movement while customization of levels within the games facilitated achievement of physical therapy goals. Physical rehabilitation aided by VR, when used in collaboration with a multidisciplinary care team, may be used to facilitate recovery from FMD.
Keywords
Introduction
Functional movement disorder (FMD) is defined as abnormal, involuntary body movements that are not a result of damage to the nervous system or known neurological disease [1]. Due to a lack of irreversible neurological damage, patients with FMD have the potential to recover. Physiotherapy and cognitive behavioral therapy alone have had promising short-term results for the management of FMD [2, 3]. However, even with psychosocial support, the majority of patients with FMD remain symptomatic for protracted periods of time, with varying levels of physical and psychological comorbidity [4]. Pediatric FMD is particularly challenging to treat, but early diagnosis and treatment may facilitate recovery [5–7]. Because FMD may lead to maladaptive integration of physical and psychosocial functions, a multidisciplinary team approach has been suggested [8, 9].
Virtual reality (VR) is a relatively new tool in the field of physical rehabilitation offering several advantages. First, applications or games can be customized by the therapist to mimic movements done in traditional physical therapy (PT) and meet PT goals set forth by the patient care team. Second, virtual environments may be personalized to create an immersive experience. This elicits a feeling of being physically ‘present’ and allows the user to react in a realistic way. Third, VR can incentivize movement by using applications and environments that the patients find engaging. Through incentivized goals and gameplay that mirrors normal movement, it is possible to increase repetition, training duration, and patient treatment compliance to relearn normal movement patterns [10, 11].
Physical rehabilitation with virtual reality (PRVR) has been used as an adjunct for motor conditioning [12–14]. When used in conjunction with standard rehabilitation, VR improved upper and lower extremity mobility in stroke patients [15, 16]. Patients with neurological diseases, such as Parkinson’s disease, multiple sclerosis, and cerebral palsy, experienced improvements to gait and balance with VR [17]. Pediatric patients with similar neurologic diseases and acquired brain injuries have also demonstrated improvements in gait and balance when PT was combined with VR [18, 19].
PRVR has emerged as a promising approach to facilitating therapeutic gains in chronic pain rehabilitation and improvement of FMD symptom frequency in the adult population through mirrored visual feedback [20–22]. This case presents the use of VR paired with the custom MovementTM application as an additional tool that therapists can utilize to personalize PT for the management of FMD in a pediatric patient.
Patient information
This case report was Institutional Review Board exempt, and consent was sought from the caregiver. A 15-year-old girl weighing 41 kg (BMI 16.21) with a history of autoimmune polyglandular syndrome (type I diabetes mellitus, Addison’s disease, hypoparathyroidism) and psychogenic non-epileptiform seizures (PNESs) presented for complex glucose management. Psychiatric diagnoses included an unspecified eating disorder, an unspecified mood disorder, and anxiety. Social history included being raised by a single mother. During her 78-day hospital stay, which was complicated by hyperglycemia, she deconditioned to the point of being unable to stand independently for longer than five minutes without reporting extreme fatigue and weakness. At the beginning of her hospital course, a wheelchair was recommended by adolescent medicine to conserve energy given the dietary restrictions that led to her recent weight loss. However, once caloric intake improved, the patient was encouraged to ambulate and received inpatient PT to preserve functional–mobility and strength.
Clinical findings
Neurology was consulted to evaluate for seizure vs PNES activity. Electroencephalography monitoring revealed no abnormalities, and a complete neurological exam was unremarkable: reduced muscle bulk consistent with recent weight loss, tone of 0 (normal) on the Ashworth Scale, 5/5 strength throughout, no sensory deficits, and 2+ (normal) deep tendon reflexes in all extremities. On hospital day 34 (week 5), the patient initially displayed a smooth and coordinated gait with no evidence of dysmetria or truncal titubation. When asked to walk during sequential exams and PT in the following week, the patient displayed difficulty standing, dystonia, jerking movements and lateral loss of balance. Traditional PT was complicated by patient participation as she exhibited astasia-abasia in the presence of providers during hospital weeks 6–8. Re-evaluation by neurology revealed no abnormalities from the prior neurologic exam except the newly displayed abnormal gait. The astasia-abasia gait in the context of her otherwise normal neurological exam and EEG was consistent with FMD. PRVR was suggested by the PT team as a tool to assist with patient participation toward achieving PT goals.
Therapeutic interventions
In order to facilitate patient participation and progression towards PT goals, two PRVR sessions were scheduled one week apart while glucose management was being optimized starting on hospital week 9. The first session was scheduled for 15 minutes and assessed the patient’s physical tolerance and game preference prior to planning gameplay time for future sessions. PT goals included increasing overall movement compared to baseline alongside balance, improving coordination, and weight transfer training. A portable VR station may be brought into a patient’s room (Fig. 1) or, as in this case, an open space in an inpatient hospital PT gym [23]. The patient was fitted with a customized, infection control compliant VIVE headset, two hand controllers, and motion trackers (HTC Corporation, Taiwan) on each extremity. This was paired with the Movement application developed by CHARIOT (chariot.stanford.edu) to create a playlist of immersive games specific to the patient’s PT goals while tracking the total movement of each extremity. A physical therapist was present at all times to guide therapy and act as a spotter to prevent falls or deviation away from the designated play area.

Example set-up of HTC VIVE virtual reality equipment in a patient room. (Left) An additional monitor can be connected to display what the player sees. People in the room (e.g., family and the patient care team) can watch the display and coach the player. (Right) Display of player in Fruity Feet looking at fruit on the ground while a staff member adjusts gameplay settings.
Each session consisted of three applications: Fruity Feet (Invincikids, Palo Alto, CA), Beat Saber (Beat Games), and Tilt Brush (Google). In Fruity Feet, the player grabs fruit above their head, facilitating upper extremity movement, or stomps fruit on the ground, which correlates to marching in place, a standardized PT tool to strengthen lower extremity muscles (Fig. 2B) [12]. Beat Saber, a VR rhythm game, facilitates arm exercises by selectively positioning directional boxes (boxes with arrows) for the player to slash in a specified direction. It also incorporates obstacles that must be dodged to train balance, coordination, and weight transfer by facilitating full-body movement to the left, right, or squatting position (Fig. 2A). Lastly, Tilt Brush was used as a cooldown period (Fig. 2C). A more thorough summary of each game is provided in Table 1.
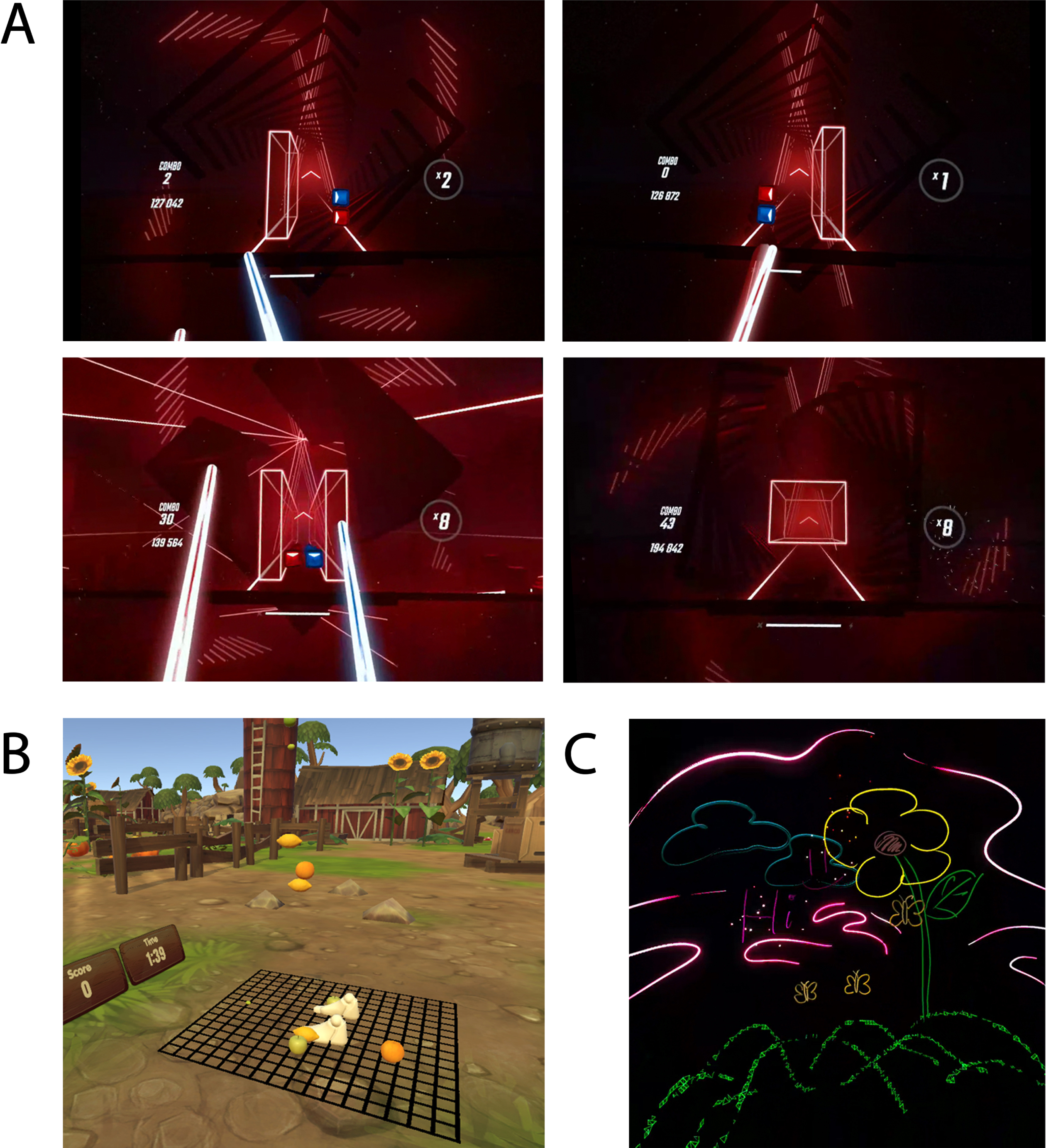
(A) Screenshots taken from Beat Saber gameplay. In clockwise orientation, the player must step right, left, squat down, or maintain midline position to avoid obstacles and hit the colored boxes in a specified direction. (B) Screenshot taken from Fruity Feet. The player’s virtual feet can be seen directly above the black grid as lemons and oranges appear around the player. (C) Screenshot taken from Tilt Brush. A drawing made in 3D space by the patient in this case.
Gameplay description of each game and targeted physical therapy goals
Qualitative and observational notes for each PRVR session are summarized in Table 2. The patient arrived at Session 1 in a wheelchair assisted by the physical therapist. When asked to walk, she displayed astasia-abasia. Upon wearing the VIVE headset, the patient expressed a sense of immersion as she explored the Fruity Feet farm-like environment and crushed fruit with both hands and feet. The physical therapist coached the patient to crush fruit with a particular hand or foot if it was idle as displayed in real time in the Movement application (Fig. 3A). Within Beat Saber, the patient danced and slashed to the beat of the music, demonstrating appropriate upper extremity range of motion and balance. The PRVR session ended with Tilt Brush during which she painted pictures and words. After the 15-minute VR session, the patient was able to walk independently back to her room without wheelchair assistance.
Summary of qualitative findings and notes before, during, and after each physical rehabilitation with virtual reality (PRVR) session
Summary of qualitative findings and notes before, during, and after each physical rehabilitation with virtual reality (PRVR) session
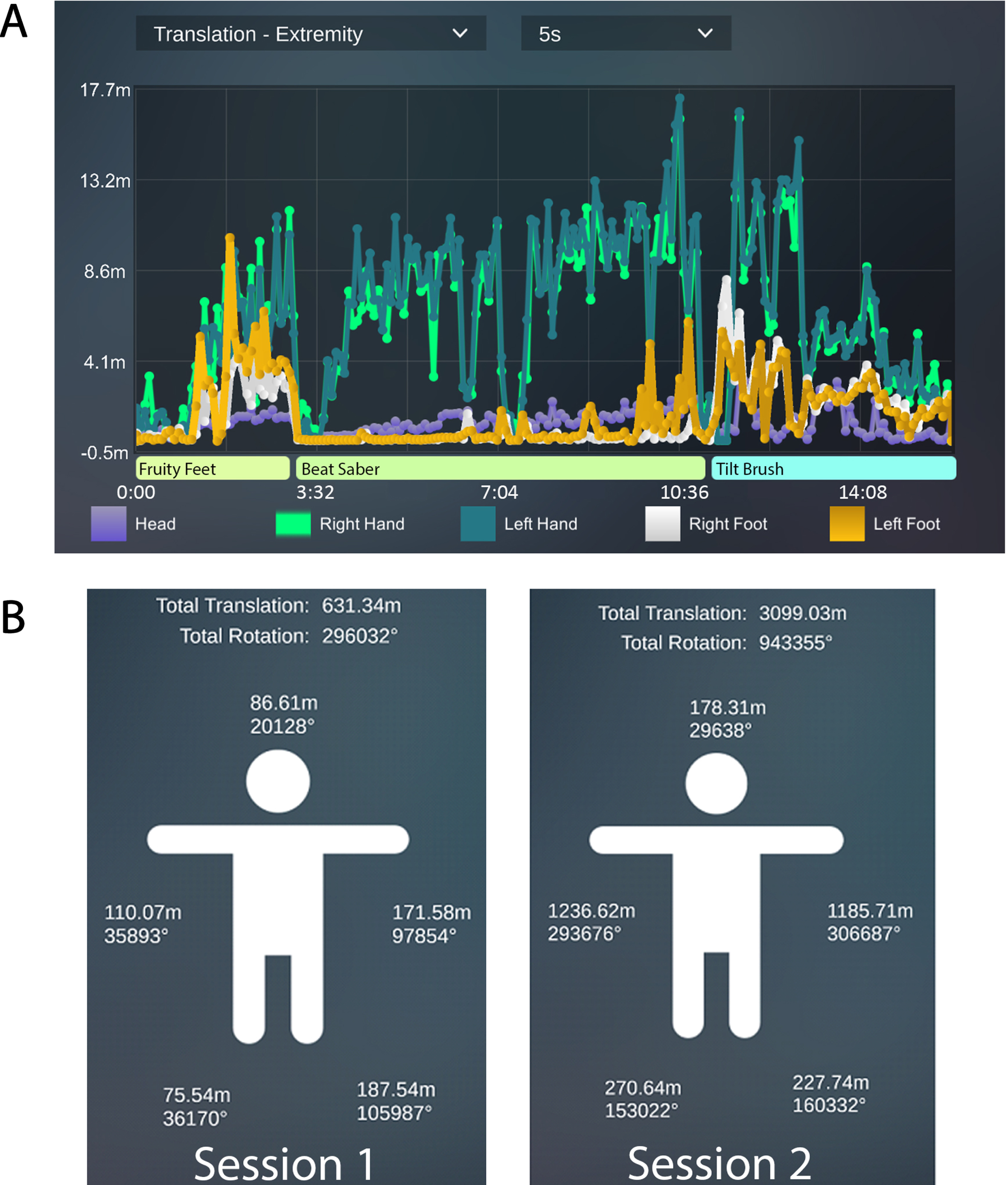
(A) Translational movement recorded through MovementTM in real time. If an extremity does not move, such as during loading screens, the tracings return to baseline. A staff member can see if an extremity has not moved over time and coach the patient to engage the extremity. (B) Summarized total translational movement for each extremity for Session 1 and 2.
The patient arrived to PRVR Session 2 without a wheelchair or walking assistance. She participated in a 30-minute VR session with a 5-minute break halfway through. The same playlist of games from session one was used, now with an increased intensity of gameplay. In Fruity Feet, the number and density of fruit were increased. In Beat Saber, the number of directional boxes was increased. The patient and her parent expressed high satisfaction with the use of VR and selected games for PT.∥The total translational extremity movement was summarized after each session (Fig. 3B). A 5-fold increase in total movement from PRVR Session 1 to 2 (Table 3). There was a nearly 10-fold increase in each upper extremity as the intensity of Fruity Feet was increased, and the patient spent the majority of her time in the Beat Saber application, which focuses on upper extremity movement. Before the Session 3 the patient’s insulin regimen was optimized and she was discharged home with her parent.
Breakdown of total time spent and total movement recorded in each physical rehabilitation with virtual reality session
Recommendations for the assessment and diagnosis of FMD are readily available; however, there is no clear consensus regarding the most effective treatment option [1, 24]. The current standard of care consists of a multidisciplinary approach combining physical rehabilitation, counseling, and social support. However, challenges arise when patients, particularly pediatric patients, are unable to or do not want to engage in PT. In this case, the patient displayed an astasia-abasia gait in the presence of providers which limited her ability to perform movements during PT.
This case demonstrated the use of VR for sensorimotor relearning for posture and balance using customized applications for a pediatric patient with FMD. VR has historically been used for non-pharmacologic management of acute and chronic pain through distraction rather than functional gain through targeted physical movement [25, 26]. In recent years, VR applications that target rehabilitation have emerged. VR can serve as a PT tool to encourage participation during therapy by choosing games that match patient preferences. Pilot and case studies have reported that patients were motivated to participate and continue exercising due to the enjoyment of the VR games and turning rehabilitation tasks into a game [20, 27]. Moreover, VR may help retrain movement through diverting attention away from the affected limb with conversion in order to generate meaningful movement. At a cognitive level, distraction may take place through music and visuals. Physically, movement can be incentivized through the natural gameplay of each game and earning points. The gameplay may distract the patient from cognitively controlling their movement while stimulating automatic movements that mirror normal movements of a particular activity (e.g., arm extension or stepping forward).
The Movement application allows the physical therapist to create a playlist of games tailored specifically to a patient’s rehabilitation goals. Additionally, the applications can be customized to focus on upper or lower extremity movements or right-left dominance. The Movement application also allows for the collection of aggregate movement data, which can be used to set goals for future sessions. However, it is important to note that the Movement application does not quantify measures of balance and coordination, and it does not quantify movement where gameplay requires the player to stand in place. Although a patient may be working towards achieving PT goals in VR, the end result may not be reflected in quantifiable measures, but it can be qualitatively assessed. This is better understood by breaking down gameplay for each game chosen for this patient case.
Targeting balance and weight transfer was an important component to managing this patient’s astasia-abasia gait. Within Fruity Feet, the player must move an extremity to reach fruit appearing around them in order to earn points. Because the fruit travels vertically or horizontally around the player and not in a single plane, the player must practice coordination and balance to reach a target fruit. Fruit that appears above or below the waist is hit by the respective upper or lower extremity, and the total translational movement recorded is reflected in the Movement application. Beat Saber gameplay consists of hitting directional blocks with the arms to earn points while avoiding obstacles by either stepping to the side or squatting. Because gameplay focuses primarily on arm movement, total translational movement recorded in the upper extremities is expected to be higher than the lower extremities. Movement recordings of the lower extremity primarily come from the player stepping approximately one foot from side to side to avoid obstacles with the addition of a small number of recordings from realignment to midline and adjustment of the feet to maintain balance. Because the patient enjoyed playing Beat Saber, the majority of each session was spent playing it. However, each level was customized to include more obstacles for the player to avoid while matching the rhythm of the music to work on balance and weight transfer. The adaptation of gameplay helped maintain patient participation while meeting PT goals. Tilt Brush was chosen as a cooldown and did not focus on a PT goal. Although patients with FMD are generally offered a multidisciplinary approach, this patient displayed the ability to walk independently without an abnormal gait after the first PRVR session and no additional services were prescribed.
The main limitation to current VR technology is its inability to simulate all movements of a standard PT session. Although total aggregate movement was increased, different applications were needed in order to target movement in a specified direction. Another limitation is the complete immersion of the player. Without seeing their surroundings, the player is at risk of falling, thus requiring close provider supervision and a safe space for VR use. Although it did not occur in this case, movement within the virtual environment can lead to motion sickness. Providers should stand near the patient to prevent collision into obstacles and stop gameplay if motion sickness is experienced.
This case demonstrates that PRVR can be a useful adjunct for motivating movement and engagement of a pediatric patient in PT by customizing games that align with the patient’s preferences. Although the use of PRVR to incentivize movement through gameplay was effective for this patient, it may not be suitable for all, particularly those who have a history of motion sickness or seizure disorders. Future studies applying PRVR as used in this case with more pediatric patients and within the adult population for treatment of FMD may elucidate if VR can reduce patients’ symptoms in the long term. Collaborative care plans coordinated by medical providers, physical therapists, and occupational therapists, along with patient involvement and buy-in, remain vital to optimizing the clinical application of this technology.
Footnotes
Acknowledgments
None.
Conflict of interest
The authors have no conflict of interest to report.