
Abstract
PURPOSE:
Early mobility (EM) and patient communication have known benefits for critically ill patients, but perceived barriers exist, notably related to family and caregiver concerns. Caregiver perceptions of an EM and communication therapy protocol in the pediatric intensive care unit (PICU) were assessed.
METHODS:
Caregivers of PICU patients at a free-standing academic children’s hospital completed a survey using a Likert-type agreement scale on their perceptions surrounding the safety of EM, benefits of EM and communication, and barriers to EM and communication services.
RESULTS:
Forty caregivers completed the survey. Most agreed or strongly agreed that EM helped their child get stronger (76%), improved their child’s mood (57%), helped them to be involved in their child’s care (86%), and improved their child’s overall experience (78%). Most disagreed with statements relating to EM causing fear or pain (57%). Caregivers agreed that communication therapy improved overall ICU experience (75%). Free-text comments emphasized meaningful relationships with rehabilitation and unit staff.
CONCLUSION:
Caregivers perceived EM and communication interventions as enriching to their child’s ICU experience and the majority did not perceive that EM caused fear or pain.
Introduction
Children who survive critical illness have long-term detrimental sequelae such as delayed recovery, residual perceptual-motor, psychiatric, and behavioral problems along with reduced quality of life [1, 2]. As mortality rates continue to decline in critically ill children [3], the focus is shifting towards preventing these long-term negative effects [2]. The ICU Liberation initiative was formed to ameliorate the negative consequences of an ICU stay using an evidence-based care bundle, also referred to as the A-F bundle, including “E” for early mobility and “F” for family-centered care, focusing on communication with patients and families [4].
Early mobility (EM) is a term used to describe physical activity early on in critical illness [5, 6]. Adult studies have shown several benefits to EM including decreases in hospital and ICU length of stay, ICU acquired weakness, delirium, and sedation needs [7–9]. The benefits of EM in the pediatric population are slowly emerging [10–13], and several studies have shown EM is attainable in the pediatric intensive care unit (PICU) [14–18]. Although studies have favored EM to be safe and feasible in the PICU population [14, 19], several challenges have been reported in the literature including limited resources, safety concerns, and patient instability [14, 20]. There are few studies assessing family perceptions surrounding pediatric EM and communication services in the ICU setting. Zheng et al. interviewed caregivers, patients, and clinicians after an in-bed cycling pilot study and found that all reported similar barriers to EM, including the low prioritization of mobilization, safety concerns, lack of physiotherapy resources, and low patient motivation [21]. Colwell et al. surveyed parents for stress surrounding EM and found that parents identified subjective pain, fragility concerns, movement of medical equipment, and perceived dyspnea as sources of stress [22]. Adult studies have found family members may fear that mobilizing their loved ones may cause pain or impede nursing care [23]. Involving families in EM can increase compliance and help them feel they were part of their loved one’s recovery [23].
Communication or speech therapy services focused on patient and family engagement may also be provided in conjunction with traditional EM activities. Critically ill individuals often have reduced communication skills that may be related to baseline deficits (such as cerebral palsy with associated dysarthria), directly tied to critical illness (such as traumatic brain injury with resulting neurocognitive impairment), or iatrogenic in nature (such as inability to talk due to endotracheal tube). Poor communication skills may limit a patient’s ability to participate in care such as EM [24], decrease patient safety [24, 25], reduce patient coping skills [26], and contribute to feelings of helplessness [27]. Communication therapy services in the ICU frequently involve Augmentative and Alternative Communication (AAC) supports such as picture boards, communication buttons, or text-to-speech communication applications. AAC supports in the adult ICU have been linked to decreased patient frustration [27, 28] as well as enhanced vent weaning and increased patient engagement [28, 29]. Costello and colleagues at Boston Children’s Hospital have implemented AAC for critically ill children and have reported through case studies on its efficacy in terms of medical outcomes as well as patient and parental satisfaction [24, 30]. There is limited literature describing family perception of communication services in the PICU.
After institution of an EM and communication protocol, caregiver perceptions surrounding protocol interventions were studied, and changes in perceptions after observation or participation in their child’s EM and communication activities were assessed.
Methods
Setting
The study took place at a free-standing academic tertiary care children’s hospital. Institutional IRB approval was granted for this study. Prior to the study, an EM and communication protocol was implemented as part of a quality initiative in both hospital PICUs (a 30-bed medical-surgical ICU and the 24-bed cardiac ICU). Per the protocol, EM orders are placed at 72 hours PICU length of stay, and patients older than 12 months received a communication consult at the same time. EM activities were defined based on patient age/developmental level and severity of illness (Appendix I). Communication interventions and activities were also directly related to patient age/developmental level and severity of illness with focus on cognitive-linguistic stimulation and patient-family-provider communication. Direct speech therapy services were provided as were specialized AAC supports such as picture communication boards, communication buttons, and text-to-speech applications. When available during sessions, EM and communication therapists attempted to engage family members as much as possible.
Survey
A literature review was performed to assess the common barriers and benefits of EM in the adult and pediatric population. The following themes emerged from the review: perceived weakness of the patient, safety of EM, pain during the EM session, fear about moving the patient, mood of the patient, how therapy affected the patient’s autonomy/independence, how EM affected caregiver’s perception of their involvement in their child’s care, and how EM affected their overall experience. Based on these themes, an electronic survey was created. It was conducted in a single setting but consisted of three sections addressing the caregivers’ concerns and feelings prior to an EM session, during an EM session, and after an EM session. Caregivers of older children also had the opportunity to provide feedback on communication therapy in a fourth section. They rated statements using a Likert-type agreement scale and were permitted to provide free-text comments. The survey questions were validated by a family advisory committee for content and clarity prior to use. Inclusion criteria were a caregiver’s child participating in at least one EM session, caregiver familiarity with EM session (present for EM or familiar with EM process), caregiver age of 18 years or older and English speaking. A member of the research team, not involved in clinical care of the patient, approached caregivers for consent. Each survey was completed once by each participant. Study data were collected and managed using REDCap electronic data capture tools hosted at Vanderbilt University. REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies (projectredcap.org).
Statistical analysis
Survey answers were assessed for agreement, neutral, or disagreement. For each question, choices of strongly agree and agree were combined into one category of agree, and disagree and strongly disagree were combined into one category of disagree. Age analysis was completed using Microsoft Excel (2008). Free text responses were reviewed by study team for common themes.
Results
A total of 42 participants consented. However, two were unfamiliar with EM and thus did not complete the survey, resulting in a final total of 40 completed surveys. Twelve of the 40 had a child old enough to participate in the communication protocol and observed it. Caregivers reported a wide range of their child’s age (Table 1) with a median age of three years. Fifteen (37.5 %) reported their child’s age as less than 12 months, and as such were unable to participate in the communication protocol portion.
Age of caregiver’s child and number of caregiver-witnessed early mobility sessions
Age of caregiver’s child and number of caregiver-witnessed early mobility sessions
aEM = early mobility.
On review of the pre-EM questions of the survey (Fig. 1), over half of participants agreed their child had become weak during their ICU stay (55%). Caregivers reported that prior to the first EM session they had concerns that EM was unsafe (21%), would cause pain (31%), and that their child would be afraid to move or do activities (21%).
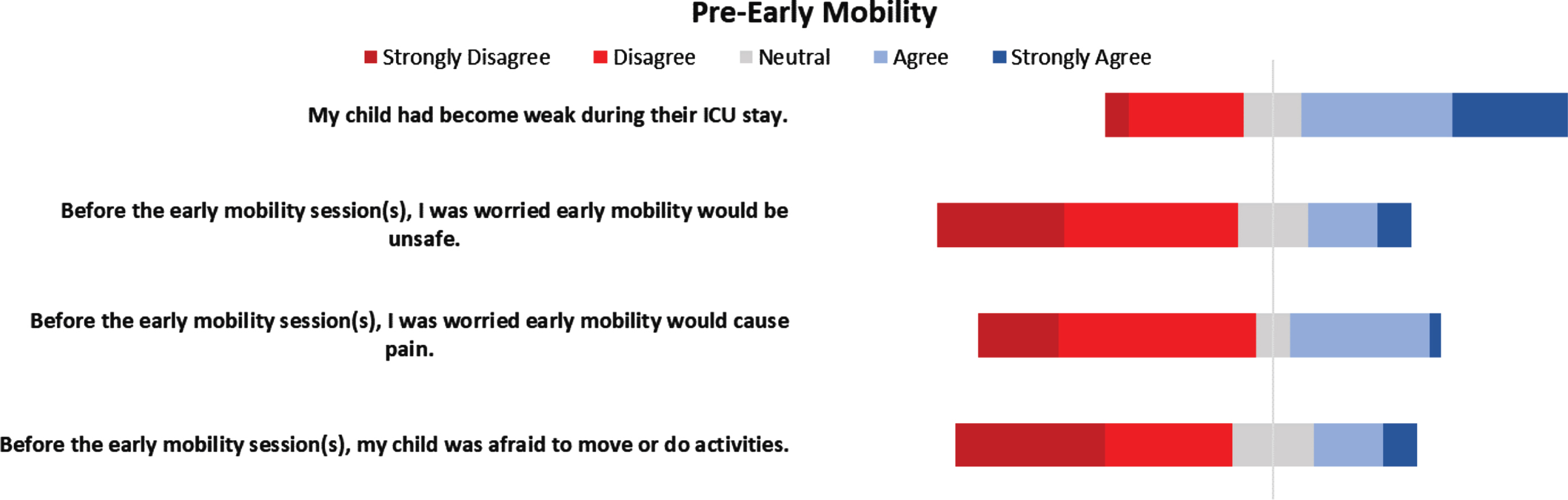
Caregiver perceptions of early mobility prior to early mobility sessions.
Survey questions concerning during-EM (Fig. 2) and post-EM (Fig. 3) perceptions showed that despite initial concerns, a majority of caregivers agreed that their child enjoyed early mobility (60%), disagreed that their child experienced pain during the sessions (52%), and disagreed that their child was scared (64%). Caregivers agreed that EM helped their child get stronger (76%), improved their child’s mood (57%), motivated older children to participate in their own care (53%), helped the caregiver to be involved in their child’s care (86%), and improved their child’s overall experience while in the ICU (78%).
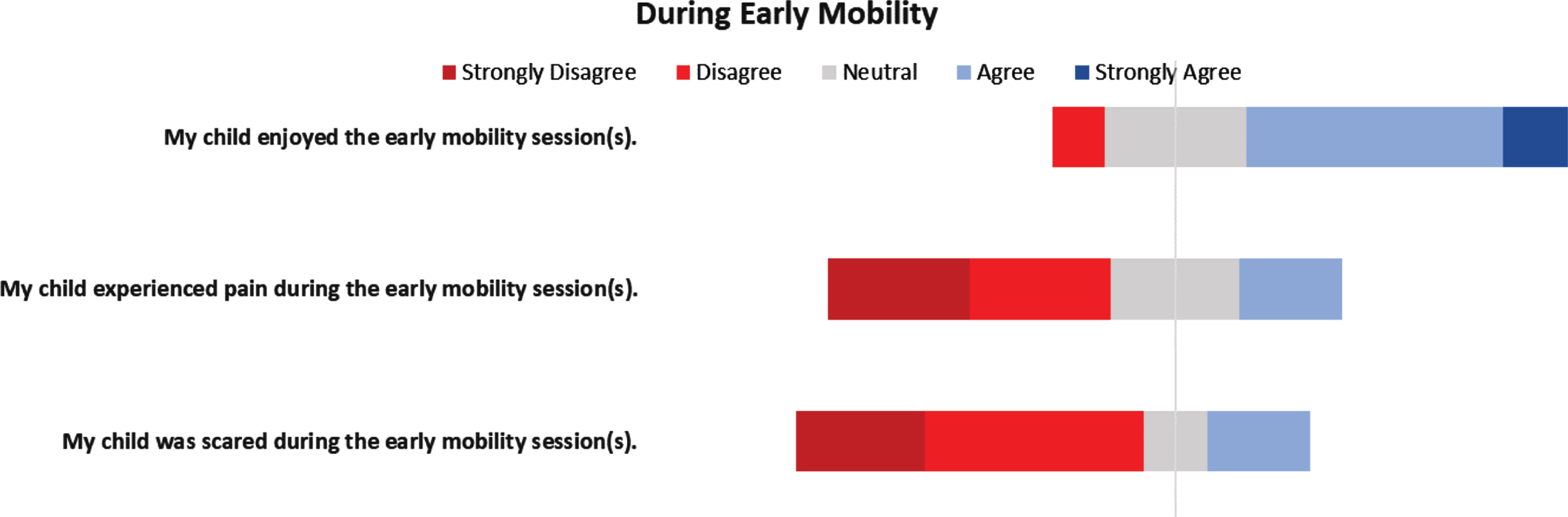
Caregiver perceptions of early mobility during sessions.
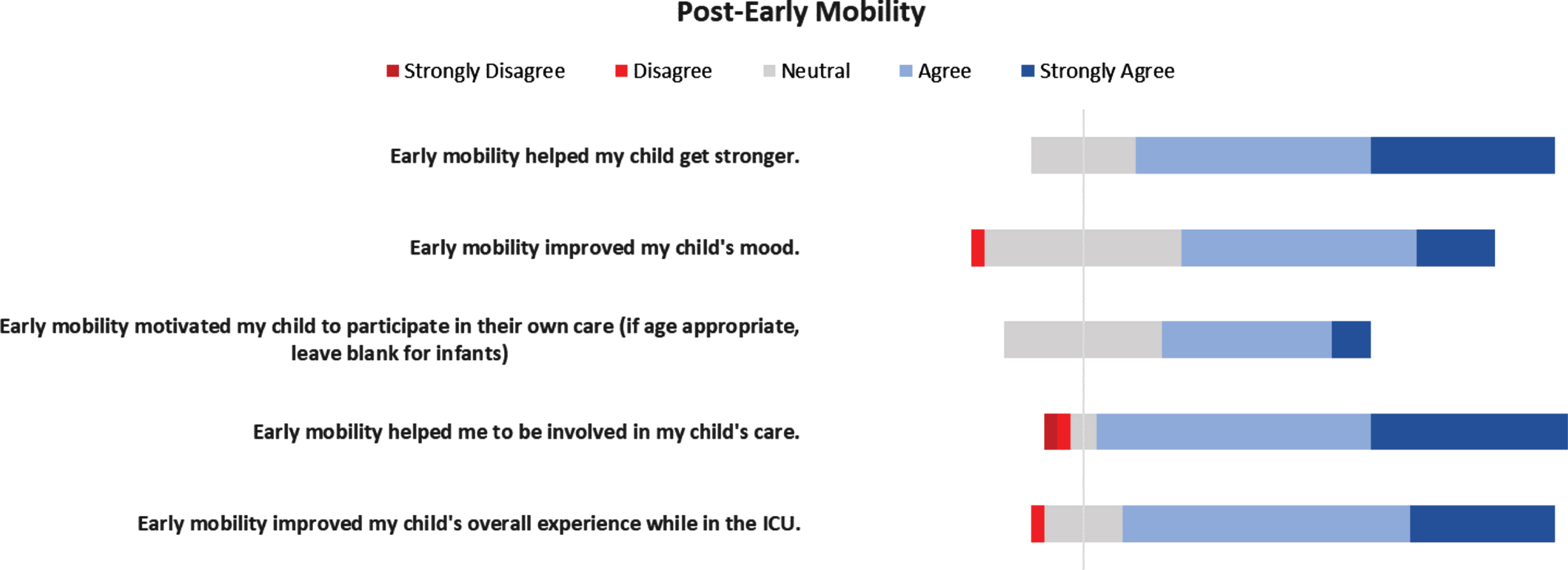
Caregiver perceptions of early mobility after sessions.
Survey questions surrounding communication (Fig. 4) revealed caregivers agreed that the protocol and communication interventions helped their child communicate better with them and/or other people (58%), get better (58%), have more dignity (50%), and improved their overall experience in the ICU (75%).
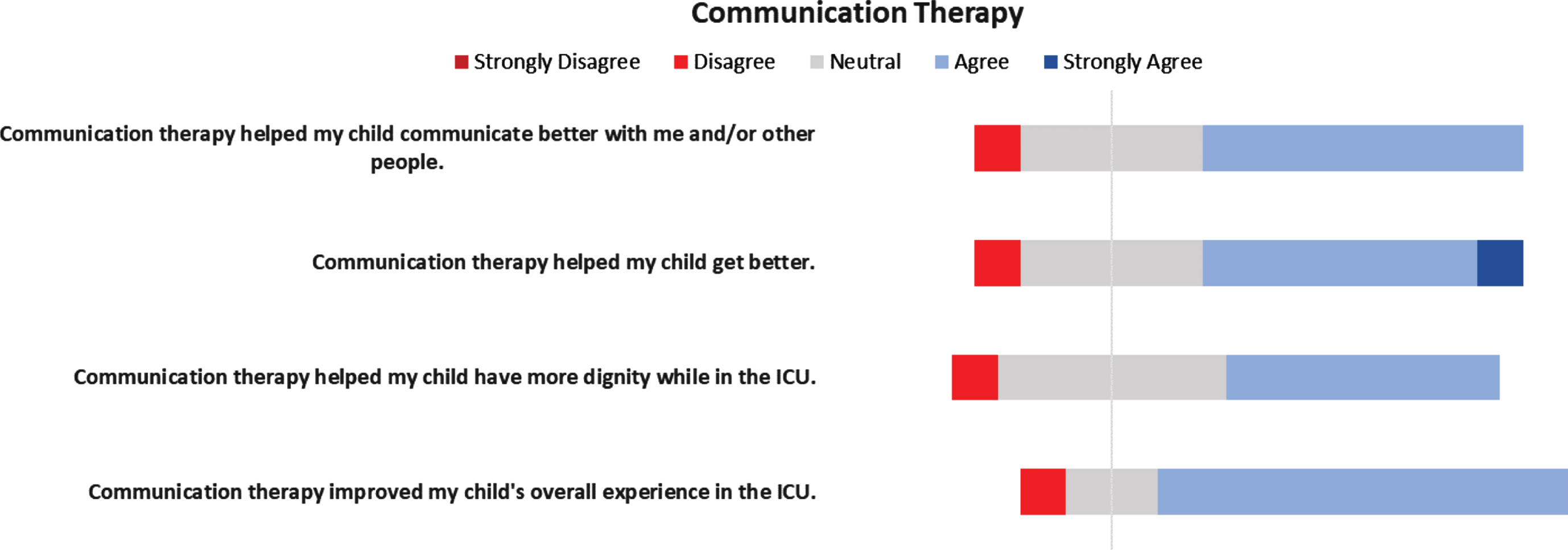
Caregiver perceptions of communication protocol/therapy.
Free-text survey comments were overwhelmingly positive. Participants felt therapists valued caregiver input. They appreciated that therapy was included early in the care of their child and that the care team was forward-thinking in their child’s recovery. Finally, caregivers felt that the positive attitudes and the encouragement from the therapists were key components for their child’s recovery. Some examples of these comments are as follows, “The staff is great. The therapists are very helpful and instructive. Their positive attitudes and encouragement have been wonderful too”, “It meant so much to know that people involved in his care were thinking ahead...”, and “I feel that having the early mobility therapy helped my son progress extremely”.
Despite the potential valuable benefits and low risk, PICUs continue to have difficulty providing EM for critically ill children. Many barriers exist to EM, including patient-related issues, perceived safety concerns, lack of equipment, lack of personnel, and caregiver concerns [20, 21]. It has been noted in multiple studies that one key factor to the success of EM is involvement of family members [21, 23]. In this study, caregiver perceptions of EM and communication interventions in the PICU were further evaluated.
About 30% of caregivers were concerned EM would be painful to their child prior to the initiation of EM, but after experiencing EM only 19% felt their child actually experienced pain during the sessions. In the future, it may be beneficial to have a pain management plan with the bedside nurse prior to EM sessions to alleviate caregiver concerns. Most caregivers agreed their child had become weak during their ICU stay, but a small portion did fear EM would be unsafe prior to the sessions. However, the majority of surveyed caregivers felt their child enjoyed early mobility and that it had positive effects on their recovery. These findings would correlate with Colwell et al.’s study showing ∼80% parents did not find EM stressful, and many felt it was helpful for their child’s recovery [22]. These results suggest caregiver observation and/or participation in EM may alleviate concerns and have a positive impact on caregiver perceptions.
Furthermore, very little literature exists surrounding caregiver perceptions of communication therapy in the PICU. While previous studies have shown that communication between providers and the families has eased multiple stressors throughout the ICU stay [29, 30], limited data exists surrounding the benefit of pediatric patient communication in the ICU. The majority of caregivers agreed that this protocol helped their child: communicate better with them and/or other people, get better, have more dignity, and improve their overall experience in the ICU.
Although caregiver concern may be a perceived barrier to EM in the PICU population, the findings would suggest otherwise. Previous literature has shown that family participation in EM is beneficial for recovery of the patient [21, 23], and that caregivers believe they have a different supportive role that clinicians cannot provide [23]. Caregiver engagement may foster success when instituting EM and communication protocols in pediatric patients. The ICU Liberation bundle emphasizes family engagement, including family presence on ICU rounds, decision-making, and treatment planning that has been proven to be beneficial [4, 31]. EM also allows caregivers an opportunity to directly assist caring for their child during critical illness. The findings support this, as the majority of survey participants agreed that the EM and communication protocol helped them to be involved in their child’s care and improved communication with their child during the period of critical illness. Data is emerging that caregivers and family members of the critically ill can suffer psychological harm, including post-traumatic stress disorder, depression, and anxiety [32]. Many caregivers may experience feelings of helplessness during their child’s ICU stay, which may be partially due to their inability to care for or communicate with their child. Further research is needed to assess whether caregiver participation in EM and communication protocols may alleviate some of the psychological stressors of having a child or loved one in the PICU.
This study had several limitations. It occurred in a single center with a center-specific protocol. The survey was completed after a child had received EM, and thus was subject to recall bias when asking caregivers about their perceptions pre-EM. The surveys were also administered at different points throughout the child’s hospitalization and recovery. If a patient had already transferred out of the ICU during the survey, a caregiver may have a more favorable opinion of the EM and communication protocol. Lastly, the survey was completed on only a small portion of the patients.
Conclusions
Caregivers perceive EM and communication interventions as enriching to their child’s ICU experience. Future research may consider correlation of caregiver involvement with patient outcomes and caregiver mental health and stress level.
Footnotes
Acknowledgments
The authors would like to thank the Monroe Carrell Jr. Children’s Hospital at Vanderbilt Rehabilitation team and SLP team for all their dedication to providing the highest quality patient care.
Conflict of interest
The authors have no conflicts of interest or funding to report.