
Abstract
Sjögren-Larsson syndrome (SLS) is a rare neurocutaneous disorder characterized by the presence of congenital ichthyosis, spasticity, and mental retardation. As with other rare genetic diseases, treatment is mainly symptomatic. Due to the absence of definitive treatment, lifelong follow-up and support of patients are important to improve the quality of life. A 7-year-old female child who was diagnosed as having SLS was referred to the rehabilitation clinic. After 20 sessions of a rehabilitation program, she started walking independently with the additional contribution of ankle-foot orthoses (AFOs). The contribution of the short-term rehabilitation approach and especially the administration of AFOs to the independence level of the patient is emphasized herein.
Background
Sjögren-Larsson syndrome (SLS) is a rare neurocutaneous disorder characterized by the presence of congenital ichthyosis, spasticity, and mental retardation [1]. As an autosomal recessive inherited disorder, SLS is a type of leukodystrophy, which is caused by mutations in the ALDH3A2 gene for fatty aldehyde dehydrogenase (FALDH).
SLS was first described in 1957 by Swedish physicians, Sjögren and Larsson. They reported a group of 28 interrelated patients from Sweden, who had symptoms of what is now thought of as the clinical triad, or diagnostic signs, of SLS: intellectual disability, spastic diplegia, and congenital ichthyosis [2]. Although several genotypic and phenotypic variations have been reported [3–5], the signs and symptoms of SLS typically occur within the first two years of life. Cutaneous manifestations such as ichthyosis and erythematous rash are the first signs that bring the patient for medical attention [6]. Beyond the classic presentation of the disease, patients can develop many symptoms such as speech difficulties, seizures, preterm birth, glistening white dots in the retina of the eye, and kyphoscoliosis [6–8].
Neurologic manifestations are one of the leading presentations. Developmental delay is noticed in early infancy. Spasticity may be apparent before the age of 3 years and is more prominent in the lower limbs than in other parts of the body. The majority of patients with SLS require a wheelchair for mobility over time and also develop contractures [1, 5]. Detailed evaluation of neuromuscular findings has great importance in both establishing the correct diagnosis among a differential which includes diseases such as cerebral palsy (CP) as well as in guiding the rehabilitation approach.
One of the important involvements is ocular manifestations because the main pathologic mechanism of the disease is FALDH deficiency and associated long-chain fatty alcohol and aldehyde accumulation [9]. The main features are perifoveal crystalline inclusions (glistening white dots), cystoid foveal atrophy, and lack of macular pigment [9–11]. High refractive errors and photophobia may be present [9, 12]. There are also cases in the literature without ocular involvement [12, 13].
As with other rare genetic diseases, treatment is mainly symptomatic [14]. Due to the absence of definitive treatment, lifelong follow-up and support of patients are important to improve the quality of life. In this case presentation, the results of a short-term rehabilitation approach and use of ankle-foot orthoses (AFOs) in a patient with SLS are emphasized.
Case presentation
A 7-year-old female born to consanguineous parents and diagnosed with SLS was referred to the clinic for rehabilitation. She was born full-term, appropriate for gestational age, by normal vaginal delivery. Her parents claimed that the prenatal period and delivery had been uneventful. It was learned from her medical records that erythematous dry scaly skin areas localized to the abdomen and four extremities were determined on physical examination immediately after birth. A microscopic examination of skin biopsy material was reported as compatible with ichthyosis. Topical treatment with moisturizing creams and keratolytic agents had been administered for 5 years and the skin lesions were kept under control.
From the early infancy period, the patient started to show motor developmental delay, which was seen in sitting at 1 year and walking at 4 years of age. Delayed speech was also prominent at 2 years of age. There was no history of any seizures. After age 5 years, the skin lesions progressively started to increase, accompanied by lower extremity spasticity and hyperactive deep tendon reflexes in the neurologic examination by a different physician. In this period, the patient was misdiagnosed as having CP in a different outpatient clinic and administered a botulinum toxin type-A injection with slight improvement. Eventually, at age 6 years, a diagnosis of SLS was considered based on dermatologic and neuromuscular findings. A genetic test showed homozygous mutation in the ALDH3A2 gene (c.683 G > A, p.Arg228His), which confirmed the diagnosis.
The patient had a 4-year-old younger sister with a similar clinical history (ichthyosis, spasticity) who could walk independently, and an 18-month-old brother with no obvious musculoskeletal findings in a current examination; genetic tests of both revealed a homozygous mutation. The family reported that her brother had limited ichthyosis and there was a slight delay in motor developmental stages. He had just learned to walk.
On referral to the rehabilitation clinic, the patient was taking acitretin therapy. A skin examination showed more localized ichthyosis that was prominent mainly in the trunk and extremities and spared the face. Pyramidal system involvement signs were found in a neurologic examination. She had grade 2 spasticity in both gastrocnemius muscles and grade 1 spasticity in hip adductors of both limbs according to the modified Ashworth scale, hyperactive deep tendon reflexes in both knees and ankles, and ankle clonus bilaterally. Babinski sign was positive bilaterally. An electrophysiologic examination was performed looking for peripheral neuropathy because mild atrophy was seen in foot intrinsic muscles, but there were no pathologic findings. She was walking dependently but a gross observation of the gait pattern revealed wider steps with a smaller stride length. According to the Gross Motor Function Classification System (GMFCS), she was assessed at level 3. Genu recurvatum was seen at the right stance phase. At the end of the swing phase, initial contact with the ground occurred with the forefoot instead of the heel due to spasticity and weakness of the ankle dorsiflexors. A rehabilitation program scheduled for three times per week included range of motion, stretching, and strengthening exercises for lower extremities in addition to coordination-balance exercises. Solid type AFOs were provided for both limbs. These AFOs were fabricated with high-temperature thermoplastic and designed with both plantar flexion and dorsiflexion control which could be adjusted in the neutral ankle position according to the patient’s needs. It was requested that the AFOs be used as much as tolerated during the day, especially while walking and at night. Additionally, a home exercise program including range of motion and stretching exercises was prepared and explained to the family. After 20 sessions of the rehabilitation program, she started walking independently with the additional contribution of the AFOs. Her parents stated that she fell less due to the improvement in balance. There were no skin lesions caused by the AFOs.
Discussion
As with other rare genetic diseases, there is no definitive treatment for SLS. Beyond symptomatic treatment and increasing independence, quality of life should be the main goal of the rehabilitation physician. Herein, the contribution of a short-term rehabilitation approach and especially the administration of AFOs regarding the independence level of the patient are emphasized. The diagram summarizing the 3-step rehabilitation approach in SLS is shown below (Fig. 1).
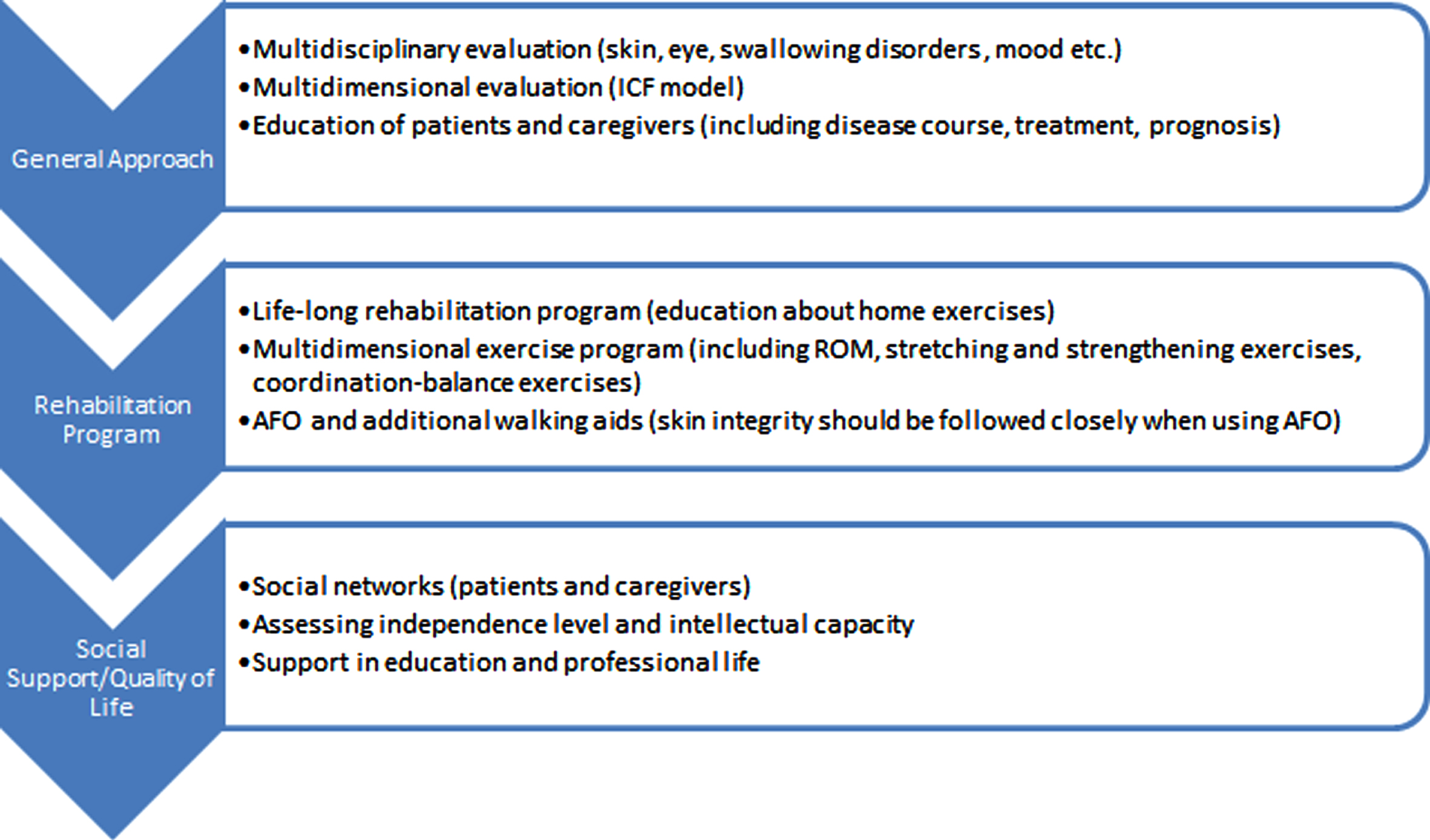
3-step rehabilitation approach in patients with SLS (ICF: International Classification of Functioning, Disability and Health, ROM: Range of motion, AFO: Ankle-foot orthosis).
The observation of many phenotypic and genotypic variations in rare diseases emphasizes the importance of an individual rehabilitation approach. Assessing all aspects of physical and mental health from the perspective of the patient and caregiver is a cornerstone for improving quality of life. Most patients with SLS have activity limitations and restrictions in their participation in society [15]. In a recent study conducted by Staps et al., broader assessments of parents and caregivers were reported via online questionnaires: the most often reported problems were itchy skin, reduced mobility, and dependency; mood problems were rarely mentioned [16]. As supported by these studies, lifelong rehabilitation practices are important for maintaining as much independence as possible in daily living activities. In this case, after the initial rehabilitation program focused on spasticity and gait disorders, an improvement was observed in the gait pattern, balance status, and independence level in daily activities, as supported by the caregivers of the patients. A home program including range of motion and stretching and strengthening exercises, mainly for the lower limbs, and coordination-balance exercises were given to the caregivers of the patient, in addition to using AFOs. The patient was planned to be evaluated at three-month intervals to re-evaluate the neuromuscular findings and update the rehabilitation program because the patient’s age was close to the contracture development age stated in the literature. Detailed observation of the patient in terms of mood, swallowing disorders, and skin and eye findings is important during follow-up because of their high prevalence in the disease course; this requires a multidisciplinary evaluation [16]. It is also important to evaluate siblings in detail during follow-up. A similar rehabilitation program was planned for the patient’s sister, primarily for spasticity. AFOs were not recommended to her sister because they would not provide additional improvement to her gait pattern. A home exercise program that focused on range of motion exercises was given for the brother, who had no musculoskeletal symptoms other than delayed motor developmental stages and, considering his age, was followed closely.
Another important aspect of the rehabilitation approach in this case is the use of AFOs. The prescription of an AFO is common practice in the treatment of patients with neuromuscular disorders, mainly in CP. The main goals of AFO use are to improve overall function and gait quality, reduce energy consumption, maintain correct ankle-foot alignment, and prevent contractures by slowly stretching spastic muscles [17, 18]. In a study conducted with children with diplegic CP, the effect of AFO use on walking parameters was examined and it was found AFOs had a clinically significant effect on stride length and speed [18]. In a comparison of AFO configurations, mainly solid, hinged, and posterior leaf spring, it was shown that all AFO configurations improved the execution of walking/running/jumping skills, upper extremity coordination, and fine motor speed/dexterity [19]. As another important aspect of AFO use, they are intended to have a direct impact on ankle motion, but they are also thought to indirectly influence other joints [20]. Regarding the positive effects of AFOs in this case, the patient achieved the ability to adjust her ankle position during the gait cycle, in addition to controlling the knee position through ground reaction forces during the stance phase of the gait cycle. Eventually, the improvement in balance decreased falls, and the patient started walking independently.
Solid AFOs are preferred because they provide ankle stability more effectively, apply more stretching force to the ankle, and are able to apply secondary corrective force on the knee joint, especially for right genu recurvatum. An objective analysis of gait parameters may be required in future studies to precisely understand its effect. Another point to be emphasized is that the use of AFOs in daily practice should be followed up at regular intervals in terms of skin abrasions and skin infections. Considering patients with SLS, this becomes more important because ichthyosis and secondary skin infections are frequently seen in the course of the disease. If there are such findings in the relevant area, special coatings can be applied inside the AFOs. In addition, care should be taken in terms of infection.
The most important disease to be considered in the differential diagnosis of SLS is CP, the most common cause of motor disability in childhood [1]. Patients with SLS have clinically similar features to patients with diplegic CP in terms of gait pattern, spasticity, and neurodevelopmental delay, eventually leading to misdiagnosis, as in this case. In a detailed physical examination, the cutaneous manifestations made SLS the leading differential. Compared with CP, SLS may show a progressive pattern due to its inherited neurometabolic feature and may lead to contracture development and ambulation loss at an earlier age. Ocular problems and intellectual disorders may be more common in patients with SLS than in diplegic CP. Definitive differential diagnoses can be made using genetic analysis. Regarding treatment modalities, botulinum toxin injection plays an important role in the treatment of spasticity, mainly used in patients with CP. In this case, a botulinum toxin type-A injection was administered to the ankle plantar-flexors previously, but limited functional gain was achieved. Further studies are warranted to understand the effect of botulinum toxin injections on spasticity in patients with SLS.
Beyond the typical features of SLS in physical examinations, its effects on the social life of the patient and caregiver should also be evaluated in detail. Rare diseases may have a greater impact on caregivers than diseases such as CP. Given that SLS is a rare disease, supporting caregivers with the help of social networks and informing them about the prognosis can alleviate their concerns. It should not be forgotten that the patients with SLS need closer support in their education and professional life due to a decrease in the level of independence and deterioration in intellectual capacity. Multidimensional evaluations of the effects of the disease should be performed within the framework of the ICF model [21]. In this case, spasticity and GMFCS evaluations were done for body structure/function and activity domains, respectively. As the most important limitation of this case report, future studies with more systematic evaluations including the participation domain in accordance with the International Classification of Functioning, Disability and Health (ICF) model are needed. The validity of the assessment scales used in diseases such as CP in rare diseases is another limitation.
In conclusion, small touches in rehabilitation medicine can have major positive impacts for patients and caregivers, especially in rare genetic diseases with no definitive treatment. A multidisciplinary approach for complete well-being will reveal more effective results in long-term follow-up. Further assessments with objective measurement in gait analysis are warranted to reach more definitive conclusions.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
Parental verbal and written informed consent as well as informed assent from the child was obtained and approved by the authors’ Institutional Review Board.